Integration of CDSS and MDT: A New Paradigm for Intelligent Diagnosis and Treatment of Hepatobiliary Tumors

Yidu Cloud
Medical Big Data Platform
With the advent of the artificial intelligence era and the evolving landscape of medical concepts, intelligent diagnosis and treatment of diseases have gradually become a prevailing trend.
Establishing Clinical Decision Support Systems (CDSS) and Multidisciplinary Team (MDT) models is a crucial measure to improve medical efficiency and quality. As a healthcare artificial intelligence company, Yidu Cloud provides more reliable support and assurance for the informatization construction of China's healthcare system. With the support of the key special project "Precision Medicine Research" under the National Key R&D Program, Peking University Health Science Center and the Fifth Medical Center of PLA General Hospital took the lead, joining forces with experts from the CSCO Liver Cancer Committee and the Asia-Pacific Alliance for Liver Disease Technology/Hepatobiliary Tumor Expert Committee, together with Yidu Cloud, to jointly create a national AI-powered multidimensional MDT collaboration platform for hepatobiliary tumors. This platform leverages AI technology to provide intelligent clinical decision support for hepatobiliary tumors, thereby promoting the intelligent diagnosis and treatment of these diseases and further enhancing the efficiency and quality of medical services. By integrating clinical information from hospital information systems and deeply developing artificial intelligence technologies, the combination of CDSS and MDT is poised to become a new model for the intelligent diagnosis and treatment of hepatobiliary tumors.
Source: Journal of Clinical Hepatology, Vol. 35, No. 10
The current state of healthcare in China remains concerning. Overall, issues such as insufficient total medical resources, their uneven distribution, and variable medical quality remain prominent. Meanwhile, the country is characterized by an aging population and a year-on-year increase in the incidence of chronic diseases and cancers, making it urgent to transform and upgrade healthcare service models [1]. With the advent of the big data era and the evolution of medical concepts, intelligent diagnosis and treatment of diseases have gradually become a prevailing trend [2].
In April 2018, the Chinese government issued the “Guiding Opinions on Promoting the Development of ‘Internet + Healthcare’,” establishing a favorable platform for the comprehensive sharing of medical information and technology, thereby facilitating innovative development in “Internet + Healthcare” [3]. Against this backdrop, a pressing challenge in the healthcare sector is how to fully unlock the value of big data in healthcare, leverage big data technologies to accelerate the intelligent transformation of disease diagnosis and treatment, and improve the quality of medical services. Clinical Decision Support Systems (CDSS) and Multidisciplinary Team (MDT) models are important measures for enhancing medical efficacy. This article reviews the characteristics and limitations of CDSS and MDT systems both domestically and internationally, proposes a vision for integrating CDSS with MDT, and aims to promote the development of intelligent diagnosis and treatment of diseases in China.
1.1 Definition of CDSS
Clinical Decision Support System (CDSS) is a system tool that leverages computer technology to provide healthcare professionals with alerts, reminders, patient data views, and clinical decision support during diagnosis and treatment. It is based on clinical knowledge (including clinical guidelines, evidence-based medicine, drug package inserts, pharmacopoeia standards, etc.) as well as patients’ basic information and clinical conditions [4]. Its purpose is to offer decision support for disease diagnosis, treatment, and rational drug use during the care process, thereby improving the quality of medical care.
1.2 Development History and Types of CDSS
Based on the emergence timeline, system architecture, and characteristics of knowledge representation, the development of Clinical Decision Support Systems (CDSS) can be broadly divided into four stages. Stage 1: Standalone CDSS, which emerged in the 1960s, with typical representatives including Ledley & Lusted, Leeds, and MYCIN. Stage 2: Integrated CDSS, which appeared in the late 1960s, represented by systems such as HELP and RMRS. Stage 3: Standardized CDSS, which originated in the 1990s, exemplified by Arden Syntax and GLIF. Stage 4: Service-oriented CDSS, which emerged in the early 21st century alongside the rapid development of internet technology, with examples including SAGE, SEBASTIAN, and SANDS.
