35 Years of Exploration, Now a Global Benchmark: How Germany's DRG Payment System Achieves Multi-Stakeholder Balance Between Quality and Cost
Author: Dr. Liu Zhichen, Senior DRG Expert and Postdoctoral Fellow at Fudan University
Germany was the first country in the world to establish a social security system through legislation. Prior to 1993, it primarily adopted a fee-for-service payment model. However, due to the lack of relevant regulatory measures, this led to a rapid increase in healthcare costs. To curb the rapidly rising medical expenses, Germany initiated reforms in health insurance payment methods in 1993, implementing a per-unit-of-service payment system under a global budget framework. Nevertheless, the per-unit-of-service payment approach incentivized healthcare providers to artificially split visits and prolong hospital stays, among other issues, which ultimately drove up healthcare costs and compromised the quality of care.
In 1984, Germany began exploring its own G-DRG payment system by drawing on the DRG payment models of the United States and Australia. In 1997, the German government commissioned the Hospital Association and the Health Insurance Associations to develop the G-DRG system.Although Germany’s DRG payment system drew heavily on the experiences of countries such as the United States and Australia during its development, it has also featured numerous localized innovations tailored to Germany’s specific national characteristics.
Design of a Highly Unified DRG Payment System Framework
Germany’s DRG payment system adheres to a highly unified, top-down design principle, establishing an overall payment framework known as the “321” model.
1. "Three Unifications"
“The Three Unifications” refer to the national standardization of DRG coding, national standardization of weight coefficients, and state-level standardization of base payment rates.
(1) Nationwide Standardization of DRG Coding in China
Germany implements a nationwide uniform DRG coding system, which has been updated annually since the first edition was published in May 2001.
The G-DRG coding system classifies disease diagnoses into 23 Major Diagnostic Categories (MDCs 01–23, including nervous system diseases, respiratory system diseases, digestive system diseases, etc.) and one Pre-MDC (Pre-Major Diagnostic Category).
According to the speech titled “Specific Application of DRGs in German Hospitals” delivered by Wang Qian at the Second National DRG Forum in July 2017, the G-DRG system has undergone 15 version updates since 2003. The number of DRG groups has continued to grow, increasing from 664 groups in 2003, to 824 in 2004, 878 in 2005, 1,192 in 2009, and reaching 1,255 groups in the 2017 version. Among these, there are 1,208 groups for major clinical departments, 42 groups with undetermined weight evaluations, and 5 groups for day-case hospitalization. During this period, the German government has also continuously expanded the scope of data collection and increased the number of special disease groups subject to specific payments.
German DRG codes consist of a four-character alphanumeric code, such as I10A or L33Z. The first letter represents one of the 24 Major Diagnostic Categories (MDCs). The two digits denote subcategories within the MDC. The fourth character indicates a base DRG stratified by resource consumption, with five levels: A signifies very high resource utilization; B signifies relatively high resource utilization; C signifies moderate resource utilization; D signifies lower resource utilization; and Z indicates that no severity level is assigned to that group.
The coding system used in G-DRG includes ICD-10 diagnostic codes, procedure codes, and DRG-specific codes. Hospitals input inpatient information into a unified ICD-10 coding system, which is then automatically converted into DRG codes based on the ICD/OPS mapping system and certain DRG-specific codes (such as AO codes for orthopedics), as illustrated in Figure 1.
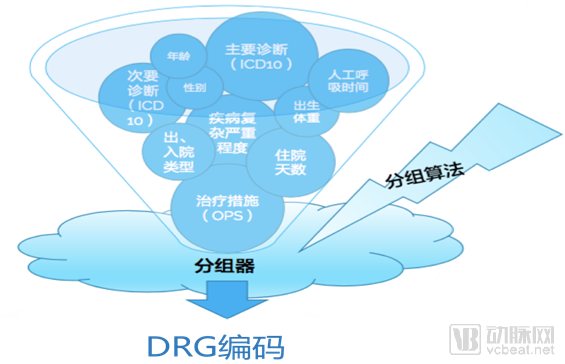
Figure 1. Process of Generating German G-DRG Codes
(2) National Uniformity of DRG Weight Coefficients
When implementing the G-DRG system, Germany established an independent entity, InEK, to determine the relative weights for each DRG group and to regularly revise these weight values. The weights themselves reflect the relative relationship between diseases in terms of resource consumption and medical complexity, with their calculation based on actual cost data. Germany’s cost accounting methodology employs a highly precise bottom-up allocation approach, enabling accurate estimation of the cost per service for each patient. In 2017, the number of sample hospitals participating in cost data collection in Germany reached 245, covering 4.3 million cases.
Meanwhile, to ensure the accuracy of cost data, InEK conducts plausibility checks and extensive consistency audits on the cost data, removing any unreasonable entries. Ultimately, InEK calculates the relative weight coefficients based on calculation rules agreed upon by health insurers and hospitals, and adjusts them annually in accordance with changes in actual costs.
