Value-Based Healthcare in China: White Paper Launch and Pathways to Leapfrog Development
Value-based healthcare, or high-cost-effectiveness medical services, represents a trade-off between healthcare expenditure and clinical outcomes.
On November 23, 2019, the 3rd International Health Finance Summit, themed “Healthcare Reform and Payment Innovation,” was held in Shanghai. Dozens of government officials, academics, executives from innovative enterprises in the industry, and experts from home and abroad gathered to discuss policy and industry hotspots, including health insurance reform, policy innovation in the public healthcare security system, and innovations in commercial insurance and other commercial payment mechanisms. As one of the highlight segments of the forum, the 2019 White Paper on Value-Based Healthcare in China was officially released.
Li Qun, Deputy Director of the Health Finance Research Office at Fudan University’s School of Management and Senior Director of Research and Consulting for iShouKang China, began by interpreting medical payment and value-based healthcare at the forum that day.
Value-based healthcare is a concept imported from abroad, originating in developed countries in Europe and North America. What significance does value-based healthcare hold for developing countries or low- and middle-income countries?
At the 2014 World Health Assembly, the World Health Organization (WHO) estimated that low- and middle-income countries spent $850 billion annually on healthcare. Of this, clearly effective medical technologies accounted for 13%, potentially effective technologies for 22%, while wasteful healthcare expenditures reached 20–40%. This translates to an annual waste of $250 billion in healthcare spending in low- and middle-income countries, indicating widespread inefficiencies in resource utilization and quality issues within their healthcare systems.
From the perspective of population health, value is defined as the ratio of a series of clinical outcomes centered on patient disease to the total healthcare costs incurred throughout the entire care process. Healthcare expenditures and clinical outcomes are the two focal points of value-based healthcare and serve as the criteria for assessing whether medical services are “valuable.”
It is understood that in low- and middle-income countries, improving public health and medical services could prevent approximately 16 million deaths. Value-based healthcare can play a significant role in enhancing the quality of medical services, increasing patient health literacy, and advancing public health service levels.
Li Qun pointed out that the following elements are indispensable for promoting understanding of healthcare value among all stakeholders within the healthcare system and driving transformation.
First, the transformation of the payment system,Shift from traditional fee-for-service to value-based healthcare payment.
Second, the transformation of the medical service system,Healthcare institutions should redefine their positioning and organizational frameworks around medical value. Taking diabetes as an example, hospitals should not focus solely on metrics such as blood glucose control; instead, they should encompass comprehensive care throughout the entire disease course—including early intervention, lifestyle guidance, management of acute events, and complication control—along with associated healthcare outcome indicators.
Third, establish a solid foundation in medical informatics.Establish clinical efficacy and health outcome standards, along with corresponding information systems, for selected disease areas and patient populations to enable systematic data collection, sharing, and analysis.
Fourth, conduct benchmarking analysis, research, and medical informatics-related work., based on the aforementioned data analysis, conduct benchmarking analyses focusing on clinical efficacy and best practices to drive continuous improvement in clinical practice and healthcare delivery models; explore new data sources and innovative clinical trials, and develop clinical decision support systems, among other initiatives.
“Interconnected data serves as the foundation. Without data and benchmarking studies, the transformation of payment systems and healthcare services will be unsustainable,” said Li Qun.
With the advancement of national institutional reforms and the implementation of several major healthcare reform measures, value-based healthcare has become a focal point in the medical industry. However, due to challenges such as fragmented healthcare services, the lack of standardized clinical outcome metrics and medical data, and the continued reliance on traditional fee-for-service payment models by health insurance payers, the widespread adoption of value-based healthcare in China still requires concerted efforts from multiple stakeholders.
To this end, the Health Finance Research Office of Fudan University and iShoukang jointly released the white paper “Value-Based Healthcare in China: How to Promote Industry Collaboration and Business Model Innovation, and Accelerate the Transformation of the Healthcare System.” The white paper explores international case studies on the implementation of value-based healthcare, aiming to encourage participation from industry stakeholders, patients, and third-party payers, and to leverage the effectiveness of platform institutions to facilitate the execution of specific projects. Li Qun provided an interpretation of the white paper.
China's Medical Insurance Expenditure Is Not Proportional to Its Utilization Efficiency
The white paper analyzes the current state of healthcare services in developing countries, based on data released by the Organisation for Economic Co-operation and Development (OECD) in 2016.
