OncoVent Bio Announces Breakthrough in Ovarian Cancer Immunotherapy with SOC-Combined Neoantigen Vaccine Oregovomab
Dr. Laurie H. Glimcher, a renowned immunologist, once described the challenge of traditional immunotherapies in treating cold tumors as follows: “Cold tumors are like castles surrounded by moats. T cells are blocked by the moat from attacking the castle, while few T cells are present inside the castle. Consequently, checkpoint inhibitors may be less effective against cold tumors than against hot tumors.”
"Cold tumors" primarily refer to those lacking a pre-existing immune response, characterized by scant intratumoral T cells. In contrast, "hot tumors" are infiltrated with abundant T cells and currently represent the primary candidates for immune checkpoint inhibitor therapy and combination regimens.
However, to date, only eight types of tumors—bladder cancer, head and neck cancer, kidney cancer, liver cancer, melanoma, non-small cell lung cancer, and tumors with microsatellite instability (MSI) characteristics—are considered “hot.” This implies that patients with other cancer types cannot benefit from conventional immunotherapy. In the realm of “cold” tumors, such as gastrointestinal cancers, glioblastoma, ovarian cancer, prostate cancer, and pancreatic cancer, the lack of a basic immune response results in very low efficacy of immune checkpoint inhibitor therapies (e.g., PD-1/PD-L1 inhibitors). Moreover, these treatments may even interfere with T-cell function and cause adverse effects.

Dr. Shi Yuenian, Co-founder and CEO of OncoVent
Dr. Shi Yuenian, Co-founder and CEO of OncoVent, stated bluntly: “The pain points of first-generation tumor immunotherapies targeting PD-1/PD-L1 have revealed the focal point for next-generation tumor immunotherapies—how to enhance the primary immune response in cancer patients?”
A vivid way to understand this is: how can “cold” tumors be turned “hot”? This is currently a hot topic in the field of cancer therapy. Dr. Shi introduced to reporters several common methods for enhancing the body’s immune response:
First, a small number of autologous T cells are directly extracted from cold tumors, extensively expanded ex vivo, and then infused back into the patient to enhance the immune response. Although this approach is theoretically the most suitable for treating cold tumors, its commercialization remains limited due to the complexity of its operational procedures.
Second, identifying neoantigens for cold tumors. During tumor progression, antigens develop immune tolerance. If these antigens undergo mutation, they may become neoantigens, which can reactivate the immune response. However, tumor antigen mutations are random and uncontrollable, and such mutations do not necessarily result in the generation of neoantigens.
OncoVent is targeting a second approach to turning “cold” tumors “hot,” seeking new immune targets—namely, neoantigens—for ovarian cancer patients. Unlike conventional neoantigens arising from gene mutations, OncoVent artificially intervenes in tumor antigens that have already established immune tolerance through non-humanized “expression.” Dr. Shi further explained, “In combination with first-line chemotherapy agents, we enable fully murine antibodies to bind to tumor antigens, forming antigen–antibody complexes. This imparts foreignness to the original antigens, inducing alterations that generate neoantigens, thereby triggering an immune response and reactivating the immune system.”
Traditionally, neoantigens are generated by mutations. OncoVent has redefined “Neoantigen” to encompass a broader category; specifically, its “Neoantigen” refers to an antigen-antibody complex with murine-derived properties. This approach differs significantly from conventional tumor therapies that target specific druggable pathways. Explaining the origin of this therapeutic strategy, Dr. Shi stated, “This was partly due to historical circumstances. Over a decade ago, during Phase III clinical trials, there was limited understanding of how to design clinical protocols in the field of immuno-oncology (IO). We revisited previously failed clinical projects to analyze the reasons for their failure. Through the design of Phase IIA clinical protocols, we embarked on the path of developing tumor vaccines.”
Oregovomab is OncoVent’s flagship product, licensed from OncoQuest Inc., with exclusive commercial rights in Greater China. Leveraging the “neoantigen” principle, OncoVent has initiated multiple R&D pipelines for cancer vaccines (as shown in the figure below).