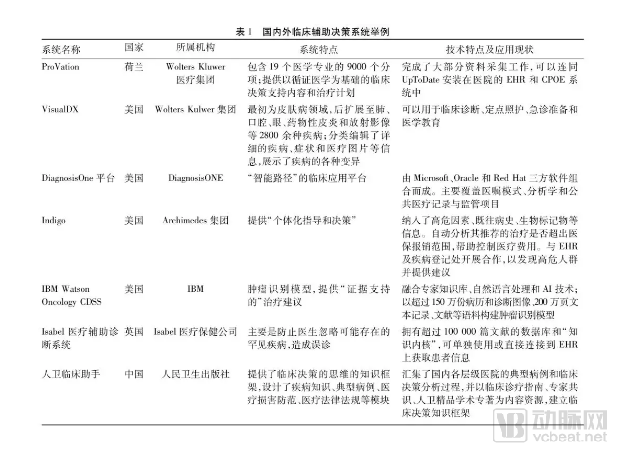
Based on design principles, Clinical Decision Support Systems (CDSS) are categorized into two types: knowledge-based CDSS and non-knowledge-based CDSS. Knowledge-based decision support systems constitute the majority of current CDSS implementations. Their core lies in the construction of a knowledge base and the specific application of this knowledge to support decision-making. This type of CDSS relies partially on rules and associations that include compiled information, typically employing IF-THEN rules for knowledge storage and management. Non-knowledge-based CDSS predominantly utilize artificial intelligence (AI) approaches, enabling computers to acquire knowledge from historical experiences or other clinical data. Common methods include artificial neural networks, Bayesian networks, and genetic algorithms [5]. Examples include Isabel Healthcare in the United Kingdom and VisualDX in the United States (Table 1).
From the perspective of the current research status of Clinical Decision Support Systems (CDSS), foreign countries started earlier and developed faster, with the majority having reached the second and third stages characterized by integrated and standardized systems, and gradually progressing toward the fourth stage. In contrast, China started later and developed more slowly, remaining largely in the first stage, although attempts have been made to research, develop, and apply systems at higher stages. Regarding the current application status, domestic CDSS applications are mainly concentrated on theoretical research, focusing on diagnosis for single diseases or single disciplines, as well as intelligent review and result interpretation within laboratory information systems during auxiliary examinations. CDSS systems with genuine personalized analysis and decision-support capabilities have not yet been realized.
1.3 Limitations of Current CDSS
The implementation and promotion of Clinical Decision Support Systems (CDSS) are critical measures to address challenges in the healthcare industry, such as data explosion, overwhelming demand, and resource scarcity. However, the current level of CDSS adoption remains suboptimal across all types. Knowledge base–driven CDSS often exhibit insufficient integration with clinical workflows, while AI-based CDSS remain far from mature.
Summary of the reasons:
(1) The scale of the knowledge base is insufficient, and its update speed is limited.
(2) Lack of support for standardized information models, due to inconsistent system standards, resulting in poor portability and difficulty in promotion and application.
(3) Whether it can rapidly and intelligently process massive volumes of heterogeneous, high-complexity clinical data.
(4) Lack of a shared service model: Currently, mainstream Clinical Decision Support Systems (CDSS) are embedded as subsystems within Electronic Medical Records (EMR), such as clinical pathway systems and rational drug use systems. It is critically important to determine whether these systems can accurately and sensitively capture user attention without disrupting their workflow.
(5) Lack of comprehensive decision support: The functionalities of most Clinical Decision Support Systems (CDSS) are limited to providing clinicians with reminders, alerts, and treatment recommendations for patient care, while lacking support for post-discharge outcome evaluation, health education, and other services.
(6) Patient information may be scattered across multiple disparate information systems, with no single system providing a complete view of the patient’s data.
(7) Traditional CDSSs merely provide passive guidance and lack clear pathways for consultations in cases of complex or rare diseases; single-discipline-based CDSSs are no longer able to meet clinical needs [6].
In view of the limitations of traditional CDSS mentioned above, and in combination with national policies and the practical needs of medical institutions, our team believes that CDSS should possess the following characteristics in the era of big data:
(1) A highly structured, computable authoritative knowledge base.
(2) By integrating knowledge bases, real-world data, and AI technologies, the system learns from and identifies patterns within massive clinical datasets to automatically acquire knowledge for decision support.