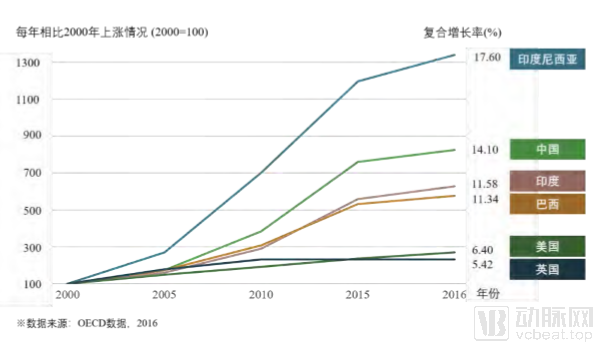
Rapidly Rising Healthcare Costs in Developing Countries (Image from the White Paper)
As shown in the figure, China’s healthcare expenditures have risen rapidly when measured as a percentage of GDP. Since 2000, the rate of increase in China has been more than three times that of European and American countries. The white paper notes that, in reviewing the first decade of China’s new healthcare reform, scholars including Ye Zhimin recently published an analysis in The Lancet, which found that from 2008 to 2017, government spending on healthcare in China increased from RMB 359 billion to RMB 1.52 trillion. The share of general government health expenditure (GHE) in total government expenditure rose from 5.7% in 2008 to 7.5% in 2017, and health insurance coverage improved significantly.
Li Qun noted that during the previous round of healthcare reform in China, pharmaceutical expenditures rose rapidly, significantly expanding national health insurance coverage. However, there remains substantial room for improvement in the efficiency and effectiveness of fund utilization. The majority of basic medical insurance resources in China are concentrated in hospitals, while primary healthcare institutions, pharmacies, and other entities account for only 20% of health insurance spending, resulting in low efficiency and effectiveness in the use of healthcare expenditures.
Furthermore, China’s effectiveness in chronic disease prevention and control remains suboptimal. Taking cardiovascular and cerebrovascular diseases as an example, from 2014 to 2016, the annual growth rate of treatment costs for these conditions was 15.5%, amounting to an increase of RMB 123.7 billion, which accounted for 25.6% of the total increase in treatment costs during the same period. In 2016, China’s expenditure on the treatment of cardiovascular and cerebrovascular diseases reached RMB 495.2 billion. The average age of patients with these conditions is 61 years; they suffer from an average of 4.2 comorbidities per person, and utilize an average of 36 different medications annually. Although insured individuals among this patient population account for only 5%, they consume 51% of the basic medical insurance fund, underscoring the substantial financial burden borne by both individuals and the insurance fund.
Li Qun analyzed the problems existing in China's current medical system.
Currently, China's healthcare services are hospital- and physician-centric, with hospitals prioritizing service volume and revenue, thereby being heavily driven by financial incentives.Faced with challenges such as chronic diseases, healthcare service institutions remain relatively fragmented, with scarce basic resources and capabilities, and a lack of incentives for integrated services and improving population health. In short, the existing healthcare service system makes it difficult to prioritize medical value.
Secondly, traditional payment and incentive mechanisms fail to drive the measurement and continuous improvement of healthcare value.Health insurance reimbursement is based on service volume, lacking measurement of medical outcomes. This tends to lead to overutilization of health services and medical resources, making it difficult to reflect the value of medical services and technologies. Furthermore, the absence of systematic mechanisms for market access, long-term evaluation, and adjustment can easily result in the irrational use of medical technologies and waste of insurance funds.
Third, the lack of medical outcome assessment and benchmarking results in an absent foundation for measuring medical value.Although healthcare institutions have a high level of informatization, medical data remains fragmented across isolated information silos, and the lack of interoperability has become, to some extent, an obstacle to building an integrated healthcare system.
The transformation of healthcare systems is a long-term and complex process. Western countries have taken the first step, and we may find our own path by learning from their practical experiences.
Explorations in European and American Countries
To gauge global progress in value-based healthcare, the Economist Intelligence Unit (EIU), a research division under The Economist Group, conducted a study in 2016. It assessed 25 countries across four indicators: policy environment, patient-centered integrated care systems, systematic measurement of health outcomes and expenditures, and outcome-based payment models. The survey results indicate that China’s overall progress across the four dimensions of value-based healthcare is relatively optimistic, making it the only BRICS nation to rank in the second tier. The first tier remains dominated by traditional Anglo-American countries such as the United Kingdom and the United States.
