Multi-Ministry Joint Issuance of the Pilot Work Plan for Regional Medical Center Construction with 8 Pilot Provinces and 30 Output Hospitals
VCBeat (WeChat: vcbeat) has learned that, to further implement the Healthy China strategy, advance supply-side structural reform in the health sector, effectively address the public’s difficulties in accessing medical care, and promote the development of regional medical centers, the National Development and Reform Commission, the National Health Commission, the National Administration of Traditional Chinese Medicine, and the Secretariat of the State Council’s Leading Group for Healthcare Reform jointly issued the “Work Plan for Pilot Programs on the Construction of Regional Medical Centers” recently.
The plan primarily includes the following key points:
Expected Goals:Through three to five years of effort, the gap in the treatment level of key diseases between relevant regions and those in Beijing, Shanghai, and other areas has been significantly narrowed; cross-provincial and cross-regional medical consultations have decreased substantially, driving breakthrough progress in the establishment of a tiered diagnosis and treatment system.
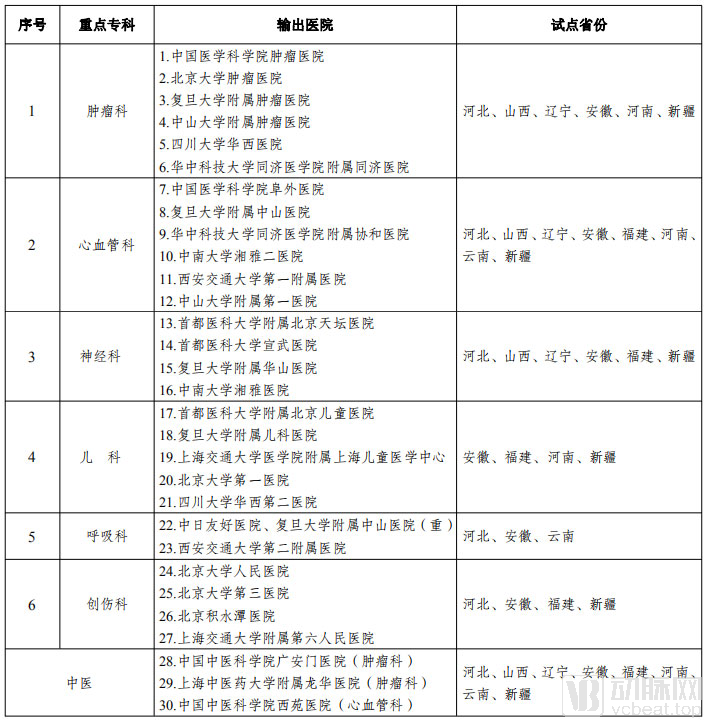
Key Disease Categories:Prioritize the development of six specialties: Oncology, Neurology, Cardiology, Pediatrics, Respiratory Medicine, and Trauma Surgery.
Pilot Regions:Pilot construction was launched in eight provinces and autonomous regions: Hebei, Shanxi, Liaoning, Anhui, Fujian, Henan, Yunnan, and Xinjiang.
Discharging Hospital:The 30 pilot exporting hospitals were primarily selected from Beijing and Shanghai, with a small number chosen from five other cities with concentrated high-quality medical resources: Wuhan, Changsha, Guangzhou, Chengdu, and Xi’an.
Construction Model:Including the public hospital model primarily funded by government investment and the private healthcare model based mainly on purchasing services.
Full Text of the Work Plan for the Pilot Program on the Construction of Regional Medical Centers
In accordance with the work arrangements of the Central Committee of the Communist Party of China and the State Council, this work plan is hereby formulated to deeply implement the Healthy China Strategy, advance supply-side structural reform in the health sector, make concerted efforts to address the difficulties people face in accessing medical care, and promote pilot initiatives for the development of regional medical centers.
I. General Requirements
(I) Overall Approach. Guided by Xi Jinping Thought on Socialism with Chinese Characteristics for a New Era, we will fully implement the spirit of the 19th National Congress of the Communist Party of China and its Second and Third Plenary Sessions. Adhering to a people-centered approach to health, and relying primarily on National Medical Centers while giving full play to the role of National Clinical Research Centers for Medicine, we will select a number of high-quality medical institutions in regions with abundant medical resources, such as Beijing and Shanghai. By establishing branch centers and affiliates, promoting multi-site practice for physicians, and employing other measures, we will build Regional Medical Centers in areas with significant patient outflows and relatively scarce medical resources. We will make full use of advanced technologies such as “Internet Plus Healthcare,” artificial intelligence, and big data to promote the grouped and brand-oriented development of high-quality medical resources, thereby better meeting the public’s demand for medical services.