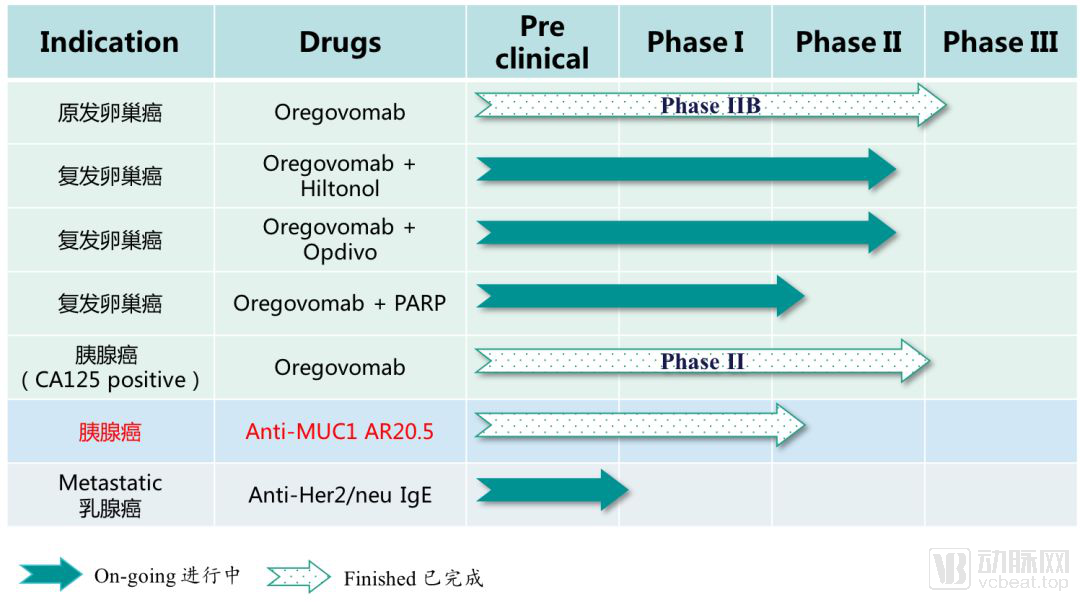
OncoVent's R&D Pipeline
Among these, OncoVent’s most advanced pipeline is Oregovomab for the treatment of primary ovarian cancer. Oregovomab is a high-affinity monoclonal antibody (Mab B43.13) that binds to the ovarian cancer antigen CA-125, thereby initiating a series of immune responses against this antigen.
CA-125 is a glycoprotein specifically expressed on the cell membrane of ovarian cancer cells and is widely used as a prognostic marker for ovarian cancer. Although CA-125 does not normally trigger an immune response in patients with ovarian cancer, OncoVent has “redefined” CA-125 by treating it as a novel “immune checkpoint,” endowing it with “new characteristics” to induce an immune response.
This approach to endowing CA-125 with new characteristics is achieved through the tumor vaccine Oregovomab. OncoVent combines murine antibody Xenotypic IgG1 with the tumor antigen CA-125 to form an antigen-antibody complex. This complex, known as a neoantigen, exhibits enhanced immunogenicity, thereby activating the immune system. Another innovation of Oregovomab lies in its murine origin; upon administration, it induces a human anti-mouse antibody (HAMA) response, which rapidly activates the human immune system. The "foreignness" of the murine antibody acts similarly to an immune adjuvant.
OncoVent and OncoQuest INC. have observed in clinical practice that Oregovomab must be combined with first-line chemotherapy regimens (standard of care, SOC) to significantly improve therapeutic outcomes in ovarian cancer. Dr. Shi explained, “Preclinical and clinical data have demonstrated that chemotherapy can moderately alter the tumor microenvironment and may also modify tumor surface antigens. SOC regimens, such as carboplatin/paclitaxel, kill a portion of tumor cells, leading to the shedding of CA-125 and facilitating its interaction with Oregovomab to form neoantigens.”
Currently, OncoVent and OncoQuest INC. have completed the Phase IIb clinical trial of Oregovomab. A total of 97 patients with newly diagnosed advanced ovarian cancer with metastasis were enrolled. The study included a Phase IIb experimental group of 47 patients (SOC + Oregovomab) and a control group of 50 patients (SOC). In the experimental group, Oregovomab was administered concurrently with chemotherapy during the 1st, 3rd, and 5th cycles at a dose of 2 mg per patient per administration. An additional dose was given after the completion of the final chemotherapy cycle, resulting in a total cumulative dose of 8 mg per patient. Patients were then observed for 36 months without further dosing.
