Sanming Medical Reform: Eight Key Steps Over Eight Years and the National Replication Model
On December 6, the National Health Commission held a press conference in Sanming, Fujian Province. Huang Ruxin, Party Secretary of the Fujian Provincial Health Commission, and Zhang Yuanming, Deputy Mayor of the Sanming Municipal People’s Government, respectively introduced the healthcare reform practices, progress, and outcomes in Fujian Province and Sanming City.
As early as November 15, the Leading Group for Deepening the Reform of the Medical and Healthcare System under the State Council issued the “Notice on Further Promoting the Experience of Fujian Province and Sanming City in Deepening the Reform of the Medical and Healthcare System,” arranging relevant work to promote the healthcare reform experiences of Fujian Province and Sanming City, and requiring that the focus of deepening healthcare reform be shifted more toward ensuring implementation and achieving tangible results.
Sanming City is a star of healthcare reform, which is no longer news. Sanming launched its healthcare reform in early 2012. After years of exploration, it has transformed from an obscure prefecture-level city into a national model. During this period, it made bold breakthroughs in pharmaceuticals, medical services, and health insurance, and its experience has significantly influenced the implementation of healthcare reform in Fujian Province. We cannot help but ask: What exactly did Sanming do? And how did it do it?
Sanming City is located in the mountainous region of central-western Fujian Province, covering an area of 22,900 square kilometers and administering 12 counties (county-level cities and districts). The city’s permanent resident population exceeds 2.5 million, which is more than 200,000 fewer than its registered household population, highlighting a significant trend of population outflow. As a former industrial hub, Sanming has a high proportion of retirees, with the issue of “getting old before getting rich” being particularly prominent. In 2011, the support ratio for urban employees in Sanming was 2.06:1, meaning that roughly two workers supported each retiree, and this indicator showed a declining trend, imposing substantial pressure on the system.
At the time, Sanming City also faced common problems prevalent in the healthcare industry. Due to gray areas in the pharmaceutical distribution sector, artificially inflated drug prices led to dual waste in both the price and volume of medications, accounting for 30%–50% of total pharmaceutical expenditures.
In 2000, the pharmaceutical revenue of 22 hospitals at or above the county level in Sanming City amounted to RMB 313 million. By 2005, this figure had risen to RMB 649 million, representing a 107.59% increase over five years. In 2010, it further climbed to RMB 1.433 billion, marking a 120.91% increase over the preceding five years. By 2011, pharmaceutical revenue reached RMB 1.69 billion, with expenditures on drugs and medical consumables accounting for as high as 61% of total revenue. The excessive growth rate and unreasonable structure of pharmaceutical revenue rendered the fiscal burden unsustainable, imposed an excessive financial burden on patients seeking medical care, and failed to reflect the professional value of healthcare workers.
In 2010, the pooled fund for employee basic medical insurance in Sanming City recorded a deficit of RMB 144 million; this widened to RMB 208 million in 2011, with local government finances unable to cover the shortfall. The convergence of fiscal constraints, a continuously declining support ratio (i.e., the ratio of contributors to beneficiaries), and persistent deficits in the medical insurance fund compelled Sanming City to undertake comprehensive healthcare system reforms.
At the outset of the Sanming healthcare reform, a series of goals, visions, and methodologies were proposed, including:
With the goal of achieving the “Four Feasibilities” (acceptable to the public, affordable for government finances, sustainable for the fund, and viable for hospitals);
Adhering to the requirements of the “Three Returns” (public hospitals returning to their public-welfare nature, doctors returning to their role as clinicians, and drugs returning to their therapeutic function);
Taking the “Three Reliances” (reliance on government for hardware investment in public medical institutions, reliance on hospitals themselves for software and daily management, and reliance on institutional and mechanistic innovation to reduce medical costs and improve operational efficiency) as the focal point;
Through the approaches of “three-medical linkage” (pharmaceuticals, medical services, and health insurance) and “four-level coordinated promotion” (municipal, county, township, and village-level medical institutions).
In summary, this approach follows the “emptying the cage to change the bird” strategy to create fiscal space and optimize structure. By eliminating unreasonable margins previously embedded in pharmaceuticals and medical consumables, it alleviates the burden on the basic medical insurance fund. This enables a win-win outcome for both patients and healthcare providers (hospitals and physicians), thereby fostering a virtuous cycle within the healthcare system.
