Riding the DRG Tailwind: How Hospitals and Health Insurance Can Navigate the Great Reform
2019 marked the tenth year since the launch of China’s new healthcare reform. Internet-enabled tiered diagnosis and treatment progressed steadily, yielding remarkable achievements. However, at this juncture, the National Healthcare Security Administration (NHSA), as the ultimate payer, faced a major test.
“The 2019 HIA Hospital Operations Analysis Report” described the current medical insurance environment as follows: More than half of the regions in China have experienced deficits in their medical insurance funds. Taking Liaoning Province as an example, in 2018, only Shenyang and Dalian among its 14 prefecture-level cities maintained a balance in their medical insurance funds, while the remaining 12 cities faced expenditures exceeding revenues after November.
In this regard, the National Healthcare Security Administration (NHSA) has been preparing for quite some time. On October 24, the NHSA issued the technical standard titled “National Healthcare Security DRG (CHS-DRG) Grouping Scheme.” This move provided an official template for DRG (Diagnosis-Related Groups) classification, which had previously been characterized by a multitude of competing approaches. It is now certain that DRG will serve as the basis for healthcare insurance reimbursements.
Currently, 30 cities have been designated as national pilot cities for DRG-based payment, with simulated operations required in 2020 and actual implementation launched in 2021. Subsequently, various news reports emerged: Zhejiang Province is poised to become the first province in China to implement a unified provincial DRG point-based payment system; and 74 medical institutions in Wuhan have been identified as the first batch of national pilot units for DRG-based payment.
So, in the context of policy-driven momentum, can enterprises enter the market to further promote medical insurance payments? To explore this question, VCBeat interviewed several experts deeply engaged in DRG (Diagnosis-Related Groups), attempting to analyze the potential market emerging under the policy from both short-term and long-term perspectives.
In the vast majority of regions, the DRG grouper is led by the state, with major enterprises such as Neusoft, Guoxin, and Ping An assisting in its development, thereby ensuring the scientific rigor of base rates for diseases. However, the completion of the grouper’s formulation does not mean that all concerns are alleviated.
CHS-DRG coding is based on ICD-10, while procedure coding adopts the ICD-9-CM-3 version. Local DRG variants modeled after this framework differ in structure, but the codes that influence DRG case grouping remain consistent to a certain extent.
Taking "community-acquired pneumonia" as an example, its code in the ICD-10 Clinical Version 2.0 is J15.902, indicating unspecified bacterial pneumonia. According to the structure of ICD-10, the letter "J" represents diseases of the respiratory system. The first three characters, "J15," constitute the category, and the first four characters, "J15.9," represent the subcategory. These elements form the core components of the code, which are standardized internationally. Characters from the fifth position onward are referred to as subdivisions. With the exception of a few internationally standardized subdivisions, countries may expand upon these, which accounts for the diversity and main differences among various versions of ICD-10 codes in China. In the case of community-acquired pneumonia, the ".9" denotes a "residual category" (which also includes .8 and other subcategories with titles containing "other" or "unspecified"). This refers to conditions that cannot be classified under other specified subcategories within the same category and serves primarily as a catch-all. Generally, hospitals are advised against using residual category codes. Instead, they should determine the correct category and subcategory based on the central axis of the disease to accurately reflect the diagnosis and treatment provided.
Therefore, from the perspective of permutations and combinations, disease grouping is not particularly complex; the complexity lies in case assignment and base rate calculation. The core issue resides in the raw data.
Among the 26 national monitoring indicators, seven are automatically extracted from the front sheet of medical records, accounting for 26.92%. However, data released this September by Wang Yi, Director of the Medical Records Department at Peking Union Medical College Hospital, showed that the accuracy rate of front sheet completion for key medical records in Beijing municipal hospitals was 79.27% in 2018; yet, when cross-referenced with the full clinical documentation within the medical records, this figure would be significantly lower than 79.27%. If there are inaccuracies in the front sheet of medical records, the resulting case grouping, assignment to diagnosis-related groups (DRGs), and base rate calculations derived from these data will deviate from reality to some extent.
"Most errors on the medical record face sheet, whether coding or non-coding, can only be accurately identified by reviewing the medical records," stated Zhou Yutong, CEO of Yisheng Intelligence, in an interview.