(3) Uniform Base Payment Standards Across All States
The fundamental principle established by Germany’s DRG payment system is that the payment standard for the same disease should be consistent. As previously mentioned, this followed a nine-year transition period. Starting in 2010, Germany implemented a uniform base rate across all federal states nationwide. In 2010, the G-DRG system defined a total of 1,154 DRG groups, each subdivided into several severity levels, with clearly specified reimbursement standards. Although these reimbursement standards were determined independently by each state, the variations were minimal. By 2015, the state-level base rates converged toward a nationally unified payment standard. As shown in Figure 2, the differences in base rates among Germany’s 16 federal states (listed in the leftmost column) were negligible. This occurred because the base rates set by each state were based on a federal benchmark rate of €3,376, with an upper limit of €3,460 and a lower limit of €3,341; however, actual rates were adjusted according to local circumstances. Consequently, the base rates in all states fell within the range of €3,341 to €3,460.
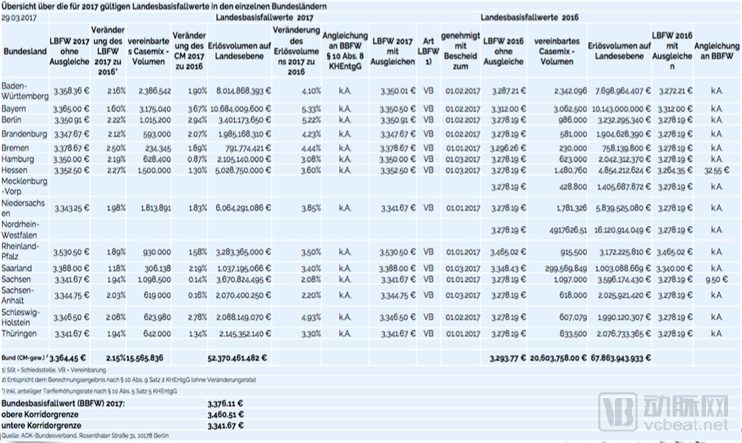
Figure 2. Basic Rates by State in Germany’s G-DRG System, 2017
2. “Two Full Coverages”
Since 2009, Germany has implemented a policy of mandatory universal health insurance, requiring all residents to enroll in either statutory health insurance or private health insurance. By 2015, the health insurance coverage rate in Germany had reached 100%, with 86% of residents participating in the statutory health insurance system, 11% opting for substitute private health insurance, and approximately 3% comprising military personnel and police officers covered under special programs. Government regulations grant insured individuals the right to claim reimbursement for services including disease prevention, early diagnosis, treatment, and rehabilitation management.
To align with the aforementioned system and better mitigate potential negative impacts of DRG-based payment on patient or case selection, Germany established the principle of “two comprehensive coverages” upon implementing the DRG payment system: in terms of scope of application, the DRG system covers nearly all patients; in terms of disease categories, it covers almost all conditions except mental disorders, with special payment arrangements limited to a few specific conditions such as hemodialysis. Starting in 2013, Germany promulgated and piloted the Regulation on the Flat-Rate Payment System for Psychiatric and Psychosomatic Facilities (Verordnung zum pauschalierenden Entgeltsystem für psychiatrische und psychosomatische Einrichtungen, PEPPV), formally introducing the DRG payment model into mental health care services and conducting annual updates and maintenance of payment standards.
3. “A Separation”
Germany's G-DRG coding system adopts a separation of surgical and medical specialties in the design of disease classification and coding. The middle two digits of the G-DRG code consist of numerical codes ranging from 01 to 99, where 01–39 represent surgical cases, 40–59 represent other cases, and 60–99 represent medical cases.
The steps for generating G-DRG codes are as follows:
Step 1: Determine the MDC grouping based on the principal diagnosis;
Step 2: After determining the MDC group, assign the case to a surgical group, medical group, or other group based on whether an operating room is required.
Step 3: If surgery is not performed, diseases are first classified based on the principal diagnosis to determine the base DRG code. The patient’s clinical severity level is then determined based on factors such as the severity of comorbidities or complications, ultimately establishing the final DRG code for reimbursement purposes. The Patient Clinical Complexity Level (PCCL) is generally determined by the severity of comorbidities or complications, gender, age, average length of stay, and other factors. Clinical severity levels are divided into five categories, represented by the numbers 0–4. Typically, patients with a PCCL of 0 or 1 are assigned to the same DRG code. A PCCL of 2, 3, or 4 indicates that the severity of comorbidities or complications is sufficient to increase the hospital stay by 3–4 days for more than 75% of patients, resulting in assignment to a different DRG.