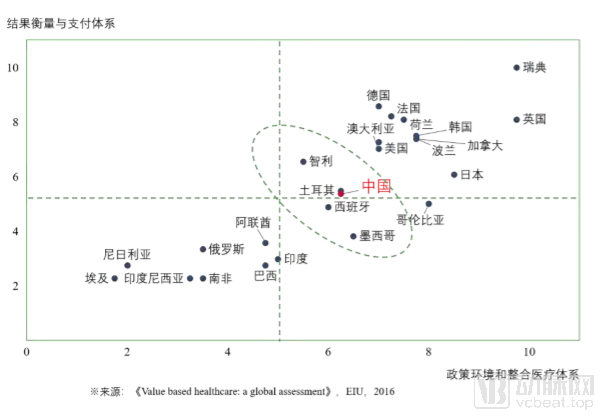
EIU’s Assessment of Progress in Value-Based Healthcare Reforms Across 25 Countries (Image from the White Paper)
The chart indicates that developed countries in Europe and the United States have made significant progress across multiple dimensions, while developing countries, including China, have also completed high-quality upgrades to their healthcare systems. On the other hand, many countries, including BRICS nations such as India, Russia, and Brazil, still have considerable room for improvement in various aspects.
In 2010, Obama signed the Patient Protection and Affordable Care Act (the “ACA”), officially launching a new round of healthcare reform in the United States.
The U.S. healthcare system is highly complex. Viewed through the analytical framework of “medical care, pharmaceuticals, and health insurance” commonly used in China, the United States’ transition toward value-based care can be characterized by two key developments: the transformation of its healthcare delivery system and payment models toward value-oriented approaches, and the establishment of a value assessment framework for health technology assessment (HTA) to guide pharmaceutical market access. In this process, the Centers for Medicare & Medicaid Services (CMS), the federal agency administering public health insurance programs, and the Institute for Clinical and Economic Review (ICER), an independent nonprofit organization conducting HTA research and policy analysis, have played leading and guiding roles.
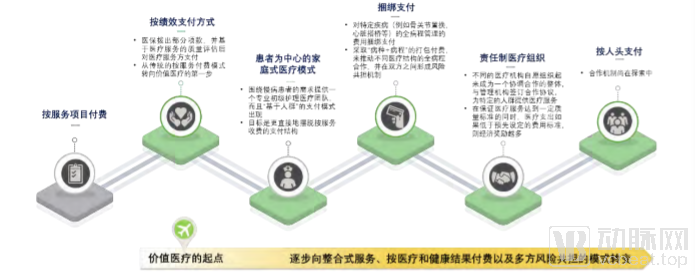
Comparison of Various Value-Based Care Programs in the U.S. (Image from the White Paper)
The U.S. “healthcare reform” is proceeding in an orderly manner along a path characterized by the National Health Insurance Agency as the primary driver, government leadership, legislative foundation, and private sector participation. Within this complex system, the Centers for Medicare & Medicaid Services (CMS) has developed a roadmap to guide stakeholder engagement and help the public understand the evaluation framework.
“This system is highly complex. It begins with the Value-Based Payment (VBP) mechanism for home-based medical services and the performance evaluation framework for physicians contracted with the Centers for Medicare & Medicaid Services (CMS). Next, it involves upgrading care delivery systems and reforming payment models for chronic diseases and surgical procedures, ultimately evolving into Accountable Care Organizations (ACOs). ‘This system can be simply understood as China’s Medical Consortium model,’ said Li Qun. In this model, healthcare institutions collaborate to assume responsibility for the health of a defined population or geographic region, enter into performance-based agreements, and aim to transition toward a capitation payment model.”
For each CMS initiative, a partner organization is selected and monitored over a three- to five-year period, with program outcomes evaluated using an evidence-based approach. Data from 2019 indicate that there were approximately 1,600 Accountable Care Organizations (ACOs) nationwide in the United States, serving 14 million beneficiaries. Comparisons with control groups revealed varying degrees of improvement in both healthcare quality and expenditures.