“Medical records are the fundamental basis for medical practices. The medical record summary is, in fact, a part of the medical record, serving as its abstract; the abstract must be consistent with the main text, and only without deviation does it hold significance. Therefore, the foundational condition for the implementation of Diagnosis-Related Groups (DRG) is the accuracy of the entire medical record, not merely the accuracy of the medical record face sheet. This point must be clarified. We cannot conclude that the quality of diagnosis and treatment fails to meet standards simply because the diagnoses and procedure names on the coding or medical record face sheet do not comply with ICD or DRG requirements. After all, clinical diagnostics and disease classification are distinct disciplines with substantial differences between them; clinicians are neither familiar with nor have the capacity to fully understand ICD requirements. Thus, quality control physicians and coders must assist clinical staff in accurately reflecting the patient’s actual diagnosis and treatment through proper coding. What needs to be reviewed? The complete medical record.”
In this regard, Zhou Yutong cited the following four examples:
“For oncology patients, the selection of the principal diagnosis varies depending on the primary reason for the visit. If a patient is admitted for the confirmation of a primary tumor, the principal diagnosis must be the chemotherapy regimen if chemotherapy is administered during this admission, regardless of whether it was initially selected as the principal diagnosis. Conversely, for cancer patients admitted specifically to undergo chemotherapy or radiotherapy, chemotherapy or radiotherapy should be designated as the principal diagnosis. This issue of principal diagnosis selection can only be determined by analyzing the medical records to identify the primary reason for the visit. It is incorrect to assume that chemotherapy is the purpose of the current visit simply because both a chemotherapy-related diagnosis and a tumor diagnosis are listed on the front page of the medical record.”
The coding differs between singleton vaginal deliveries and multiple gestation cesarean sections; furthermore, codes vary among singleton, twin, and triplet pregnancies. If physicians document only “pregnancy” or “delivery,” the medical record must be reviewed to determine the actual clinical circumstances.
In cardiac surgery, the coding for coronary artery bypass grafting (CABG) varies depending on whether one, two, or more arteries are grafted. The specific number of arteries involved must be confirmed in the operative report to determine the correct code; it is insufficient to rely solely on the general term "coronary artery bypass grafting."
Revisiting Burns: The Core of Burn Coding Is Anatomical Site, Followed by Severity. Different Sites and Severities Warrant Different Codes and Clinical Representations. We Often Encounter Front Sheets Documenting “10% Third-Degree Burns and 90% Second-Degree Burns, with Burns at a Specific Site.” How Should Coders Assign Codes? Is the Affected Site Classified as Third-Degree or Second-Degree Burn? Which Should Be Designated as the Principal Diagnosis? This Depends on How the Medical Record Is Documented.
In short, different enrollment methods correspond to different base rates. If physicians document in the manner described above, it often leads to undercoding, ultimately resulting in financial losses for the hospital and reduced performance-based compensation for physicians.
Therefore, hospitals should reduce the substantial losses caused by under-coding in Diagnosis-Related Groups (DRGs) by strengthening quality control. Currently, under-coding is a widespread issue in hospitals, whereas over-coding constitutes insurance fraud and is not typical. However, there are no mandatory national requirements regarding the number of hospital quality control personnel. Under current circumstances, most hospitals employ only 3–4 coders and 1–2 medical record quality control staff.
Compared with international data, coders in the United States and Australia encode 4–5 medical records per day, whereas in China, taking Jilin Province as an example, the reported average is 15 records per day, with actual workloads sometimes reaching 50 records per day. As evident from the aforementioned scenario, to ensure the quality of case-mix grouping, coders/quality control specialists must not only review the front sheet of the medical record but also conduct a page-by-page comparison with the underlying clinical documentation. This reveals a severe mismatch between demand and supply.
Human resources constitute another challenge facing hospital medical records departments. The ability to identify errors within a vast array of medical records, each containing diverse types of mistakes, actually demands a high level of professional expertise from coders and quality control specialists. In China, the academic training for coders and quality control personnel has historically been dominated by associate degree programs; undergraduate majors in this field have only been introduced in recent years. However, hospitals require coders and quality control specialists with a background in clinical medicine. In reality, however, how many professionals with clinical medicine qualifications would be willing to work solely as coders or quality control specialists?
The aforementioned three issues do not directly impact healthcare insurance expenditures; in fact, given the widespread under-staffing and under-budgeting in hospitals, the Healthcare Security Administration may achieve savings that exceed initial projections. However, in the long run, such under-resourcing will ultimately erode hospitals’ motivation to implement policies.
Therefore, to ensure that DRG truly exerts its intended effect, a balance must be achieved between hospitals and the Healthcare Security Administration.
In summary, whether addressing issues with case grouping, base rate calculations, or talent shortages, the common objective is to achieve data standardization while ensuring efficiency. By allocating sufficient human resources to the medical record review process, errors in case grouping can be mitigated; as the error rate in medical records decreases, the issue of under-coding in hospitals will be readily resolved.