Step 4: If surgery is performed, determine the surgical procedure code based on the type of surgery (e.g., cholecystectomy, biopsy, or endoscopy). The OPS 3.1 version is used for surgical procedure coding. If multiple procedures are performed, assign the patient to the corresponding surgical DRG based on the level of surgery (classified as major surgery, minor surgery, and others), as shown in Figure 3.
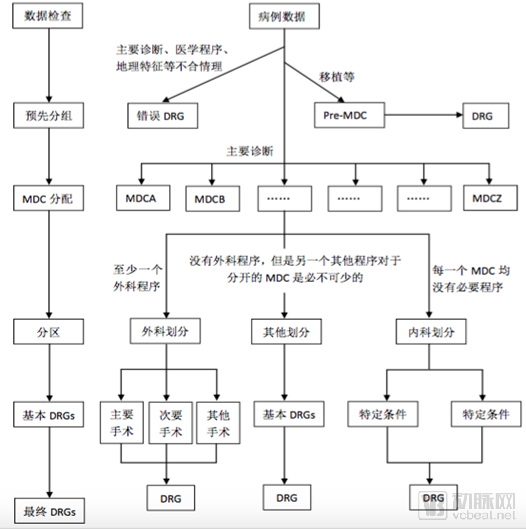
Figure 3. The German G-DRG grouping process reflects the characteristic separation of medical and surgical cases
Integrating with Social Governance to Strengthen a Sustainable Payment System for Self-Management
Li Zhen and Zhao Qing (2015) argue that the governance structure of Germany’s statutory health insurance system is a framework centered on social governance, organically integrating government and societal oversight. Within this system, the boundaries of governmental responsibility are clearly defined: the government is tasked with policy implementation and regulation within the basic legal framework. Meanwhile, self-governing social entities—namely health insurers, physicians, hospitals, and their respective associations—operate under the principles of “autonomy and partnership.” Through equal consultation, negotiation, and strategic interaction, these stakeholders address key governance areas such as financing, benefit coverage, and fund management to achieve an internal balance of interests. Ultimately, they work toward a shared health policy objective: “maintaining and restoring the health of insured individuals or improving their health status,” as illustrated in Figure 4.
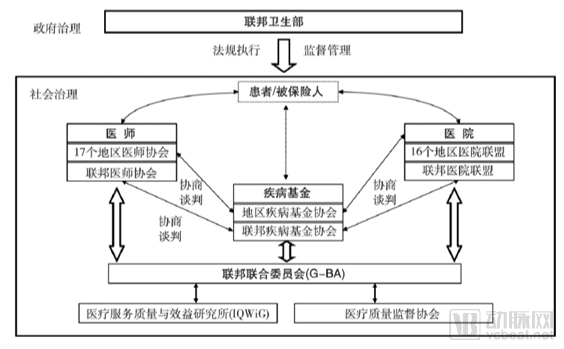
Figure 4 Governance System of Germany’s Statutory Health Insurance Scheme
1. Government governance primarily focuses on regulatory formulation, enforcement, and oversight
In the design of the DRG payment system, the government does not directly engage in the specific operational affairs of the social health insurance system; instead, it focuses its role on the formulation, implementation, and supervision of relevant policies. Regulations concerning insured populations, the scope of health insurance coverage, financing, and the operations of disease fund associations are updated and revised continuously to adapt to the evolving needs of economic and social development.
In 2009, to facilitate the full implementation of the Diagnosis-Related Groups (DRG) payment system in Germany, the German government introduced a mandatory universal health insurance policy and established clear regulations for the standardized operation of sickness funds. It also implemented a rigid national global budgeting system, under which total healthcare expenditures and health insurance contribution rates were determined by the Bundestag (German Parliament). Furthermore, a nationwide risk adjustment mechanism was established to balance risks among different sickness funds within a unified framework (as shown in Figure 5). The introduction of these systems laid a solid foundation for the successful nationwide rollout of the DRG payment system.
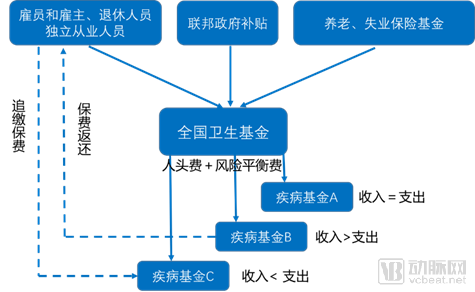
Figure 5 German Sickness Funds and Risk Structure Compensation Mechanism
As the statutory representative body for government governance, the German Federal Ministry of Health assumes responsibility for issuing, enforcing, and supervising laws and regulations during the implementation of the Diagnosis-Related Groups (DRG) payment system. Since the rollout of the DRG payment system, it has issued a series of laws, regulations, and policy documents to ensure the smooth operation of DRG-based payments and achieve the desired outcomes.