(3) It can be embedded into clinical systems, seamlessly integrating with electronic medical record (EMR) systems to intelligently extract patient disease characteristics and provide recommendations, thereby facilitating physician use and aligning with clinicians' daily workflows.
(4) Capable of evidence-based traceability, with recommended results linked to supporting evidence such as clinical guidelines, literature, and similar case records.
2.1 Definition and Design Objectives of MDT
Multidisciplinary Team (MDT) is a widely advocated diagnostic and therapeutic model in modern healthcare. It typically involves a relatively stable group of experts from multiple disciplines who convene regular, scheduled meetings at designated locations to provide clinical treatment recommendations for diseases affecting specific organs or systems. The aim is to offer patients the most scientific and rational treatment plan based on multidisciplinary deliberation, which is particularly suitable for the diagnosis and management of complex conditions such as cancer and heart failure. Furthermore, MDT can effectively promote disciplinary development and achieve concurrent improvements at the levels of individual physicians, departments, and hospitals [7].
2.2 Development History and Current Status of MDT at Home and Abroad
The MDT model, which originated in the United Kingdom, has been introduced into the medical field for over 70 years. In the early 1990s, the oncology MDT model was promoted nationwide across the UK. Since the 1990s, the oncology MDT model has developed rapidly in Europe and the United States. In 1997, The University of Texas MD Anderson Cancer Center took the lead in the U.S. by fully implementing subspecialty-specific clinical pathways for oncology, giving rise to the MDT in its true sense. In 2007, the United Kingdom enacted legal documents stipulating that “every cancer patient must receive comprehensive diagnosis and treatment through an MDT.” France subsequently issued similar legal documents. Currently, Europe has the most mature implementation of oncology MDT, with nearly 65% of hospitals conducting oncology MDT, whereas only 35% of hospitals in Asia have implemented oncology MDT, primarily concentrated in Japan [8].
Multidisciplinary Team (MDT) initiatives in China started relatively late. The concept of multidisciplinary collaboration was first proposed in the early 1980s, and large tertiary Grade A hospitals, such as West China Hospital of Sichuan University, subsequently established MDT models. In 2010, the Ministry of Health of China began to form the National Committee for Standardized Diagnosis and Treatment of Cancer. MDT has gradually gained recognition and popularity in some tertiary Grade A hospitals and specialized treatment centers across the country, with continuous issuance of guidelines for standardized cancer diagnosis and treatment.
In 2018, the National Health Commission issued the "Notice on Launching Pilot Programs for Multidisciplinary Diagnosis and Treatment of Cancer," deciding to carry out nationwide pilot programs for multidisciplinary diagnosis and treatment (MDT) of cancer from 2018 to 2020. Currently, many regions in China are exploring, developing, and implementing the cancer MDT model. For instance, the Cancer Hospital of the Chinese Academy of Medical Sciences has established MDT services for specific diseases, including lymphoma, urological cancers, head and neck cancers, thoracic cancers, gastrointestinal cancers, hepatobiliary and pancreatic cancers, and breast cancer [9]. Institutions such as Peking Union Medical College Hospital, Zhongshan Hospital Fudan University, and West China Hospital of Sichuan University have developed their own therapeutic specialties by leveraging regional medical resources and expert capabilities. The Jiangsu Province People’s Hospital has opened multidisciplinary joint outpatient clinics for gastric cancer, lung cancer, lymphoma, gynecological cancers, colorectal cancer, and stroke [10]. Some economically less-developed regions are also actively promoting cancer MDT; for example, the Inner Mongolia Autonomous Region Cancer Hospital and the Affiliated Tumor Hospital of Xinjiang Medical University have established multidisciplinary teams for seven types of cancer, including lung cancer.
Although many large hospitals have established “one-stop” multidisciplinary diagnosis and treatment centers organized by disease type, certain limitations remain.
2.3 Limitations of Standalone MDT Systems
Multidisciplinary Team (MDT) is regarded by many experts as the ideal model for diagnosis and treatment [11]. However, it has not yet been widely implemented in China. Some existing MDT practices are irregular and plagued by numerous issues, such as: becoming a mere formality; having few and non-permanent experts; inconsistent quality; failure to implement decisions made during MDT meetings; and a disconnect between initial diagnosis and subsequent follow-up after consultation discussions, which prevents continuous tracking of treatment plans and integrated analysis [12].
