Six Months After New Clinic Regulations, Are Doctors Still Eager to Open Clinics?
In May this year, the National Health Commission and four other ministries jointly issued the "Guiding Opinions on Launching Pilot Programs to Promote the Development of Clinics" (hereinafter referred to as the "Opinions"), initiating pilots in ten cities designated for clinic reform: Beijing, Shanghai, Shenyang, Nanjing, Hangzhou, Wuhan, Guangzhou, Shenzhen, Chengdu, and Xi’an. The "Opinions" streamline the procedures for establishing clinics and introduce multiple measures to encourage their establishment. Furthermore, they encourage physicians who have practiced in medical institutions for at least five years and hold intermediate or senior professional titles to establish specialized clinics on either a full-time or part-time basis.
On November 8, the National Health Commission also released the “Basic Standards for Clinics in Pilot Regions for Clinic Reform (2019 Revised Edition),” the first new set of standards since 2010, targeting the ten pilot cities announced in May this year. The document introduces adjustments and updates regarding professional title requirements for medical personnel, the removal of minimum floor area requirements, and the addition of provisions for health information system development.
In fact, in recent years, the state has successively introduced policies to gradually simplify the access process for social medical institutions, implementing the "integration of two certificates" for the approval of establishment and practice registration of medical institutions below the secondary level; in terms of physicians' free practice, it has long been liberalized and continuously encouraged. The new clinic regulations this year are a further clarification and refinement based on the previous foundation.
Now that half a year has passed since the release of the “Opinions,” how has implementation progressed in the pilot regions? Will simplifying market-entry procedures lead to a sudden surge in clinics overnight? Will encouraging physicians to open their own clinics spark an entrepreneurial wave among doctors? VCBeat (WeChat ID: vcbeat) interviewed multiple healthcare institution managers and, combining these insights with data, presents the following findings.
Pilot Areas Gradually Implement New Clinic Regulations
According to data released by the National Health Commission, there are currently nearly 220,000 registered and operational clinics across China, with an average of more than 7,000 clinics per province. The average number of practicing staff per clinic is 2.6, including an average of 1.4 physicians and 1.2 nurses. Diagnosis and treatment services for common and frequently occurring diseases in internal medicine, stomatology, traditional Chinese medicine (TCM) internal medicine, TCM surgery, orthopedics, and gynecology account for over 90% of clinic operations, playing a significant role in primary healthcare services. However, the development of clinics faces major challenges, including shortages of human resources, limited medical service capabilities, and difficulties in industry regulation.
Against this broad backdrop, the “Opinions on Launching Pilot Programs to Promote the Development of Clinics” were issued in May this year. The Opinions put forward multiple measures to facilitate clinic establishment and strengthen regulatory oversight, primarily focusing on simplifying clinic licensing procedures, adjusting basic standards for clinics, encouraging qualified physicians to establish clinics, and requiring clinics to implement information systems. Ten cities, including Beijing, Shanghai, and Shenyang, were designated as pilot sites.
Subsequently, multiple pilot regions followed suit, introducing corresponding implementation plans tailored to local conditions.
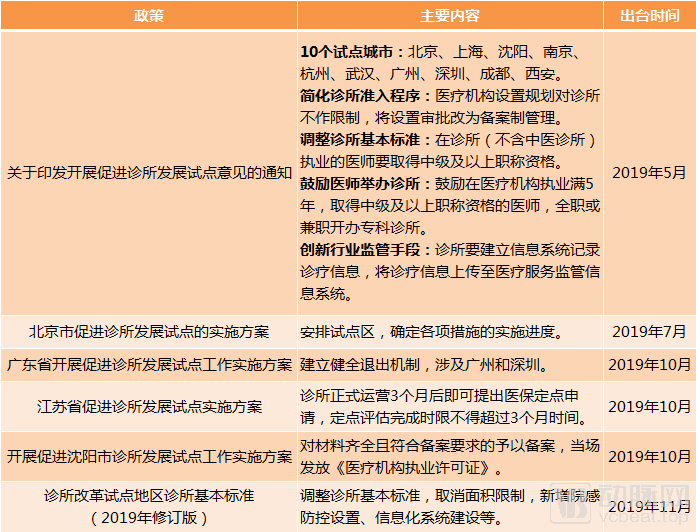
Policies Promoting the Development of Clinic Pilot Programs, Chart by VCBeat
In its May Notice, the National Health Commission proposed adjustments to clinic standards. In early November, the newly released Basic Standards for Clinics in Pilot Regions for Clinic Reform (2019 Revised Edition) was finally issued. Compared with the 2010 version, the main changes are as follows:
1. The new standards require clinical physicians to obtain a Physician Qualification Certificate, be registered, and have practiced in medical institutions for at least five years, holding the professional title of Attending Physician or higher. The previous requirement was simply holding a Physician Qualification Certificate.