(II) Expected Goals. Through three to five years of effort, a number of high-level clinical diagnosis and treatment centers, advanced talent training bases, and high-standard platforms for scientific research innovation and translation will be established in regions with shortages of high-quality medical resources. A cohort of medical groups with distinct brand advantages and capable of providing high-level services across regions will be cultivated. A series of “Internet + Healthcare” collaborative platforms supported by high-level hospitals will be developed, and a number of specialty alliances centered on regional medical centers will be formed. The gap in the treatment of key diseases between these regions and leading areas such as Beijing and Shanghai will be significantly narrowed, cross-provincial and cross-regional medical visits will be substantially reduced, and breakthrough progress will be made in the construction of the tiered diagnosis and treatment system.
(3) Basic Principles.
First, we must adhere to a problem- and goal-oriented approach. Focusing on key diseases and underserved regions, we will strengthen comprehensive planning, take targeted measures to address shortcomings, reinforce weak areas, and improve quality, thereby accelerating the development of regional “highlands” of medical services and minimizing cross-regional medical visits to the greatest extent possible.
Second, prioritize the integration of existing resources. Pilot regions are encouraged to foster collaboration between established medical institutions with a solid foundation and introduced high-level hospitals, making full use of existing facilities, equipment, and personnel to strategically amplify the impact of national top-tier premium medical resources.
Third, ensure the fulfillment of public welfare responsibilities. Regional medical centers must fully assume their public welfare obligations in providing basic medical services. Pilot regions must uphold the public welfare nature of healthcare, fulfill governmental responsibilities in operating medical institutions, and encourage social forces to establish non-profit medical institutions.
Fourth, we will coordinate and advance the integrated reform of medical care, health insurance, and pharmaceuticals. We will grant regional medical centers more flexible policies in areas such as pricing, medication use, and talent management, thereby exploring pathways and accumulating experience for establishing a modern hospital management system that incentivizes staff and ensures sustainability.
Fifth, resolutely and effectively prevent risks. Scientifically plan project layouts to avoid blind and disorderly expansion, striving to achieve the “three no’s”: no capital contribution from hospitals, no new government debt risks, and no increased burden on patients. During the pilot period, each pilot province or region should, in principle, prioritize the establishment of no more than three regional medical centers.
II. Work Arrangements
The reform to establish regional medical centers has a broad impact and has drawn significant public attention. In line with the working principle of “selecting hospitals based on key disease categories, choosing regions according to needs, fostering hospital–local government collaboration, and promoting joint development by provincial and national authorities,” pilot projects were launched first, with experiences continuously summarized and refined during the pilot phase.
(1) Key Disease Categories. Priority will be given to diseases characterized by high mortality rates, substantial disease burden, concentrated patterns of patient referrals outside the local area, and severe threats to public health. Six specialties—oncology, neurology, cardiology, pediatrics, pulmonology, and traumatology—will be prioritized for development.
(II) Pilot Regions. Taking into comprehensive consideration factors such as the shortage of high-quality medical resources within the region, the absence of hospitals directly administered by the central government or domestic first-class hospitals reaching the “national team” level, a large population base, a high volume of patients seeking medical care outside their home regions, advantageous geographical location, convenient transportation, and alignment with national strategic development needs, pilot programs will be launched in eight provinces and autonomous regions: Hebei, Shanxi, Liaoning, Anhui, Fujian, Henan, Yunnan, and Xinjiang.
(3) Output Hospitals. Output hospitals included in the pilot program for regional medical centers should, in principle, possess leading medical technical expertise and a high level of domestic recognition; maintain ample talent reserves so that their technical capabilities are not diluted by the establishment of regional medical centers; and demonstrate outstanding clinical teaching capabilities and robust research capacity, enabling them to train technical backbones and disciplinary leaders for the region and undertake national-level research projects. The 30 pilot output hospitals are primarily selected from Beijing and Shanghai, with a small number chosen from five other cities with concentrated high-quality medical resources: Wuhan, Changsha, Guangzhou, Chengdu, and Xi’an. Except for some municipal hospitals in Beijing and Shanghai, all others are hospitals administered by the National Health Commission, the National Administration of Traditional Chinese Medicine, and universities directly under the Ministry of Education. Meanwhile, several high-level private medical institutions will be actively reserved as candidates for subsequent pilots to ensure their fair participation.
(IV) Construction Model. Adhering to the primary principle of safeguarding the public-welfare nature of basic medical and health services, construction shall rely mainly on existing local medical resources. Local authorities may select appropriate construction and operational models based on the nature and characteristics of the partner hospitals, so as to effectively enhance sustainable development capacity and strive to ensure public welfare, mitigate risks, maintain high quality, and enable development.
1. The public hospital model primarily funded by government investment, in which the exporting hospital and the government of the pilot region jointly establish independent medical institutions to fulfill the responsibilities of regional medical centers. Construction funds are mainly raised locally, with central budgetary investments allocated as appropriate. All first-batch pilots adopted this model.