The underlying reasons include not only the lack of policy intervention and support at the national level, but also the insufficient supply of high-quality medical talent [8]. The “data silos” and “information barriers” formed among hospitals and across regions hinder the implementation of standardized management [13]. Furthermore, decision-making quality varies due to constraints such as unstructured case discussions and time pressure [14]. A substantial amount of information is required prior to consultations; in the absence of a foundational consultation database, MDT members are compelled to make optimal decisions within a limited timeframe [15]. Consequently, omissions of certain relevant data may lead to erroneous MDT decisions. Excessive workloads and time pressure are also the most significant factors contributing to lowered morale within MDT teams, reduced expert participation, and hasty decision-making [11]. How to effectively leverage big data resources and AI technologies to overcome these limitations remains a question worthy of consideration.
3.1 The Current Status of Hepatobiliary Tumors in China Urgently Requires a Transformation and Upgrade of Diagnosis and Treatment Models
Malignant tumors of the liver and biliary tract are characterized by low rates of early diagnosis, resectability, and efficacy of adjuvant therapy, resulting in persistently high mortality rates [16]. China is a country with a high incidence of hepatobiliary malignancies. Among these, primary liver cancer ranks as the fourth most common cancer and the second leading cause of cancer-related mortality in China [17-18]. The latest annual figures show 380,000 new cases and 326,000 deaths, accounting for approximately 51% of the global incidence, which poses a serious threat to public health.
Although a small minority of patients with early-stage disease are eligible for curative interventions such as surgical resection, liver transplantation, and local ablation, the vast majority of patients with intermediate to advanced-stage disease require multimodal treatment strategies. These include localized surgery, transarterial chemoembolization (TACE), minimally invasive ablation, radiotherapy, targeted therapy, immunotherapy, management of underlying liver disease, and treatment of complications. This approach necessitates the integration of multidisciplinary expertise and experience, rendering hepatobiliary malignancies among the most complex and refractory tumors [19]. Furthermore, the pronounced heterogeneity of hepatobiliary malignancies—encompassing population heterogeneity [20] and spatiotemporal heterogeneity [21]—leads to variable clinical treatment responses and a narrow therapeutic window.
For hepatobiliary malignancies, "precise classification" and "precise treatment" should be implemented with the theoretical and technical support of multidisciplinary team (MDT) diagnosis and treatment. In 2014, China issued the Expert Consensus on the Establishment of Liver Cancer MDT Teams and Multidisciplinary Combined Treatment. The 2018 Clinical Practice Guidelines for Hepatocellular Carcinoma published by the European Association for the Study of the Liver also emphasized for the first time that the clinical diagnosis and treatment of hepatocellular carcinoma should involve collaborative efforts among multiple disciplines, including hepatology, diagnostic radiology, pathology, surgical oncology, medical oncology, and radiation oncology [22].
However, in China, except for a small number of tertiary general hospitals at or above the provincial level that are capable of implementing multidisciplinary team (MDT) approaches to provide rational, comprehensive treatment decisions for patients at different disease stages, the vast majority of primary care hospitals have very limited understanding of the diagnosis and management of hepatobiliary tumors. These institutions lack the capacity to design appropriate comprehensive treatment plans, which severely compromises patients’ survival benefits.
3.2 The Era Trend of Building a CDSS+MDT Joint Platform Based on Big Data and AI Technology
In oncology diagnosis and treatment, the substantial increase in the variety and volume of data used for medical decision-making has become a major challenge. Key questions include how to enhance the quality of Multidisciplinary Team (MDT) discussions and achieve standardized decision-making processes based on the best medical evidence [23], and how to overcome these limitations by integrating Clinical Decision Support Systems (CDSS) to provide precise, evidence-based decision recommendations. These represent significant technical challenges for intelligent diagnosis and treatment, requiring the precise design and implementation of systematic computational frameworks, the realization of semantic interoperability, and a transformation in knowledge presentation methods. In 2009, Royal Free Hospital in London, UK, pioneered the integration of a CDSS platform into breast cancer MDTs, known as MATE (Multidisciplinary Assistant and Treatment sElector). It was reported that high-quality CDSS platforms could be effectively deployed in real-world clinical settings, significantly improving MDT operational efficiency, and it was suggested that this model could be extended to MDTs for other cancer types [23-24]. In 2014, Dr. Sesen from the University of Oxford, UK, first applied an intelligent CDSS platform to assist MDT proceedings, combining rule-based and probabilistic reasoning to help clinical MDTs achieve optimal decision-making in lung cancer treatment [15].