Therefore, many companies currently offer digital solutions for medical record quality control, either by applying rule-based mapping under big data frameworks or by leveraging NLP technology for intelligent processing. The ultimate goal is to achieve automatic ICD coding assignment at the time of patient grouping; automatically determine the principal diagnosis in cases of multiple diagnoses; intelligently merge codes and optimize costs reasonably; and conduct post-grouping data audits and coding accuracy verification. These solutions also assist hospitals in internal performance evaluation, insurance payment and settlement, and regulatory audits for insurance compliance.
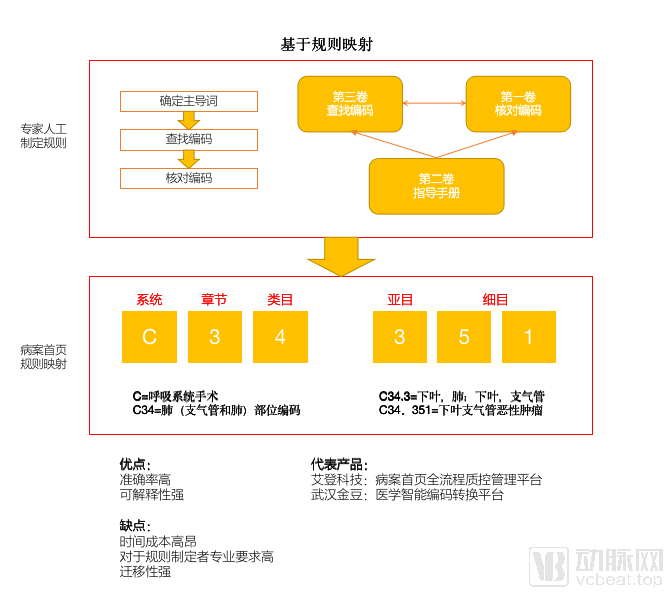
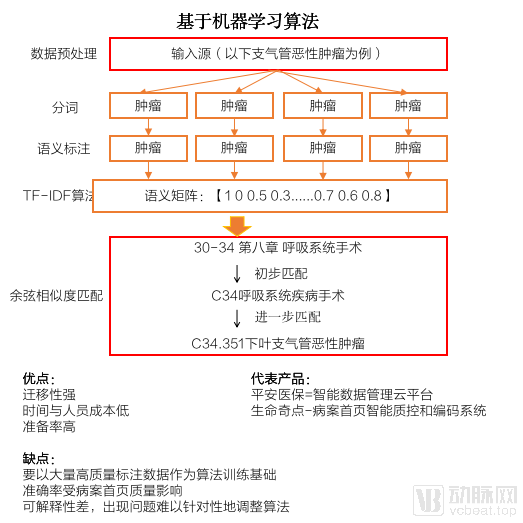
Comparison of Two Data Processing Methods (Image provided by Liu Zhichen)
NLP comprises a multitude of knowledge components, replacing the point-to-point linear logical relationships found in traditional quality control systems with human brain-like logical processing. Based on this algorithm, the system no longer operates on a “single-point input, single-point output” model; instead, it integrates patients’ existing medical record information to generate diagnostic judgments, enabling computers to understand, analyze, and process unstructured text.
For example: If a physician initially diagnoses a patient with hypomenorrhea and abdominal pain, but subsequent testing—specifically serum human chorionic gonadotropin (HCG) levels and gynecological ultrasound—confirms an ectopic pregnancy, there is clearly a commonsense error in the diagnostic sequence. Since menstruation does not normally occur during pregnancy, natural language processing (NLP) systems can leverage logical reasoning to provide clinical decision support alerts to the physician.
Liu Zhichen, a senior expert in the field of Diagnosis-Related Groups (DRG) in China and a joint postdoctoral fellow at Fudan University’s Public Administration Mobile Station, believes that Natural Language Processing (NLP) typically relies on rule-based approaches. This involves leveraging extensive accumulated medical knowledge to align and match processed text with standard coding descriptions through coding logic and rules, thereby achieving accurate coding. The construction of such logic and rules depends on content information from various sections of electronic medical records, including patient demographics (gender, age), clinical diagnoses, surgical procedures, imaging findings, and pathological information. Such algorithmic coding delivers high performance and strong interpretability of the coding pathway, effectively meeting the practical needs of physicians.