How Much of Sanming’s Goal Has Been Achieved? On December 6, at a press conference held by the National Health Commission, Sanming City released a set of data: the average cost per hospitalization under the urban employee basic medical insurance scheme decreased from RMB 6,553 in 2011, before the reform, to RMB 5,847 in 2018; the average cost per hospitalization for urban and rural residents increased from RMB 4,082 to RMB 4,869, representing an average annual growth rate of only 2.55%. Compared with the pre-reform period, the average annual salary of hospital directors rose from RMB 112,000 to RMB 324,300 in 2018, while the average annual salary of medical staff increased from RMB 42,200 to RMB 113,400 in 2018. Despite a year-on-year decline in the support ratio (the number of contributors per beneficiary), the urban employee basic medical insurance fund turned from deficit to surplus and has maintained a positive balance for seven consecutive years.
VCBeat (WeChat ID: vcbeat) has also compiled historical data to more intuitively demonstrate the effectiveness of the Sanming healthcare reform.
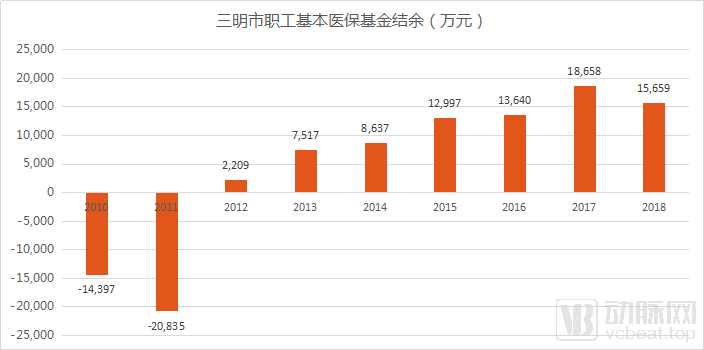
Surplus of the Basic Medical Insurance Fund for Employees in Sanming Before and After the Healthcare Reform; Data Source: Sanming Municipal Healthcare Security Administration
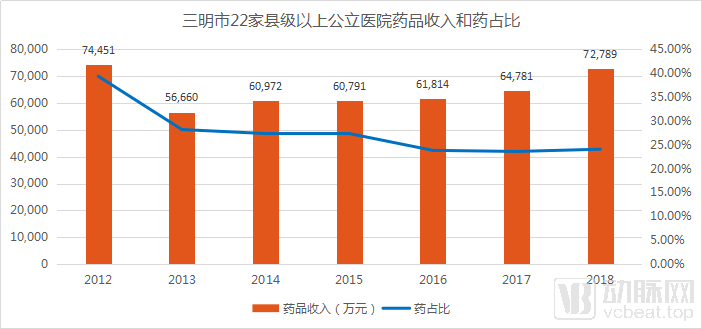
Changes in Drug Revenue and the Proportion of Drug Costs at 22 Public Hospitals Above the County Level in Sanming, Source: Sanming Municipal Health Commission
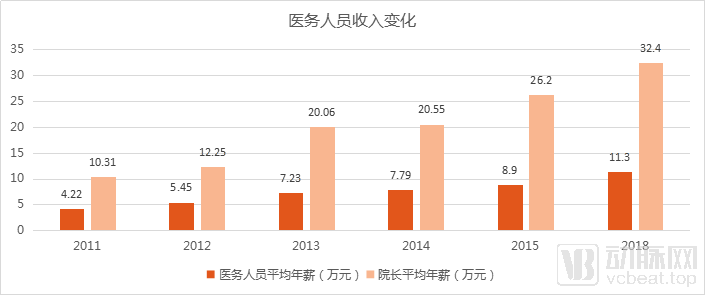
Changes in the Income of Medical Staff and Hospital Directors in Sanming City (Specific Data for 2016 and 2017 Are Not Yet Available in Public Sources)
Data source: Sanming Municipal Health Commission
Based on the above data, it is evident that during the “vacating the cage to change the bird” process of the Sanming healthcare reform, drug revenue was effectively reduced and stabilized, and the proportion of drug costs in total medical expenses was continuously lowered. The funds freed up through this adjustment, combined with the advancement of systemic reforms, have achieved consecutive surpluses in the medical insurance fund, increased income for medical personnel, and reduced out-of-pocket expenses for patients. The vision from those early years is gradually becoming a reality.
As 2019 draws to a close, the Sanming healthcare reform has effectively been underway for eight years since early 2012. What we hope to glean from Sanming is not merely the halo of being a benchmark, but rather the methodology employed throughout the process. Therefore, using each year as a chronological marker, we look back at the different issues addressed by Sanming City across various stages over the past eight years, in an attempt to identify effective approaches.