In 2016, China issued the “Guiding Opinions of the General Office of the State Council on Promoting and Standardizing the Application and Development of Health and Medical Big Data” (hereinafter referred to as the “Opinions”) [25], which proposed improving tiered diagnosis and treatment information systems based on internet and big data technologies to extend and enhance the service capabilities of healthcare institutions. In August 2018, the Bureau of Medical Administration and Hospital Management of the National Health Commission released the “Notice on Launching Pilot Programs for Multidisciplinary Team (MDT) Diagnosis and Treatment of Tumors,” requiring that from 2018 to 2020, a certain number of hospitals be selected nationwide to conduct pilot programs for MDT diagnosis and treatment of tumors. By implementing these MDT pilots, the leading and demonstrative roles of pilot hospitals would be leveraged to gradually promote this model across China, thereby improving the comprehensive level of disease diagnosis and treatment [7]. In active response to national policy initiatives and contemporary development trends, the Peking University Health Science Center and the U.S. National Cancer Institute jointly hosted the “2018 Beijing International Forum on Hepatobiliary Tumors” in November 2018, during which the “Launch Ceremony of the Multidimensional MDT Big Data Collaborative Technology Platform Project for Hepatobiliary Tumors” was held. This event marked the first proposal to “empower intelligent diagnosis and treatment of hepatobiliary tumors by integrating Clinical Decision Support Systems (CDSS) with MDT.” It is reasonable to believe that the deep integration of big data technologies, health and medical big data, and MDT systems will inevitably usher in a new generation of transformations in MDT, further enhancing the efficiency and quality of medical services.
3.3 China Has Initially Established the Data and Technical Foundations for Building a Joint CDSS+MDT Platform
With the advancement of hospital informatization, electronic medical record data have been continuously accumulated and developed. From the perspective of national policy, the aforementioned “Opinions” [25] propose that “China should standardize and promote the integration, sharing, open access, and application of health and medical big data; by 2020, achieve cross-departmental and cross-regional sharing with foundational data resources such as population, legal entity, and spatial geographic data, and attain significant results in the integrated application of data across healthcare, pharmaceuticals, medical insurance, and other related fields.”
From a grassroots development perspective, on February 20, 2017, the Chinese Society of Clinical Oncology (CSCO) launched the “China Primary Liver Cancer Clinical Registry Study” project. The first phase enrolled complete clinical data for patients treated in the hepatobiliary oncology departments of 20 large tertiary A hospitals nationwide. The second phase planned to include data from 55 hospitals. As of April 21, 2019, the CLCS project had initiated data collection at 43 research centers, completing initial diagnosis and treatment data collection for nearly 20,000 patients, as well as full-course diagnosis and treatment data for nearly 10,000 patients.
Some hospitals have implemented patient tracking and management through in-person interviews, telephone follow-ups, and online interactions via WeChat official accounts, thereby obtaining more comprehensive data from both in-hospital and out-of-hospital settings. This provides a solid data foundation for the integration of Clinical Decision Support Systems (CDSS) and Multidisciplinary Teams (MDT), facilitating the realization of the significant potential of intelligent MDT.
To address the imbalance in physicians’ comprehensive clinical management capabilities under China’s “tiered diagnosis and treatment” policy, Peking University Health Science Center and the Fifth Medical Center of PLA General Hospital (formerly the 302nd Hospital of the PLA), in collaboration with the Asia-Pacific Liver Disease Technology Alliance/Liver and Biliary Tumor Expert Committee, jointly established a national multidisciplinary team (MDT) big data collaboration platform for liver and biliary tumors. This platform, built on big data and artificial intelligence technologies, provides intelligent clinical decision support for liver and biliary tumors and officially entered trial use within parts of the alliance in November 2018.