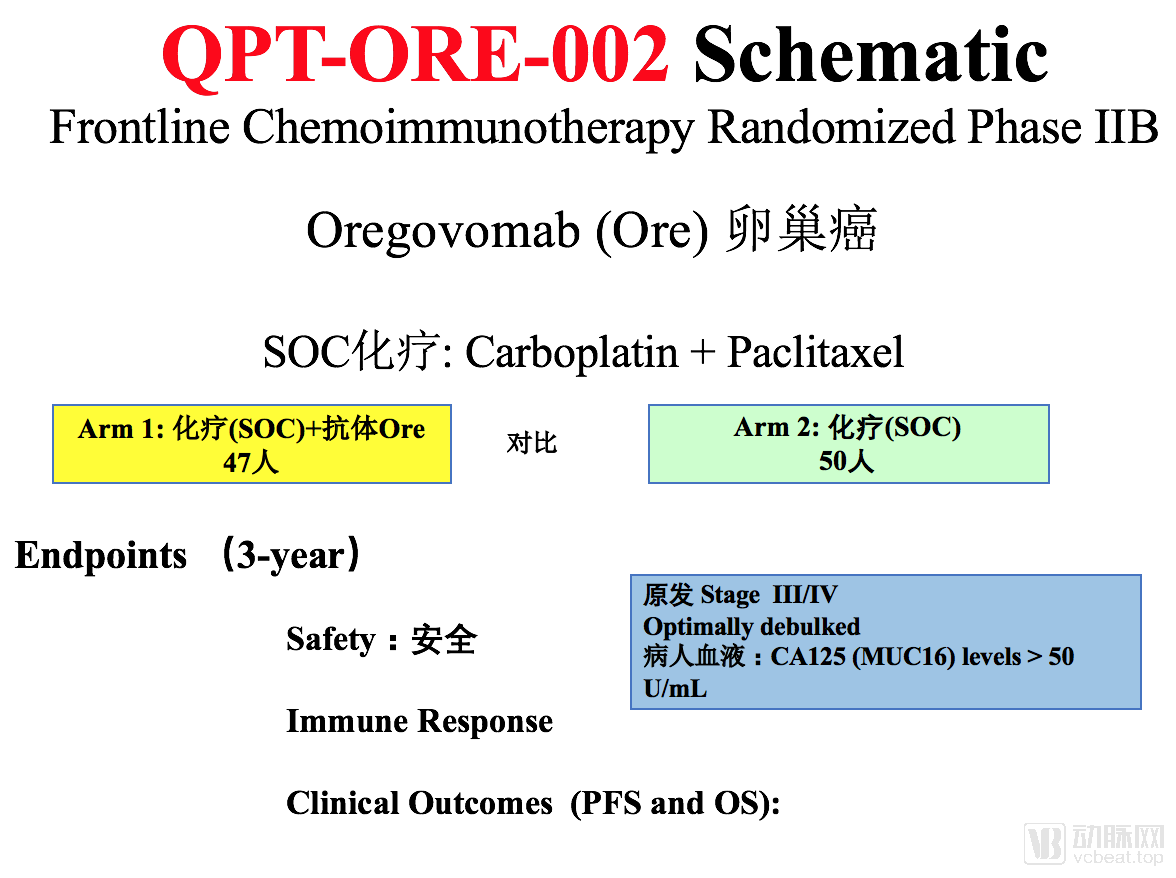
Phase IIb Clinical Trial Design of Oregovomab
Phase IIb clinical trial results demonstrated that Oregovomab combined with standard of care (SOC) yielded significantly improved clinical efficacy. The progression-free survival (PFS) in the experimental group was 41.8 months, compared to only 12.2 months in the control group, representing a approximately 3.5-fold increase in PFS for the experimental group relative to the control group.
Currently, OncoVent and OncoQuest INC. are initiating a Phase III clinical trial for first-line treatment of primary ovarian cancer, planning to enroll over 500 newly diagnosed patients with advanced ovarian cancer worldwide to further evaluate the progression-free survival (PFS) in patients receiving Oregovomab plus standard of care (SOC) versus those receiving SOC alone.
When used in combination with first-line chemotherapy, Oregovomab has the potential to become a first-line treatment for ovarian cancer. In contrast to Olaparib, an approved oncology drug on the market that requires patients to have achieved a complete or partial response to standard of care (SOC) before initiation, Oregovomab is not subject to this restriction and can be directly combined with SOC without any known side effects. Conversely, Olaparib cannot be administered concurrently with SOC and is associated with adverse effects such as neutropenia.
Furthermore, Oregovomab differs from traditional targeted therapeutic agents in that it is designed to stimulate the body to generate new antigens rather than block specific targets. Consequently, a dose of only 2 mg per injection is sufficient to achieve therapeutic efficacy. In contrast, Opdivo, a drug developed targeting PD-1, requires a dosage of 500 mg per injection, which is more than one hundred times the dose of Oregovomab.
In addition to the core pipeline asset Oregovomab, another oncology drug in clinical development is BrevaRex monoclonal antibody. This agent is indicated for the treatment of malignant tumors expressing the MUC1 tumor antigen and has completed its FDA Phase I clinical trial. In the FDA Phase I clinical trial, BrevaRex monoclonal antibody demonstrated favorable tolerability and was able to activate MUC1-specific T cells. A Phase II clinical trial for BrevaRex is planned to commence next year.