In Europe, healthcare reforms in the United Kingdom and the Netherlands share a common feature: a strong emphasis on evaluating healthcare outcomes within national strategies. Taking a UK initiative as an example, both patients and health administrators can log in to access data on clinical outcomes for various diseases, hospital performance metrics, and the operational performance of individual healthcare institutions. The transparent disclosure of such data has fostered healthy competition. The Netherlands has also launched similar initiatives, mandating under its national strategy that precise assessments of healthcare outcomes be conducted for more than 50% of all disease conditions nationwide within a five-year period.
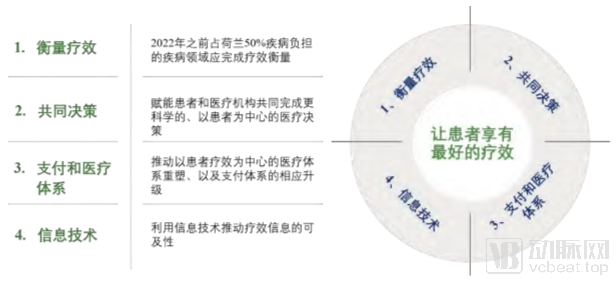
Four Action Plans of the Netherlands’ Five-Year Plan (Image from the White Paper)
In Europe and the United States, collaboration with healthcare institutions has facilitated the transformation of pharmaceutical divisions from cost centers to value centers, thereby helping healthcare providers reduce expenses. Consequently, pharmaceutical companies, commercial insurance firms, and health IT enterprises have become increasingly prominent in the process of healthcare reform. Although China’s healthcare system and stage of development differ significantly from those of Western countries, and its development path cannot be simply replicated, valuable lessons can still be drawn from their successful experiences to avoid unnecessary detours.
The experiences of European and American countries offer valuable lessons for China’s healthcare reform. First, China should establish a clear roadmap that includes promoting pilot projects in the initial phase and replicating and scaling them up in later stages, thereby advancing reforms in an orderly, phased manner. Second, reforms should be driven through legislation and national strategy; legislative measures and other mechanisms should facilitate coordination among all stakeholders, designate leading institutions, and allocate necessary resources. Third, attention should be focused on systemic reform rather than piecemeal improvements. While localized tweaks and fragmented policies may yield short-term gains, they cannot sustainably drive comprehensive system upgrades over the long term and may ultimately produce counterproductive outcomes.
It is worth noting that, in addition to the three points mentioned above, the rigorous standards for evidence-based assessment adopted by European and American countries are also worthy of emulation. On one hand, these countries prioritize evidence-based evaluation through pilot iterations; their pilot programs undergo internal third-party assessments before being scaled up nationally. By establishing evidence-based evaluations and conducting health economic assessments, they provide technical evidence and benchmarking standards to facilitate project implementation. On the other hand, the complexity of healthcare systems necessitates multi-stakeholder engagement and public-private partnerships, involving payers, healthcare providers, pharmaceutical companies, and health IT enterprises, thereby promoting transparent and fair upgrades across the entire system.
In the new round of healthcare reform, the government has promoted systemic transformation, including shifting toward medical consortiums and transitioning to a value-driven strategic purchasing model for health insurance payments. Li Qun stated that he hopes to encourage active participation from multiple stakeholders in the industry in this new wave of healthcare reform.
Currently, the goal of biopharmaceuticals and medical devices is to promote a value-based access system, ultimately achieving innovative payment models to reach a triple-win outcome for the healthcare insurance system, patients, and the industry.
Currently, the practice of value-based healthcare within China’s pharmaceutical and medical device industry is primarily manifested in the medical products provided by enterprises and their integrated services that “go beyond the product.” From offering safe, efficient, and high-value pharmaceutical and medical device products, to driving payment innovations for high-value medical products and providing value-added health services, and further to delivering patient-centered holistic solutions, pharmaceutical and medical device companies are continuously refining their product-service offerings and enhancing the level of integration across the industrial chain.
Li Qun noted that commercial health insurance has experienced rapid growth over the past two years, with its primary value lying in extending coverage to previously uninsured populations while maintaining coverage for existing insured groups.
Currently, commercial health insurance has primarily explored value-based healthcare in three areas: initial forays into proactive management, reflected in health insurance products that integrate value-added health services; linking claims payments to treatment outcomes, a measure mainly applied to efficacy insurance for pharmaceuticals and medical devices; and transitioning toward managed care health insurance, exemplified by innovative single-disease management health insurance products, such as those providing whole-course disease management and long-term event risk coverage for chronic patients insured with pre-existing conditions. Taikang Insurance serves as an innovative case study in this regard.