2. Social governance is primarily based on self-management within autonomous entities
The core of Germany’s statutory health insurance system lies in strengthening social governance capacity, characterized by the balance of interests within governance entities and among various social stakeholders. In advancing the Diagnosis-Related Group (DRG) payment system, Germany has consistently applied the principle of “autonomy and partnership.” Healthcare providers, insurers, patients, and their respective associations achieve self-management and sustainable operation of the DRG payment system through self-governance within autonomous entities and negotiations between them.
(1) Main Administrative Bodies of G-DRG and Their Functions
As previously introduced, the DRG payment system is a complex systematic project. To this end, G-DRG has established a specialized management body based on various autonomous entities (industry associations) to provide professional management and organizational assurance for the overall operation and implementation of the G-DRG payment system.
Taking InEK, the statutory governing body for G-DRG, as an example, the institution is jointly composed of the Association of Statutory Health Insurance Funds, the Association of Private Health Insurers, and the German Hospital Federation, representing the interests of statutory health insurance funds, private health insurance companies, and hospitals, respectively. Together, they form a sustainable, association-led self-governance mechanism for the German G-DRG system. Its core functions primarily include DRG definition, grouper certification, data collection and analysis, formulation and updating of grouping and coding rules, and calculation of relative weights.
InEK has developed the following auxiliary tools during its development and construction process, which are provided for hospital use and updated annually.
DRG Agreement
DRG agreements are standardized protocols governing administrative procedures for general matters, such as the management of readmission cases, patient referral processes within hospitals, and the handling of case-related medical expenses during annual transitions.
DRG Payment Catalog
The DRG payment catalog includes 1,255 DRG items (based on the 2017 version of the G-DRG system, with the number of DRG groups in the DRG item table updated annually), expenditure weight values, and average length of stay (including data such as minimum, median, and maximum values). DRG reimbursement is calculated based on factors such as the average length of stay and expenditure weight values.
See Figures 6 and 7 for details on the generation process of Germany’s uniform annual DRG payment catalog and examples of the payment catalog. Currently, each hospital in Germany conducts internal cost analyses and submits these data to InEK. InEK then processes all submitted data through case-mix adjustment, structural data reconciliation (including data supplementation), to produce the uniform annual DRG payment catalog. This lifecycle spans two years.
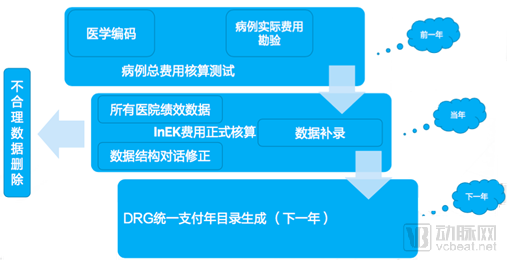
Figure 6 Generation Process of the G-DRG Unified Annual Payment Catalog
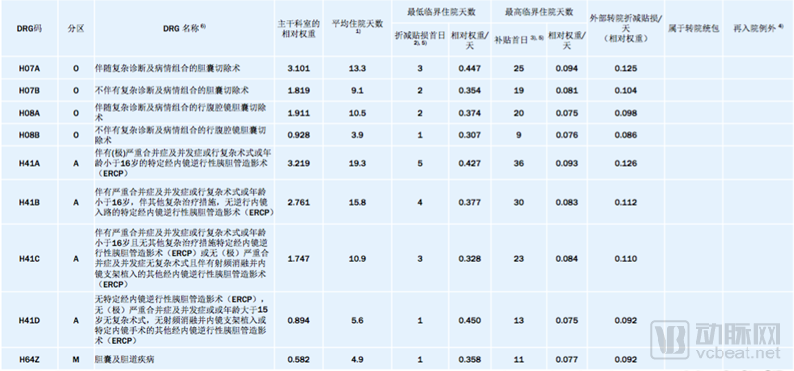
Figure 7. Examples of the Reimbursement Catalog for Common Benign Gallbladder and Biliary Tract Diseases
In addition to the DRG payment catalog, Germany maintains other payment catalogs. These serve as fee schedules for special costs, allowing for additional and supplementary payments for procedures such as renal dialysis, oncology drugs, radiotherapy, and chemotherapy.
In accordance with the Hospital Financing Act (Krankenhausfinanzierungsgesetz, KHG) and the Hospital Remuneration Act (Krankenhausentgeltgesetz, KHEntgG), the total payment amount for each hospital under the G-DRG system is calculated as follows:
Total Compensation = Relative Cost Weight × State Base Rate + Additional Fees + Charges for Excess Length of Stay - Deductions for Short-Stay and Transfer Patients
It also clearly specifies the calculation methods for additional charges and deductions. Specifically, for long-term inpatients, an upper threshold is established for the within-range value; any marginal costs exceeding this upper threshold incur an additional daily compensation fee. For short-term inpatients, a lower threshold is set for the within-range value; if expenditures on major service items fall below this lower threshold, a daily deduction is applied.