2. For clinical laboratory testing, medical imaging, electrocardiography (ECG), pathology, and sterile supply services, if relevant service agreements are signed with other medical institutions to provide these services, the corresponding equipment need not be equipped. Compared with the 2010 version, ECG, pathology, and medical imaging have been added.
3. The usable area and architectural layout of the clinic need only meet the medical requirements of its approved diagnostic and treatment specialties. In contrast, the 2010 version required a minimum floor area of 40 square meters.
4. Add a new requirement to “establish an information system and, in accordance with the regulations and standards set by the health administrative authorities, achieve interconnectivity with the medical service supervision information system.”
As can be seen, the Standard continues to uphold the principles outlined in the Opinions. Compared with the previous version, the most significant change is the shift from a primary focus on auditing hardware, such as equipment and facilities, to evaluating the qualifications and competencies of physicians. This adjustment raises the qualification requirements for clinical physicians in clinics, thereby increasing the entry threshold for clinic practice, and introduces additional requirements for information technology systems.
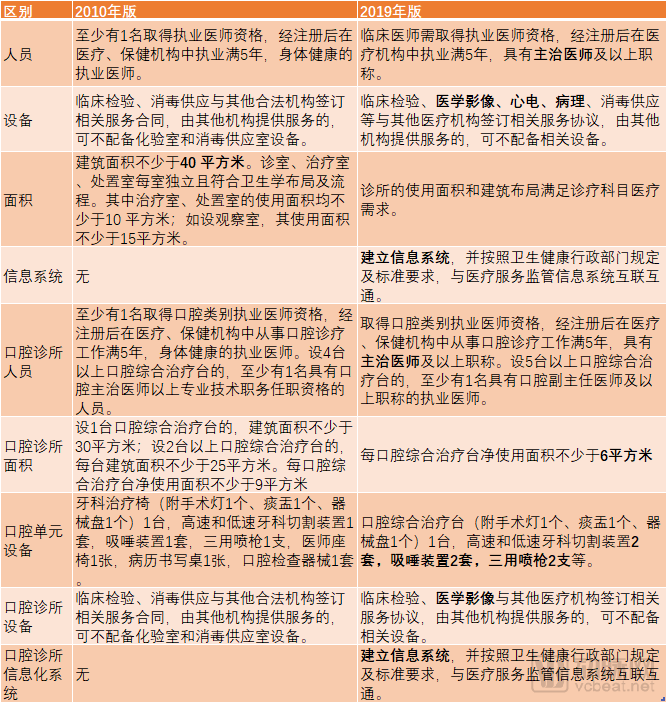
Specific Differences Between the Two Versions of the Standards, Chart by VCBeat
Simplified Procedures, Reduced Costs for Opening Clinics
Establishing a clinic has long been a headache for many entrepreneurs due to its time-consuming nature and complex procedures. Yu Ying, CEO of Youlin Clinic, once voiced strong complaints on Weibo about the difficulties in obtaining clinic approvals. With the implementation of the new regulations mentioned above, have clinic founders already experienced changes? We interviewed multiple healthcare institution managers in Shanghai, Chengdu, and other cities, and reviewed the changes in the clinic application process in light of previous policies, as illustrated below:
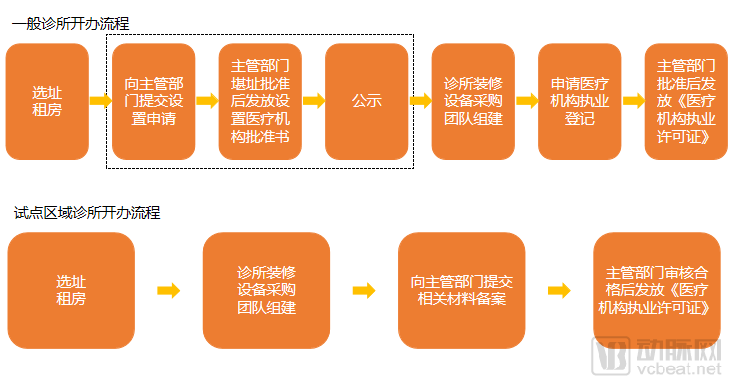
Comparison Chart of Establishment Procedures, Graphic by VCBeat
According to the Regulations on the Administration of Medical Institutions, the general process for establishing a clinic involves seven steps with the health administrative authorities. Numerous uncertainties exist within these steps. For instance, the site cannot be located adjacent to restaurants or schools, nor can it share access routes with other commercial or residential entities; failure to meet these requirements will result in failing the site assessment, thereby precluding the issuance of the Approval Letter for Setting Up a Medical Institution and preventing progression to subsequent steps. Even if the site assessment is passed, the public notification phase poses another challenge, as objections from the public can disrupt the subsequent procedures. These factors contribute to a prolonged approval process with significant risks, where an issue at any stage may ultimately prevent the clinic from opening.