Taikang Insurance is a representative enterprise in China’s transition of health insurance from a payer model to managed care. Taikang Insurance possesses core capabilities in establishing clinical pathways, system development, data accumulation, provider-patient operations, and disease management, while actively exploring entry points for collaboration with public medical insurance programs and public healthcare institutions. “They aim to adopt the Chinese Kaiser Permanente model, which will serve as the leverage point for future cooperation between commercial insurers and public medical institutions.”
In the information technology industry, numerous unicorn companies have emerged in recent years, with Neusoft Wanghai being one of them.
Neusoft Wanghai has deeply cultivated the field of lean hospital management, providing comprehensive operational management systems for healthcare institutions to facilitate the continuous advancement of refined hospital management. With the implementation of Diagnosis-Related Groups (DRG) and the ongoing promotion of value-based healthcare concepts in China, Neusoft Wanghai has gradually extended its business operations into these areas.
As the central vehicle of the DRG payment system, a hospital’s core competitiveness will lie in its ability to reduce operating costs through lean operations while ensuring service quality within the new framework. Neusoft Wanghai has refined ex-ante planning through “DRG + Budgeting,” optimized resource allocation via “DRG + Costing,” and enhanced management effectiveness with “DRG + Performance Management.” To date, it has assisted nearly 200 hospitals and close to 50 government agencies in implementing DRG systems.
To promote the sharing and collaboration of healthcare data, Neusoft Wanghai established the HIA Health Information Alliance, which has currently brought together more than 1,500 large medical institutions across China. The alliance analyzes hospital operations from multiple dimensions—including hospitals, departments, and disease types—and provides member hospitals with industry benchmarking data and recommendations for operational improvement.
The past decade of China’s new healthcare reform has coincided with a decade of global promotion of value-based healthcare. Li Qun stated that in communications with numerous digital health companies, it was found that many enterprises’ technologies and business models lack data and evidence demonstrating a positive impact on the healthcare system. Consequently, the growth-stage development of these enterprises and the government’s willingness to pay will be significantly affected.
To this end, the white paper also puts forward relevant recommendations for government regulators and industry stakeholders, respectively.
From the government’s perspective, first, when formulating policies, the government should prioritize coordination across departments (public health, healthcare, medical insurance, etc.) and among various policy instruments., incorporating the concept of value-based healthcare into top-level design, with a core focus on measuring population health outcomes and medical effectiveness, and leveraging key disease categories and populations (such as chronic diseases, cancer, and the elderly) as breakthrough points to drive the upgrading of service delivery systems and payment models.
Second, emphasis should be placed on establishing metrics for evaluating medical outcomes and a benchmarking research system.as well as the development of supporting infrastructure for medical informatics, to promote accurate measurement of healthcare value and guide investment directions in the healthcare system and strategic purchasing decisions by payers. It is hoped that health insurance authorities will participate in data collection on healthcare quality and the design of quality reporting, with multi-sector collaboration in this area.
Third, in the process of promoting the implementation and piloting of local policies, the central government provides greater guidance to local authorities and conducts more scientific and rigorous evidence-based evaluations.
In terms of industry, the primary objective is to create value for the healthcare service system and explore related business models.As patient-centered integrated healthcare systems are gradually established, healthcare institutions will shift from a profit-driven model to one where population health outcomes serve as the primary performance indicator.
Second, collaborate with medical insurance schemes to improve the access framework and innovate payment models. Third, integrate public and market-based systems to promote the development of commercial health insurance, thereby creating value for and providing a close supplement to basic medical insurance. Fourth, advance digital healthcare grounded in value-based evidence. Fifth, industry stakeholders should adopt a holistic view of the healthcare system, actively pursue external collaborations, and build effective platforms and leadership to guide multiple parties in forming a tightly integrated community of shared interests.
What Benefits Can Value-Based Healthcare Bring? Jin Chunlin, Director of the Shanghai Health Development Research Center, stated at the forum that value-based healthcare can improve medical service delivery and enhance patients’ personal experience, increase the efficiency of limited resource utilization, reduce costs, strengthen the integration and coordination between public hospitals and related service systems, and promote the healthy and sustainable development of the health system.
Value-based healthcare is gaining momentum in China, requiring concerted efforts from industry, academia, research institutions, and the government.