Additional payments in the G-DRG system are relatively rare, accounting for only 3.5% of the total volume in 2017. They mainly include outlier cases (additional costs considered outside the DRG distribution); specific performance schemes for surgeries and interventional procedures, medication or blood product management, dialysis, and related operations; as well as new diagnostic and therapeutic methods that are not adequately reimbursed under the DRG system and have not been excluded from DRG funding.
DRG Coding Guidelines
Updates are made annually in conjunction with the G-DRG system. InEK is primarily responsible for establishing coding rules, while the official DRG coding is performed by DIMDI.
Application of NUB
To ensure that new technologies are promptly incorporated into the G-DRG system, InEK has established a “top-up” funding application process known as New Examination and Treatment Methods (NUB). Reimbursement by Statutory Health Insurance (SHI) is contingent upon InEK’s approval and verification that the NUB meets the criteria of necessity, appropriateness, and economic efficiency. Hospitals must apply for reimbursement when utilizing new technologies. Subsequently, InEK conducts monitoring to assess whether DRGs are adequately applied, coding is accurate, and cost variations attributable to new technologies are tracked. The eligibility for NUB reimbursement also depends on the specific assignment of diagnosis and procedure codes.
The specific process is shown in the figure below:
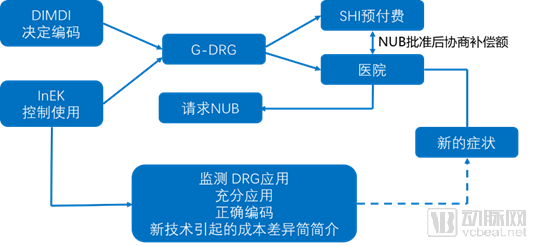
Figure 8 G-DRG Payment Process for Hospitals Adopting New Technologies
(2) Characteristics of Internal Self-Management and Division of Labor Among Highly Autonomous Entities
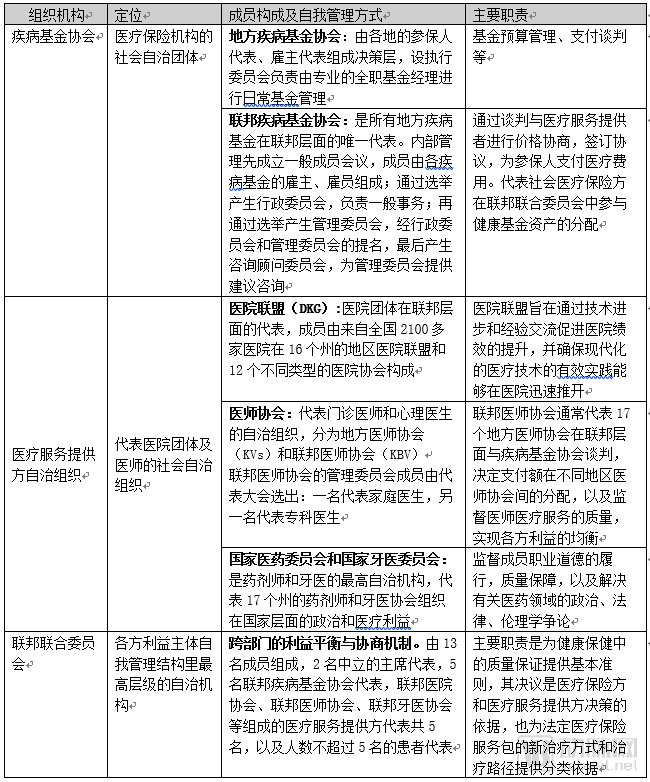
In addition to relying on specialized DRG management agencies established by each autonomous entity, the internal self-governance of various stakeholders within Germany’s statutory health insurance system, as well as the collaborative operational mechanisms among these stakeholders, primarily depend on self-regulation by different industry associations. This reflects a high degree of social autonomy, aimed at achieving a balance of interest structures both within and between associations. Specifically, the characteristics and division of responsibilities regarding internal self-governance among the associations representing the major stakeholders are summarized as follows:
Table 1 Positioning and Division of Labor Among Social Self-Governing Entities Related to the German G-DRG System
(3) G-DRG Payment Mechanism Based on Equal Negotiation Among Autonomous Entities
Germany’s G-DRG system is the primary mechanism for allocating health insurance funds to healthcare institutions, channeling approximately 85% of financial resources annually through this system. Currently, all inpatient hospital payments in Germany are based on the DRG payment model. Data published by InEK in 2016 showed that the G-DRG system facilitated total payments of €70 billion to 1,500 hospitals nationwide, covering approximately 22.1 million patients. This makes Germany one of the countries with the largest scale of DRG-based healthcare expenditure globally.