According to the “Opinions” issued this year, opening a clinic requires only four steps, eliminating certain procedures in the standard process such as application for establishment and public notice (i.e., the steps within the dashed box in the figure above). Meanwhile, the approval system for establishment has been replaced with a filing-based management system. Applicants shall comply with the clinic standards of pilot regions, submit materials for filing, and upon successful review by the local county- or district-level health administrative department, be issued the “Medical Institution Practice License.”
“We established our Sijun Surgical Clinic in Shanghai in strict compliance with the new regulations and have already obtained the medical practice license,” introduced Dr. Bao Yuke, Vice President of Zhang Qiang Doctor Group. The entire process, from site selection and preparation to obtaining the practice license, took only six months, with the filing and licensing stage completed in just 20 working days. “Under normal circumstances, our construction timeline would require only three to four months. However, the construction progress of the Shanghai Sijun Surgical Clinic was somewhat affected due to coordination with park management requirements; otherwise, the entire process from site selection to licensure would have been even faster. Based on previous experience, this entire process could take up to a year.”
The “Opinions” also stipulate that chain and group clinics operating across administrative regions shall be uniformly filed with the higher-level health administrative department, while those operating across provincial-level administrative regions shall be separately filed with the health administrative departments of the respective provinces. Bao Yuke stated that, as cross-provincial operations also involve relationships between parent and subsidiary companies or between headquarters and branch companies under industrial and commercial registration, specific procedures for establishment will need to be explored in the future.
The “Opinions” have undoubtedly brought greater convenience to the establishment of clinics, not only by streamlining procedures and improving efficiency but also by directly reducing costs. Since there are no restrictions on clinics in healthcare institution planning, the scope for site selection is broader, allowing for locations with better cost-effectiveness. Bao Yuke cited an example: “Under previous requirements, medical institutions were required to have independent access routes, which in most cases limited clinic locations to the ground floor, where rents are high. Now, we can choose spaces on the second floor or above, resulting in direct savings on rent.”
Meanwhile, the new clinic standards no longer impose mandatory requirements on clinic floor area. Small clinics established by individuals may select locations and design layouts according to their needs, thereby reducing costs.
Driven by the new regulations, Dr. Zhang Qiang’s Doctor Group has not only rapidly established its Shanghai clinic this year but also initiated preparations for multiple clinics across China. “One of them has already secured a location, while several others are in the process of site selection,” revealed Bao Yuke.
No Short-Term Outbreak Occurred
The new regulations appear to lower the threshold for establishing clinics and encourage physicians who have practiced in medical institutions for at least five years and hold intermediate or senior professional titles to open specialty clinics on a full-time or part-time basis. This seems to herald another wave of clinic construction.
However, our review of clinic registration data in pilot cities from the implementation of the new regulations in May this year through the present reveals no significant change in overall numbers compared to the same period last year. This is likely attributable to physicians’ limited motivation to open clinics, coupled with more stringent access requirements and regulatory oversight. The simplification of approval procedures does not necessarily make it easier to establish a clinic; physicians must still carefully consider market conditions, the practice environment, and their own capabilities.