Taking companies such as Huimei Technology and Yisheng Intelligence as examples, they have all developed their own disease knowledge graphs capable of processing a certain range of diseases and correcting inconsistencies in sequential data as well as errors that defy common sense. However, coding items are highly fragmented; due to the complex logic of complications or the unique characteristics of medical record documentation in specific regions, natural language processing (NLP) still has certain limitations. Both the algorithmic logic of knowledge graphs and the volume of knowledge points require further enhancement.
The Economist once wrote in its article “Getting Old Before Getting Rich”: “Never mind the bad loans and trade wars... demographics may be the biggest challenge facing China’s economy.” At present, the Diagnosis-Related Group (DRG) model adopted by Germany, which faces a similarly severe aging problem, could serve as a relatively mature reference for China.
Germany was the first country in the world to implement a social security system through social legislation, enacting three key laws: the Health Insurance Act in 1883, the Accident Insurance Act in 1884, and the Disability and Old Age Insurance Act in 1889.
To address the surplus of public hospitals, enhance hospital efficiency and competitiveness, and alleviate the medical pressure caused by an aging population, Germany established the InEK (Institute for the Hospital Remuneration System) in 2001. Drawing on Australia’s DRG system, Germany further optimized and developed the G-DRG system for health insurance reimbursement.
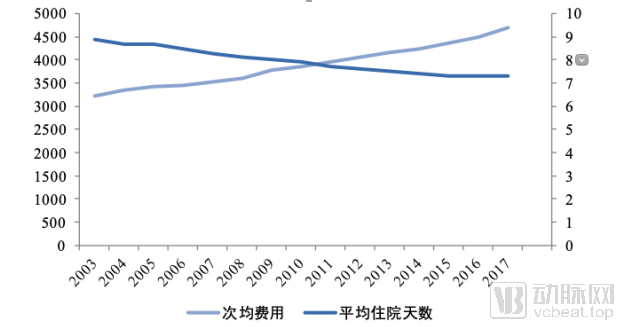
Image source: “A 16-Year Review and Lessons Learned from the Implementation of the German G-DRG Hospital Reimbursement System,” by Jiang Yishi and Shao Xiaojun
As can be seen from the figure above, since the implementation of Diagnosis-Related Groups (DRG) in Germany in 2003, the average length of hospital stay has shown a continuous downward trend, resulting in controlled growth in health insurance expenditures. However, theoretically, DRG should drive a year-on-year decrease in the average cost per case, yet the statistical curve continues to rise. Population aging is the underlying reason for this phenomenon.
“Germany is a country with a severe aging population, and the hospitalization costs for the elderly are significantly higher than those for younger people. Therefore, as population aging continues to advance and medical technology keeps developing, although patients’ average length of stay is decreasing, the high medical expenses incurred by the elderly have driven up the average cost per medical encounter. China faces a similar situation, yet its current health insurance structure is ill-equipped to address this challenge,” explained Shao Xiaojun, Chief Medical Officer of the Health and Elderly Care Business Center at Pacific Insurance.
Fundamentally, the challenges facing medical insurance stem not only from over-treatment but also from population aging, which will exert significant pressure on the system for an extended period. Therefore, relying solely on DRG-based cost containment is insufficient; expanding revenue streams through commercial insurance may offer a more sustainable solution.
Innovative payment has emerged as a highly popular niche segment in the healthcare sector over the past two years. Commercial insurance institutions, with health insurance products at their core, have long been deeply entrenched in the medical field. However, due to limited current business penetration and challenges such as the lack of transparent data accounting, they remain in the early exploratory stage. Nevertheless, for Diagnosis-Related Groups (DRG), commercial insurance serves as a crucial supplement to address the shortcomings of basic medical insurance.
“State Council policies have stipulated that critical illness insurance should be underwritten by commercial insurers. However, under the current mechanism, insurers can only set deductibles based on specific severe conditions. For example, if medical expenses for certain severe conditions exceed RMB 100,000, insurers cover 50% of the costs; if they exceed RMB 200,000, coverage rises to 100%. This policy framework is based on fee-for-service payment models. China’s commercial health insurance sector remains immature, covering only specific types of cancer, while there are hardly any sustainable reimbursement schemes for chronic diseases such as hypertension and diabetes. Due to factors like unpredictable hospital stays and variations in medical services, the underlying costs are extremely difficult to calculate,” said Shao Xiaojun.
Therefore, to enable commercial health insurance to supplement basic medical insurance, DRG must first establish a solid payment foundation.
On the premise of ensuring the accuracy of medical record data, the implementation of Diagnosis-Related Groups (DRG) in hospitals is essentially a non-zero-sum game between hospitals and the Healthcare Security Administration. Initially, issues such as undercoding or upcoding may arise; however, since DRG settlement is conducted on a monthly basis, DRG weights undergo a continuous dynamic adjustment process. If the Healthcare Security Administration observes that the treatment costs for a specific disease fall outside the expected range, it can promptly adjust the disease weight.