Germany’s allocation of healthcare costs is not determined empirically; rather, it is established through a highly sophisticated process of empirical cost calculation and negotiation.
Regarding the negotiation mechanism of the G-DRG payment system, negotiations are primarily conducted between the Association of Sickness Funds and hospitals along with their alliance organizations, each representing their respective interest groups. The negotiations focus on two key aspects: reimbursement rates and monitoring of healthcare service quality. If the parties fail to reach an agreement, the Federal Joint Committee shall make the final determination.
The specific negotiation process is shown in the figure below:
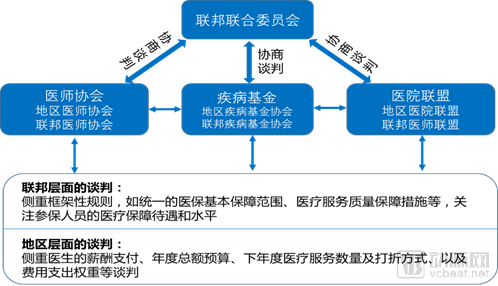
Figure 9 Negotiation Mechanism of the G-DRG Payment System
Furthermore, the establishment of InEK has enabled the German Hospital Federation and the National Association of Statutory Health Insurance Funds to achieve information sharing and communication in technical management. Within an open and transparent information mechanism, the health insurance funds, hospitals, and their associations have achieved an organic balance between controlling healthcare costs and ensuring the quality of medical services through dialogue and negotiation.
It is worth noting that Germany implements a zero-markup policy for pharmaceuticals. Whether for practicing physicians, hospitals, or rehabilitation and nursing care facilities, revenue is derived solely from medical services and is unrelated to drug costs. For all outpatient medication expenses, except for the patient’s out-of-pocket portion, payments are settled directly between health insurance institutions and pharmacies. Inpatient medication costs are accounted for as hospital expenses, with no drug markups applied.
(III) Establish a sound mechanism for DRG cost review and quality supervision
1. Medical Cost Review Mechanism of G-DRG
In Germany, the specialized body responsible for reviewing medical expenses is the Medical Service of Health Insurance (Der Medizinische Dienst der Krankenversicherung, MDK). Its members consist of physicians from healthcare institutions across China that implement Diagnosis-Related Group (DRG) payment systems. As an independent review agency, the MDK’s assessment opinions can serve as a reference for reimbursement. The federal-level review body is known as the Medical Advisory Services (MDS), which primarily provides consultation for statutory health insurance at the federal level, coordinates and supports collaboration among various MDKs, and establishes guidelines for standardization of reviews and professional training. The MDK is also required to assist the MDS in fulfilling its tasks.
(1) Review of Materials
The review materials for DRG cases by the MDK mainly include: hospital discharge data such as basic information (name, admission and discharge dates, length of stay, admission condition, discharge condition, diagnosis codes, and procedure codes); DRG data such as DRG code, MDC, major comorbidities/complications, base rate, and claimed amount; discharge summary; discharge report and partial medical records; complete medical records (sent to the MDK office).
(2) Key Points for Review
MDK’s key review focus areas for DRG cases primarily include whether the length of stay falls within the upper and lower limits, significant comorbidities/complications, principal and secondary diagnoses, accuracy of diagnosis and procedure codes, duration of mechanical ventilation, correctness of DRG coding, and additional reimbursement items.
(3) Tiered Review
Level 1 Review
Level 1 review, also known as ultra-short expert opinion (ultra-short review), involves the random selection of cases by the Statutory Health Insurance (SHI) funds. Based on hospital discharge records, SHI personnel and physicians from the Medical Service of the Health Funds (MDK) determine which cases require professional review. The Level 1 review is conducted by offices subordinate to the SHI funds. If there are no objections to the review results, the entire review process is concluded without any further steps.
Level 2 Review
Level 2 review, also known as short expert opinion (short review), utilizes hospital discharge data and discharge reports, and may also incorporate parts of the medical record as review data. The review is conducted by the offices of the Health Insurance Funds Association, with personnel from the Medical Service Review Board (MDK) responsible for handling the process. If necessary, healthcare providers are required to provide explanations to the personnel of the Health Insurance Funds Association.
Third-Level Review
Level 3 review, also known as the extensive expert opinion (extensive review), involves the utilization of all available data, including discharge summaries and complete medical records, and is conducted either at the MDK’s office or on-site at the hospital. Although not every medical expense requires a Level 3 review by the MDK, every medical bill undergoes a rigorous and close scrutiny process.