Doctors Are Not Flocking to Open Clinics
First, there is insufficient incentive for physicians to open clinics on a full-time basis. Regarding this point, Bao Yuke believes that for physicians still within the public healthcare system, leading specialists already possess significant renown, attract a large patient volume, and benefit from robust research platforms and favorable compensation packages; thus, they may not necessarily need to establish their own clinics. In contrast, ordinary physicians lack strong personal brands. Once they leave the public system—particularly major tertiary Grade A hospitals—their appeal to patients diminishes, making full-time private practice a risky endeavor.
Second, the environment for physicians to operate clinics on a part-time basis is not yet mature. Although the state has introduced a series of policies in recent years and adopted an increasingly open attitude toward physicians’ independent practice, physicians are still regarded as “employees of their institutions” in reality. Hospital administrators inevitably expect physicians to serve their hospitals on a full-time basis. If physicians operate clinics on a part-time basis, it is difficult to determine in the short term whether they are leveraging their primary practice institutions to “channel patients” to their own clinics, and how liability should be assigned in the event of medical malpractice or disputes. These ambiguities make it challenging for both hospitals and physicians to manage their mutual relationship when physicians engage in part-time clinic operations.
Third, a good doctor is not necessarily a good manager. Opening a clinic requires substantial energy and financial investment. Tasks such as site selection and positioning, brand building, managing doctor-patient relationships, handling public relations, and resolving medical disputes test not only a physician’s clinical expertise but also their business management and crisis response capabilities. However, specialization matters; most physicians within the public healthcare system possess strong clinical skills but lack the necessary business acumen to effectively manage a clinic. Furthermore, doctors are already burdened with heavy clinical and research workloads, leaving them with little time or energy to take on the additional responsibility of running a clinic.
Therefore, doctors have also rationally recognized these issues, making it unlikely that a large number of physicians will rush to open their own clinics.
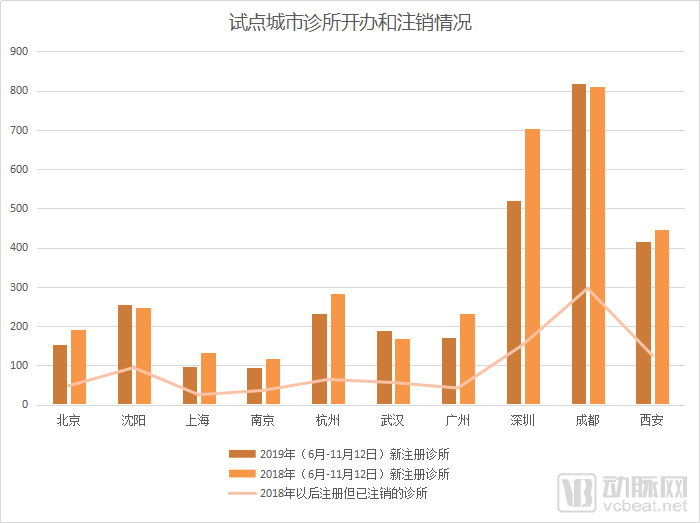
Registration and Deregistration of Clinics in Pilot Cities. Data source: Qichacha; Chart by VCBeat
The clinic also faces numerous challenges.
We also found that while a large number of clinics were newly registered, a significant number were simultaneously being deregistered. This trend is, of course, related to the operational performance of the clinics themselves; however, it is also important to recognize that the new regulations have imposed higher entry requirements and stricter regulatory measures, presenting multifaceted challenges for both the establishment and operation of clinics.
First, risks in the application process still exist. Since the step of applying for the establishment of a medical institution has been eliminated, it means that by the time a clinic completes its final filing, significant funds have already been invested in preliminary renovation and the development of both software and hardware infrastructure. If there are issues with the construction process itself, resulting in non-compliance with basic standards and failure to pass the filing review, any subsequent rectification or abandonment will lead to substantial losses of the initial investment. This places higher demands on the preparatory work for clinics.