2. A social-run medical care model primarily based on service procurement, wherein socially operated hospitals with corresponding technical capabilities, extensive experience in hospital management, and a good professional track record directly establish branch institutions in pilot regions to achieve group-based and branded development; central budgetary investments shall provide appropriate subsidies for the construction of non-profit medical institutions established under this model.
III. Reform Measures
Include regional medical centers in the national pilot program for establishing and improving the modern hospital management system, strengthen policy support, strive to achieve breakthroughs and innovations in key areas, and fully leverage their demonstrative and leading role.
(1) Advancing the reform of the management system. Regional medical centers shall implement a director responsibility system under the leadership of the Party Committee, and establish and improve the decision-making mechanisms of the Hospital Party Committee and the Director’s Office Meeting. Explore the establishment of a council for medical groups to clarify the relationships among output hospitals, healthcare sponsors, pilot regions, and social forces. Formulate hospital charters, improve management systems, strengthen performance evaluations, and promote the transformation of regional medical centers from scale-expansion-oriented to quality-and-efficiency-oriented development models to enhance institutional development quality; shift from extensive management to refined management in operational models to improve service levels and efficiency; and redirect investments from focusing on facility construction to emphasizing connotative development, thereby promoting modernization of standards, integration of services, informatization of management, and group-based operational models.
(II) Deepen the reform of the personnel and compensation systems. Permit regional medical centers to explore management measures and distribution policies that align with their operational models. Establish a dynamic adjustment mechanism for staff quotas, rationally determine the number of positions, and explore delegating the authority to evaluate senior professional titles to regional medical centers. Support regional medical centers in independently recruiting staff and determining personnel structures in accordance with national regulations and their own development needs, thereby implementing autonomy in employment and enabling flexible personnel mobility and promotion/demotion mechanisms. Implement the “Two Permissibles” policy and rationally determine the compensation levels of regional medical centers. Fully grant regional medical centers autonomy in income distribution, determining the compensation levels of medical personnel based on factors such as years of education, working hours, knowledge and skill levels, and the difficulty and complexity of tasks. Gradually establish a compensation structure that primarily reflects position value, reduce the proportion of performance-based pay, stabilize expectations among medical personnel, emphasize long-term incentives, and, where conditions permit, implement various compensation models such as position-based salary, target annual salary, and negotiated compensation systems. Research and explore treating the Standardized Residency Training Certificate as equivalent to a master’s professional degree certificate, ensuring equal treatment in recruitment, promotion, position appointment, and salary benefits. Establish multi-channel funding guarantees and compensation incentive mechanisms, allowing qualified medical personnel in regional medical centers to earn reasonable additional income through multi-site practice and opening clinics, provided they have fulfilled their primary job responsibilities.
(3) Improve the hospital compensation mechanism. Explore a compensation mechanism that aligns with the functional positioning of regional medical centers, incentivizes cost reduction and efficiency improvement, and promotes the equalization of medical resources across regions. Fully implement government investment policies for regional medical centers, increase investment in the development of key disciplines and talent cultivation, and establish a funding guarantee mechanism for contributions to the pension insurance reform for public institutions. Reasonably formulate and dynamically adjust medical service prices in accordance with the requirements of “overall cost control, structural adjustment, and balanced increases and decreases.” Implement health insurance policies adapted to the development patterns of regional medical centers. Actively advance reforms in health insurance payment methods, prioritizing the implementation of case-based payment and Diagnosis-Related Groups (DRG)-based payment reforms in regional medical centers. Establish a negotiation and consultation mechanism between regional medical centers and health insurance agencies to reasonably determine and dynamically adjust the total budget indicators for health insurance funds and payment standards such as case-based payments.
(4) Encourage the use of innovative drugs and technologies. Grant regional medical centers necessary policies for the application of new technologies, encourage clinical trials of innovative drugs and medical devices, and gradually expand the use of medical devices currently undergoing clinical trials for the treatment of life-threatening conditions that have not yet been approved for registration in China within regional medical centers. Encourage regional medical centers to leverage the advantages of their key departments to submit applications for temporary importation, in accordance with the law, for a small number of clinically urgent drugs that are genuinely needed within the region but not yet registered domestically; the National Medical Products Administration shall expedite the approval process. Output hospitals and regional medical centers shall conduct or participate in the procurement of high-value medical consumables in accordance with national and local requirements to reduce artificially inflated prices.