As shown in Figure 10:
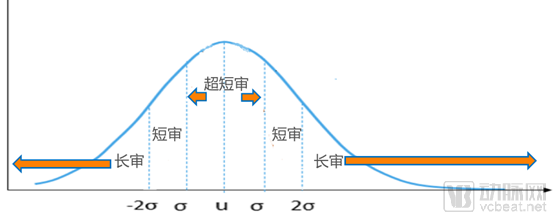
Figure 10. Tiered Review Mechanism for Cost Supervision under the G-DRG Payment System
2. Medical Quality Supervision System of G-DRG
As a payment system, Diagnosis-Related Groups (DRGs) may incentivize healthcare institutions to prioritize cost containment at the expense of medical quality. To effectively mitigate quality-related risks, Germany’s G-DRG payment system has established a comprehensive medical quality supervision mechanism. Germany established the Institute for Quality and Efficiency in Health Care (IQWiG), which is specifically responsible for implementing clinical effectiveness assessments and quality oversight, as well as providing recommendations for DRG-based payments.
Specifically, it mainly includes the following major aspects:
(1) Promoting the development of medical quality supervision through statutory legislation
(2) Fully leverage the self-regulatory role of the medical professional community in the oversight of healthcare quality
(3) Develop a quality grouper specifically for quality control and measurement, along with an inpatient quality indicator system
(4) Release Hospital Quality Report
(5) Consolidate cases to prevent a single patient from being fragmented into multiple hospitalizations
(6) Prevention of Medical Errors
(4) The design of dual hospital financing and the policy separating drug prescribing from dispensing facilitates the smooth implementation of the DRG payment system.
Public hospitals in Germany operate under the "Hospital Financing Act" of German federal law, adopting a "dual financing" model, whereby investment costs and operating costs are reimbursed separately. Investment costs refer to expenditures on facilities with a useful life exceeding a certain period, such as infrastructure construction and renovation, procurement of large- and medium-sized medical equipment, and expenses related to mergers and acquisitions. Operating costs refer to expenditures incurred in hospital operations, including personnel costs (primarily compensation for medical and nursing staff), consumables, and other expenses.
Investment costs are allocated by the government through budgetary appropriations, while operating costs are covered by statutory health insurance funds via Diagnosis-Related Group (DRG) payments. This dual financing model, on the one hand, ensures that public hospitals receive stable government fiscal support, thereby enabling them to better fulfill their social responsibilities; on the other hand, it leverages social health insurance to fund services provided by healthcare institutions, allowing them to respond promptly to market demands.
To ensure the effective implementation of the system, a strict accountability framework has been established linking the dual financing model of public hospitals with hospital planning. Public hospitals are eligible for government fiscal subsidies and reimbursements from statutory health insurance only if their institutional setup, equipment procurement, and operational costs comply with state government hospital plans. If healthcare institutions violate planning requirements by exceeding bed capacity controls or surpassing their authorized scope of services, their funding will be reduced as a penalty. Hospital planning exerts strong constraints on the allocation of medical resources within a region, and this robust accountability mechanism promotes orderly competition and development among hospitals.
Meanwhile, implementing Diagnosis-Related Group (DRG)-based payment is not only a cost-containment strategy but also a significant mechanism for introducing pricing reforms. This approach enhances transparency in hospital service scope and pricing, thereby incentivizing hospitals to improve their technical efficiency.
In addition, German hospitals implement a separation between medical services and pharmaceutical sales. Drug costs in hospitals are primarily derived from inpatient pharmacies and are already included in the Diagnosis-Related Group (DRG) payments. Therefore, whether public or private, the primary cost component for hospitals is personnel expenses, accounting for more than 60% of total costs, while the proportion of drug costs is relatively low. There is no issue of cross-subsidizing medical services with drug revenues (as shown in Figure 11).
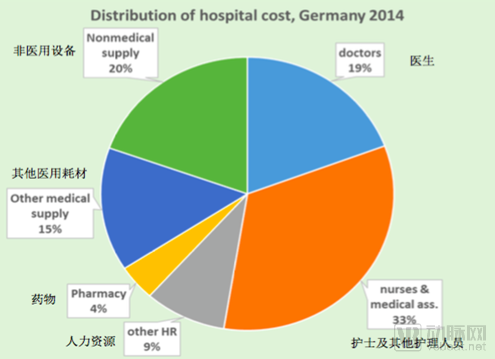
Figure 11 Cost Distribution in German Hospitals
The Effectiveness of Germany's DRG Payment Reform
The primary objectives of implementing the German G-DRG system are to enhance the internal and external comparability of inpatient services, improve performance-based reimbursement mechanisms, allocate financial resources more effectively, leverage additional profit reserves (through reduced length of stay and optimized operational and organizational structures), and reduce hospital expenditures.
Overall, German practice has demonstrated that the DRG payment system balances the interests of multiple stakeholders—including the government, hospitals, and patients—while achieving a reasonable equilibrium between healthcare quality and costs. Over a nine-year transition period, Germany standardized base rates across all states nationwide. Following the implementation of the DRG payment system, the average length of stay in 750 pilot hospitals decreased by 30%. The German DRG payment system has shifted hospital revenue strategies, positioning health insurance institutions as overall controllers of healthcare expenditures and as patient advocates. This has helped curb supplier-induced demand to some extent and encouraged hospitals to minimize patients’ length of stay.