Through continuous data refinement and ongoing adjustment of base rates, DRG payment rates will converge toward a benchmark accepted by both hospitals and the National Healthcare Security Administration. In this way, DRG simulation will establish a well-organized and transparent payment system, providing health insurance companies with the actuarial and risk-control data foundation they require.
With a clear budget for the cost of individual diseases, insurance companies have an actuarial basis to unbundle coverage responsibilities and isolate uncertainty. This enables more precise pricing and product design under different coverage scenarios to address future claims uncertainty, ultimately driving product pricing.
Based on this approach, new health insurance products are not limited to costly oncology coverage. They break the traditional restriction of insuring only healthy individuals by extending coverage to those with pre-existing conditions. Through the effective utilization of DRG data—such as weighting factors, costs, and length of stay—single-disease policies for common chronic conditions like diabetes and hypertension can be reasonably structured and managed.
The relationship between DRG and health insurance extends beyond mere revenue generation and cost containment. DRG provides the actuarial foundation for health insurance, while health insurance offers supplementary payment support to the medical insurance reimbursement schemes implemented under DRG.
However, restructuring the health insurance system under the DRG framework still presents certain challenges. Shanghai Shanzhen believes that the following five changes must be taken into account:
I. Changes in the Pricing Basis for Medical Insurance: DRG primarily impacts inpatient costs; therefore, the pricing and deductible design basis for million-yuan medical insurance products, where inpatient care constitutes the primary coverage responsibility, will undergo changes.
II. Uncertainty in Claims Arising from the Implementation Process: The rollout of DRG payment reform is a gradual process. Variations in adoption by medical institutions, utilization patterns of commercial health insurance by patients and physicians, and regional differences in implementation and usage all contribute to uncertainty in medical insurance claims payouts.
III. Claims may decline with short-term volatility but rise in the long term: Due to the cost-containment effect of Diagnosis-Related Groups (DRG) on inpatient expenses, claim payments may experience a volatile decline in the short term. However, as physicians and patients develop a more mature understanding of commercial health insurance, differences in treatment approaches may emerge between those with and without such coverage. In the long run, this will lead to higher claims payouts for commercial health insurance, while also significantly enhancing consumers’ awareness of its value.
IV. The challenges in pricing design for guaranteed-renewal medical insurance products will increase significantly: As the implementation of Diagnosis-Related Groups (DRG) drives changes in healthcare consumption behaviors, regional variations will greatly complicate long-term cost projections.
5. Pricing Disparities Among Insurance Products from Different Insurers Will Widen: Due to varying levels of understanding and actuarial capability regarding future claims uncertainty, significant pricing differences for identical products may emerge in the market.
From a macro perspective, short-term claims will experience fluctuations, while long-term claims depend on users’ acceptance of commercial medical insurance. However, as the Diagnosis-Related Group (DRG) payment system is further implemented, premiums for medical insurance will see substantial growth, and it is inevitable that they will surpass those for critical illness insurance in the future. In this context, insurers’ capability to research medical services will become increasingly important, the healthcare service attribute of health insurance will grow more prominent, and this sector will become increasingly competitive.
Medical record quality control and health insurance are two areas significantly impacted by the current implementation of DRG, with a strong emphasis on enterprises’ actual service capabilities. Meanwhile, many other sectors also need to adopt responsive measures amid the reform.
Of particular note is the response from hospitals to the implementation of Diagnosis-Related Groups (DRGs). To control medical costs, physicians are opting for more rational use of medications and consumables. Proprietary Chinese medicines and traditional Chinese medicine injections may be adversely affected due to their slower onset of action, while generic drugs and conventional pharmaceuticals may see increased sales driven by the “4+7” volume-based procurement policy.
Other niche areas, such as data-driven “AI + CDSS” and “AI-assisted diagnosis,” will likewise benefit from data standardization; however, due to the difficulties in data acquisition, these fields are unlikely to be significantly impacted in the short term.
DRG reform is a long-term process, with every country advancing through a continuous cycle of identifying errors, refining systems, and re-identifying errors. Issues such as data gaps, physicians’ limited awareness, and the parallel implementation of dual DRG grouping systems by both the National Healthcare Security Administration and the National Health Commission continue to challenge stakeholders. However, answers can be found for all visible problems; in the coming period, the government, hospitals, physicians, and enterprises must jointly explore and address emerging unknowns.
This process is a long and arduous journey.