2012: Launch of Healthcare Reform and Breakthroughs in Management Systems
In early 2012, Sanming City officially launched its healthcare reform.
It is well known that for an enterprise to drive a business initiative, it must prioritize the effort from the top down, establish an organizational structure and management processes aligned with the initiative, and clearly define responsibilities. This is even more critical when government departments seek to advance reforms, particularly those targeting deep-rooted problems that have persisted for many years.
Therefore, the Sanming healthcare reform began with restructuring the management system. A Leading Group Office for Deepening Healthcare System Reform in Sanming was jointly established by multiple departments, including the Municipal Party Committee and Municipal Government, the Municipal Finance Bureau, the Municipal Health and Family Planning Commission, the Municipal Human Resources and Social Security Bureau, and the Municipal Food and Drug Administration. This office comprehensively coordinated reform efforts, centralized the management of functional departments involved in public hospital reform—covering pharmaceuticals, health insurance, and medical services—and established an efficient mechanism for decision-making and implementation, thereby laying the foundation for the coordinated development of medical care, health insurance, and pharmaceuticals (the “Three-Medical Linkage”).
At that time, the entrenched challenges in healthcare encompassed multiple interconnected aspects—including drug pricing, the proportion of pharmaceutical costs, medical staff compensation, and health insurance reimbursement—where a change in one area would have system-wide repercussions. The most fundamental issue lay within the pharmaceutical sector.
In April 2012, Sanming City implemented key monitoring measures targeting 129 specifications of so-called “miracle drugs”—including adjuvant and nutritional agents, high-kickback products, and those with “uncertain efficacy but definite prices.” As a result, pharmaceutical expenditures decreased by RMB 16.73 million in that month alone. Meanwhile, the city strictly controlled excessive prescribing, capped average outpatient and inpatient costs per visit, and imposed stringent restrictions on the use of antimicrobial agents.
But if drug monitoring is tightened, what will happen to hospital revenues? What about the incomes of medical staff? And how will hospitals continue to develop? Sanming City has implemented corresponding measures to address these issues.
For hospitals, the responsibility for operating medical institutions should be clearly defined, and a scientific fiscal investment mechanism should be established. The government shall be responsible for funding capital construction, equipment procurement, development of key disciplines, and public health services in public hospitals. All infrastructure projects undertaken by hospitals shall receive full fiscal funding.
For hospital directors, a target annual salary system is implemented, with their salaries fully covered by fiscal funds. This reflects the director’s role in representing the government to fulfill hospital management responsibilities and severs direct financial ties between the director and the hospital. A comprehensive evaluation system for hospital directors, comprising six major categories and 40 indicators, has been established. The Municipal Healthcare Reform Leading Group conducts thorough assessments of directors based on hospital service evaluation, operational direction, safe hospital construction, hospital management, and hospital development. Assessment results are linked to the director’s annual salary and the approved total wage bill of the hospital, thereby transforming individual accountability into shared institutional responsibility and motivating all medical staff to actively participate in hospital management.
Implement a target annual salary system for physicians, under which clinical practitioners, technicians, and clinical pharmacists receive tiered annual salaries based on their rank and position. The funds required for the annual salaries of medical technical staff shall be borne by the hospital, with the president having the autonomy to distribute these funds within the approved total wage bill. The performance-based annual salary assessment for medical technical staff is linked to job workload, medical ethics and conduct, and social evaluation.
Ensuring the motivation of hospitals and physicians through institutional reforms, and reducing drug costs via measures such as drug utilization monitoring and control of excessive prescribing—these were the primary explorations undertaken at the outset of the Sanming healthcare reform. These initiatives yielded results rapidly.
In 2012, the drug expenditure of public hospitals at or above the county level in Sanming City decreased by RMB 61.2 million. Calculated based on the average growth rate across Fujian Province, Sanming City saved RMB 243 million in drug costs. The financial burden of medical expenses on the government, medical insurance funds, and patients was alleviated, while the level of medical insurance coverage was further improved.
In 2013, pharmaceuticals served as the breakthrough point to achieve the “integration of three basic medical insurance schemes.”
After achieving success in the key monitoring of drug varieties, Sanming City implemented further reforms in drug-related sectors in 2013.