(5) Enhancing sustainable development capabilities. Support regional medical centers in carrying out technological innovation and the transformation of scientific and technological achievements; the resulting revenues shall be primarily used for personnel incentives, included in the total compensation pool of the institution for the current year, but exempt from overall caps and excluded from the base calculation of the total compensation pool. Encourage the establishment of a certain number of medical schools and research institutions, relying on “Double First-Class” universities with regional medical centers as the core, to promote the integrated development of medicine, education, research, and industry, and to cultivate backbone medical technical talent within the region. Support regional medical centers in providing “Internet + Healthcare” services, formulate pricing and medical insurance policies for telemedicine services, establish telemedicine and education platforms, and provide services such as remote diagnosis and treatment, medical education, clinical pathway guidance, and remote surgical demonstrations to grassroots, remote, and underdeveloped areas, thereby improving the accessibility and overall efficiency of high-quality medical resources. Encourage social forces to participate in the construction of regional medical centers through undertaking non-clinical operations of public hospitals and other means. Encourage the introduction of commercial health insurance, develop commercial insurance products targeting special-needs medical care, innovative therapies, and advanced diagnostic and testing services, and strengthen information sharing among medical institutions, basic medical insurance agencies, and commercial health insurance organizations.
(6) Increase support for hospitals providing medical resources. Support these hospitals in strengthening their capacity to cultivate high-level medical professionals and discipline leaders, and appropriately increase the quotas for Beijing and Shanghai household registration (hukou) for relevant hospitals based on the volume of medical resources they provide. Governments in recipient regions shall provide support to medical personnel dispatched by these hospitals in areas such as household registration, housing, spousal relocation, children’s enrollment in schools, and rewards and subsidies. Where conditions permit, local governments shall allocate funds to provide reasonable compensation, ensuring that the remuneration of dispatched medical personnel reaches the average level of their counterparts with similar qualifications at the sending hospitals, and provide appropriate additional allowances on this basis.
IV. Organization and Implementation
(1) Establish a Special Coordination Group. Led by the General Office of the State Council, the National Development and Reform Commission, the National Health Commission, and the Secretariat of the Leading Group for Deepening Medical and Healthcare System Reform of the State Council, with participation from the Ministry of Education, the Ministry of Finance, the Ministry of Human Resources and Social Security, the National Healthcare Security Administration, the National Administration of Traditional Chinese Medicine, the National Medical Products Administration, the municipal governments of Beijing and Shanghai, and the provincial-level governments of pilot regions, the Group shall primarily study and propose pilot policies involving central government authority, coordinate support from the entities responsible for operating the output hospitals, guide pilot regions in introducing attractive preferential policies, and comprehensively coordinate the resolution of key and challenging issues arising during the pilot implementation.
(II) Mobilize all parties to participate actively. Adhering to the working principle of “hospital-led operations, local government-led construction, central government support, and social participation,” exporting hospitals and pilot regions shall engage in bilateral selection and voluntary cooperation, avoiding administrative mandates that force incompatible partnerships. The exporting hospitals shall assume primary responsibility for the operation and management of the Regional Medical Centers, tasked with transferring talent, technology, brand reputation, and management expertise to the pilot regions, thereby raising the overall level of medical services within the region in a relatively short period. The provincial governments of the pilot regions shall bear overall responsibility for the construction of the Regional Medical Centers, ensuring the provision of land, planning, and other construction conditions, waiving relevant fees, guaranteeing sufficient construction funding without gaps, and preventing any increase in new debt risks. Relevant central government departments shall include related projects in the key support scope of the central budgetary investment, making appropriate arrangements for the construction of clinical facilities, procurement of medical equipment, and development of informatization and scientific research platforms, while coordinating pilot policies requiring national-level approval. The central and local governments shall jointly foster a fair competitive environment and introduce social forces to participate in an orderly manner in non-clinical services such as logistics management at the Regional Medical Centers.
(3) Strengthen supervision and assessment. Incorporate reform measures such as tiered diagnosis and treatment, the development of medical consortia, the radiating influence of healthcare services, and “Internet + Healthcare” into the scope of supervision and assessment. Formulate regulatory methods and assessment indicators based on the functional positioning and responsibilities of regional medical centers, with a focus on key metrics such as the proportion of patient referrals outside the region for priority diseases, the proportion of complex and difficult cases diagnosed and treated, and the overall improvement in medical technical standards. This is to prevent blind expansion under the guise of reform, as well as the siphoning of patients and talent from primary care institutions.
V. Next Steps
The Special Coordination Group for the Development of Regional Medical Centers will strengthen follow-up guidance, engage in comprehensive planning, and promote steady progress. It will organize matchmaking and negotiations between the relevant exporting hospitals and pilot regions, carry out pilot development in batches in a prudent manner in accordance with this Plan, conduct full-process tracking and evaluation of the construction models and pilot policies for regional medical centers, and, based on the summarization of experience and refinement of policies, expand the scope of pilot development at an appropriate time.
Appendix: List of Pilot Output Hospitals and Provinces for Regional Medical Centers
Source: Official Website of the National Development and Reform Commission