In the future, integrating clinical data resources from hospital information systems with advanced big data technologies [26-27], combined with Clinical Decision Support Systems (CDSS) and Multidisciplinary Teams (MDT), may emerge as a new model for the intelligent diagnosis and treatment of hepatobiliary tumors [13]. This approach is expected to achieve the following: intelligently initiating MDT consultations for complex cases while leveraging CDSS, based on evidence association and mining techniques, to recommend the latest research findings, alternative treatment options, anticipated efficacy, and comparative analyses of advantages and disadvantages, thereby further reducing limitations and even errors in clinical decision-making [28-29]; CDSS can enhance adherence to MDT decisions and standardize treatment processes by tracking physicians’ therapeutic behaviors; CDSS can dynamically learn from MDT diagnostic and treatment opinions on complex medical records, continuously optimizing clinical decision logic to achieve iterative system updates [30]; by leveraging the advantages of distributed cloud storage and computer-assisted tools, a three-tiered medical collaboration model can be implemented, wherein provincial-level MDT teams guide regional-level MDT teams under the top-level design of national expert teams, ensuring the efficient operation of tiered diagnosis and treatment. It is believed that with the application and integration of health and medical data of Chinese residents in the future, a patient-centered data network can be established to provide various types of information required for clinical decision-making. This will create a diagnosis and treatment model for hepatobiliary tumors tailored to China’s national conditions, fundamentally improve patients’ healthcare experiences, and contribute to the building of a Healthy China.
Authors: Wang Xiaoyun1, Li Linfeng1,2, Guo Quan1, Zeng Yilan3, Li Haiyang4, Du Yingrong5, Chen Gang6, Liang Yuedong7, Lu Yinying8
Unit:
1. Yidu Cloud (Beijing) Technology Co., Ltd.;
2. School of Computer and Information Technology, Beijing Jiaotong University;
3. Department of Hepatology, Chengdu Public Health Clinical Medical Center;
4. Hospital Administration Office of the Affiliated Hospital of Guizhou Medical University;
5. Hospital Administration Office, Kunming Third People's Hospital, Yunnan Province;
6. Hospital Office of Taiyuan Third People's Hospital;
7. Hospital Administration Office, Guiyang Public Health Treatment Center;
8. Center for Diagnosis, Treatment and Research of Liver Tumors, the Fifth Medical Center of Chinese PLA General Hospital
Lu Yinying
Director, Center for Diagnosis, Treatment and Research of Liver Tumors, The Fifth Medical Center of Chinese PLA General Hospital
M.D., Distinguished Professor at Peking University Health Science Center, Distinguished Researcher at the Center for Synthetic and Systems Biology, Tsinghua University, Master’s Supervisor, and Director of the Liver Tumor Diagnosis, Treatment, and Research Center at the Fifth Medical Center of the PLA General Hospital.
Current Chairperson of the Asia-Pacific Alliance for Liver Disease Technology / Professional Committee on Liver Tumors; Vice Chairperson of the Chinese Association of Research Hospitals / Professional Committee on Molecular Diagnostics; Vice Chairperson of the Beijing Health Promotion Association / Branch on Hepatobiliary and Pancreatic Tumors; Secretary-General of the Young Committee of the Western Returned Scholars Association Physicians Society; Member of the CSCO Professional Committee on Tumor Immunology / Professional Committee on Liver Cancer; Standing Committee Member of the China Association for Precision Diagnosis and Treatment of Cancer.
This article was authored by Wang Xiaoyun from Yidu Cloud (Beijing) Technology Co., Ltd. as the first author, under the meticulous guidance of Professor Lu Yinying from the Fifth Medical Center of the Chinese PLA General Hospital. Professor Lu’s rigorous work ethic and profound academic expertise served as a strong foundation for the successful completion of this article. As a medical artificial intelligence company, Yidu Cloud provided technical support in building an AI collaboration platform, thereby accelerating and enhancing the efficiency of intelligent disease diagnosis and treatment.
Going forward, Yidu Cloud will continue to fuel the innovative development of “Internet + Healthcare,” leveraging advanced technologies to enhance healthcare quality, empower physicians to improve their diagnostic and therapeutic capabilities, facilitate medical research with greater ease, and strive to become the “cloud that safeguards public health.”