The implementation of the Diagnosis-Related Groups (DRG) system has, to some extent, slowed the growth rate of medical expenses due to shortened hospital stays and strengthened cost management by hospitals. By standardizing the management of healthcare institutions and health insurance agencies on a unified information platform, the DRG system facilitates clinical communication, comparison, and improvement of treatment processes, thereby enhancing the quality of medical services to a certain degree. Studies have shown that the adoption of the DRG payment system in Germany did not lead to a decline in medical quality; overall, the average quality of medical care in Germany is comparable to that in the United States, while expenditure is only half that of the U.S. (Thomas Mansky, 2016). Furthermore, the DRG payment system incentivizes hospitals to proactively reduce costs to generate profits, encouraging greater attention to cost-effectiveness in the procurement of pharmaceuticals, medical supplies, and equipment, as well as in the utilization of medical resources and clinical practices, thus promoting hospital cost accounting to a certain extent.
Consequently, the implementation of this payment system has forced some medical institutions unable to proactively adapt to withdraw from industry competition, while a large number of private hospitals have thrived due to their competitive advantages, giving rise to large private hospital groups such as HELIOS and Asklepios. In response to the challenges posed by DRG-based payments, many hospitals have successively implemented a series of management reforms after adopting the Diagnosis-Related Groups (DRG) system.
References:
1.Zhou Yu, Zheng Shuzhong, Sun Guozhen. Germany's DRG Payment System [J]. China Health Resources, 2004(5):139-141.
2.Wang Qian. Specific Application of DRG in German Hospitals [R]. Speech delivered at the Second National DRGs Forum, July 2017.
3.Heimig, F. Experience and Lessons from the Implementation of G-DRG in Germany: What Are the Key Factors for Success [R]. Speech delivered at the China DRG Payment Conference, September 14, 2017.
4.Li Zhen, Zhao Qing. Experience and Implications of the Governance System and Mechanism of Germany’s Social Health Insurance [J]. German Studies, 2015, 30(2): 96.
5.Chang Feng, Ji Meiyan, Lu Yun. Germany's G-DRG Health Insurance Payment System and Its Implications for China [J]. Chinese Health Economics, 2016(6):92-96.
6.Busse R, Riesberg A.Health care systems in transition: Germany[R].Copenhagen: WHO Regional Office for Europe, 2004.
7.Klein-Hitpa U, Scheller-Kreinsen D. Policy trends and reforms in the German DRG-baded hospital payment system[J]. Health policy, 2015, 119(3): 252-257.
8.Wu Qifei, Ma Liping, Liang Minghui. Review of the German Medical Quality Supervision System [J]. Chinese Hospital Management, 2010(10):21-24.
9.Chen Yao, Zhang Changkuan, Ma Xiaojing. Research on the Financing and Operation Models of Public Hospitals in Germany[J]. Medicine and Society, 2014, 27(11): 40-43.
10.U.S.Congress, Office of Technology Assessment. Hospital Financing in Seven Countries[R].Washington, DC:U.S. Government, Printing Office,1995.
11.Thomas Mansky. The German DRG Reimbursement System [R]. Speech delivered at the Beijing DRG Academic Exchange Conference on November 12, 2015.
Copyright Statement:
Most of the views expressed in this article are based on the postdoctoral research findings of Dr. Liu Zhichen, published with authorization from VCBeat. The cited articles and viewpoints reflect those of their respective authors as obtained from publicly available sources. Unauthorized reprinting, excerpting, copying, mirroring, or any other form of use is strictly prohibited.
Author Introduction:

Chief Expert in the Healthcare Sector, Industrial Internet Product Center, China Unicom Group.
Postdoctoral Fellow, Fudan University Postdoctoral Mobile Station in Public Administration; Postdoctoral Fellow, National Health and Family Planning Commission Statistical Information Center Postdoctoral Workstation. Senior Strategic Expert in the Greater Health Sector.
With nearly a decade of strategic consulting experience in the internet healthcare and broader health industry, I previously served as the Director of Strategic Consulting and R&D Business Development at a leading domestic listed IT solutions and services provider. In this role, I spearheaded the planning of numerous forward-looking, innovative business models for the health sector. Notably, I presciently predicted that reforms in China’s medical payment systems, particularly the adoption of Diagnosis-Related Groups (DRG), would become a pivotal initiative in deepening healthcare reform during the 13th Five-Year Plan period. As the overall project lead, I participated in a pilot project for DRG-based medical insurance payment reform in a prefecture-level city in China. I assisted the municipal Healthcare Security Administration in designing the top-level framework for the citywide DRG payment system reform and facilitated the implementation of supporting information technology systems.