Furthermore, the requirements for physician practice are more stringent. The new clinic standards mandate that clinicians must hold a Physician Practicing Certificate, have been registered and practiced in medical institutions for at least five years, and possess a professional title of Attending Physician or higher. This requirement itself serves as a threshold. In Bao Yuke’s view, this is highly reasonable and constitutes a test of physicians’ ability to practice independently. “Resident physicians who have just completed their standardized residency training lack sufficient clinical experience and are hardly capable of independently managing patient care.”
Wang Jun, founder of the Chuanpai Doctor Group, also stated that the new regulations would impose strict controls on issues such as the misuse of antibiotics and hormones in clinics, as well as non-compliant medical record-keeping. “Furthermore, to continuously improve the quality of care, physicians must strengthen their participation in continuing medical education.”
Finally, regulatory measures have become more stringent. The new regulations require the establishment of information systems that are interconnected with the medical service supervision information system, in accordance with the provisions and standards set by health administrative departments. It is understood that many traditional individual clinics currently do not use information systems, whereas most new-type clinics have largely completed their informatization construction through self-developed systems or third-party tools. Given the dispersed distribution of clinics and the uneven level of informatization, effective supervision is difficult to achieve through traditional methods.
Bao Yuke stated that although it is not yet clear how to interface with the regulatory system of the National Health Commission or which specific data should be integrated, it is evident that regulatory authorities aim to leverage big data, artificial intelligence, and other technologies to monitor clinical practices and medication use in clinics. This approach is intended to facilitate the timely identification of issues and enforce corrective actions, thereby ensuring the healthy operation of the industry amidst rapid development, while safeguarding medical quality and safety.
The “Opinions” explore models and policies for the development of clinics in pilot cities by optimizing practice licensing, improving service quality, and strengthening industry supervision, marking a substantive advancement in the role of clinics in undertaking more primary care diagnosis and treatment tasks. However, addressing the assumption of primary healthcare responsibilities should not rely on increasing the “quantity” of clinics, but rather on enhancing the “quality” of medical standards.
In the past, some clinics with irregular diagnostic and treatment practices and poor medical quality left patients with an impression of distrust, affecting the healthy development of the entire industry. Under the overall principle of relaxed entry but strict regulation in the new regulations, the clinic industry is bound to face such a restructuring trend: small clinics that do not meet the requirements for physician titles, have low diagnostic and treatment capabilities, abuse drugs, and have irregular operational management will be eliminated; clinics that focus on improving medical service levels and business philosophies, and are patient-centered, will be more competitive. At the same time, these clinics can also gain more trust from patients, enhance patients' trust in the clinic industry, and promote the healthy development of the industry.
Multifaceted Industry Impact
The “Opinions” propose a two-year pilot program in ten cities to refine policies on clinic establishment and management based on pilot experiences. The program will also involve timely evaluation of pilot implementation, strengthened operational guidance and supervisory assessments, the prompt dissemination of advanced practices from pilot areas, and the formulation and issuance of policy measures to promote the development of clinics across China.
It is foreseeable that after the new regulations enter the nationwide promotion phase, although specific measures may be adjusted based on practical experiences encountered during the pilot programs, the overarching directions—optimizing access procedures, improving healthcare quality, and strengthening supervision—will remain unchanged. In light of these requirements, we believe that the pilot implementation and nationwide rollout of the new regulations are not only relevant to clinics themselves but may also impact other niche sectors. For example:
Expanded Scope of Third-Party Collaboration: Third-Party Medical Institutions Can Provide More Services to Reduce Clinic CostsUnder the new clinic standards, clinics that enter into relevant service agreements with other medical institutions for clinical laboratory testing, medical imaging, electrocardiography (ECG), pathology, and sterile supply services are not required to equip themselves with the corresponding equipment. Compared to the 2010 version, ECG, pathology, and medical imaging have been added to this list. This means that clinics no longer need to purchase the aforementioned equipment, as these services can be provided by third-party medical institutions.
As previously mentioned, despite the significant upfront investments made due to the simplified clinic access process, the risk of non-compliance during the filing stage remains. Therefore, by strengthening collaborations with clinics, third-party medical institutions can enable clinics to operate under an asset-light model, thereby minimizing potential losses should any issues arise during the filing process.
Meanwhile, as clinics are required to establish information systems and achieve interoperability with the medical service regulatory information system, IT enterprises will play a more significant role in enhancing clinic informatization, facilitating data integration with regulatory authorities, and ensuring data security.