First, from the perspective of drug utilization. This year, Sanming City completely abolished drug markups and implemented zero-markup pricing for pharmaceuticals in hospitals at or above the county level, thereby dismantling the mechanism of subsidizing healthcare through drug sales, curbing artificially inflated drug prices, reducing medication waste, and promoting rational drug use. The resulting loss of markup revenue for hospitals was offset through measures such as adjusting service prices, providing government subsidies, and strengthening internal hospital management, all without increasing the financial burden on patients.
Next is the pharmaceutical distribution sector. In fact, as early as 2009, Fujian Province, as a pilot province for comprehensive healthcare reform, became the first in China to implement the “Two-Invoice System.” In June 2013, Sanming mandated strict enforcement of the “Two-Invoice System” for pharmaceuticals: under the model of “pharmaceutical manufacturer–distributor–medical institution,” one invoice is issued from the manufacturer to the distributor, and a second invoice is issued from the distributor to the medical institution, with goods accompanied by corresponding invoices to prevent counterfeit and substandard drugs from entering the supply chain.
Since October 2013, Sanming City has implemented procurement at the lowest possible prices while ensuring quality, strictly adhering to the “one drug, two specifications” rule (i.e., each drug product is limited to two specifications), and carrying out joint price-capped procurement for pharmaceuticals. By bundling the city’s total procurement volume to negotiate lower prices from manufacturers, this approach served as an early prototype of volume-based procurement. Sanming commissioned the Xiamen Haixi Pharmaceutical Trading Center to design and develop a new digital platform to implement joint price-capped procurement and settlement for both pharmaceuticals and medical devices. This platform enables regulatory authorities to conduct end-to-end oversight, thereby providing technical support to ensure the implementation of the “Three-Medical Linkage” reform.
In 2013, Sanming City established the Medical Security Fund Management Center, taking the lead in the province to achieve the “integration of three insurance schemes,” thereby reducing management costs and improving management efficiency.
Through further reforms in pharmaceutical distribution and utilization, the effectiveness of Sanming’s healthcare reform has become more pronounced; in 2013, the surplus of the pooled fund for urban employee basic medical insurance in the city reached RMB 75.17 million.
In 2014, high-level attention drew a flood of visitors seeking to learn from best practices.
2014 was a year of great significance for the Sanming healthcare reform. The achievements of its reform attracted the attention of high-level national authorities, with senior leaders and relevant ministries conducting successive inspections of the Sanming healthcare reform.
Healthcare reform involves numerous interconnected and complex components. For hospitals and physicians, the government safeguards their public-welfare nature and recognizes the value of their labor by reducing expenditures from medical insurance funds and increasing fiscal subsidies. In contrast, pharmaceutical distribution is highly market-driven. The government cannot provide long-term compensation for the “losses” incurred in this sector, especially since some of these “losses” are inherently unreasonable. Moreover, this issue involves multiple stakeholders—including pharmaceutical manufacturers, distributors, and medical representatives—resulting in broad and profound impacts.
Therefore, if the Sanming healthcare reform remained in a prolonged phase of self-directed exploration, it would face significant resistance, and its long-term trajectory would be uncertain. However, endorsement from top leadership and support from relevant ministries have greatly enhanced the certainty of the reform’s sustainability.
At this point, Sanming City has accumulated considerable experience in income distribution, compensation mechanisms, pharmaceutical distribution, tendering and procurement, and performance evaluation. However, nationwide promotion still requires continued exploration. This does not prevent cities across China from learning from Sanming’s practices.
According to data released by the Sanming Municipal Health Commission, in 2014, leaders at various levels and from different regions, as well as media representatives, conducted more than 300 visits to Sanming to investigate, inspect, and report on healthcare reform efforts. Meanwhile, Sanming dispatched over 20 teams specializing in healthcare reform to cities such as Chongqing and Tianjin to deliver special reports on their experience with healthcare reform.
Of course, the phased breakthroughs did not lead Sanming to rest on its laurels. In 2014, Sanming continued to roll out a series of measures aimed at reducing medical costs and optimizing the allocation of healthcare resources.
For example, in 2014, Sanming City identified 53 common and frequently occurring diseases that do not require intravenous infusion therapy, thereby further standardizing medication use. It took the lead in the province in implementing a tiered diagnosis and treatment system and a two-way referral system, guiding insured individuals to make rational choices of medical institutions for care. The city promoted the establishment of a division-of-labor and collaborative mechanism between urban hospitals and primary healthcare institutions to prevent overmedicalization, forming a care model characterized by initial consultation at the primary level, tiered diagnosis and treatment, separate management of acute and chronic conditions, and two-way referrals, thus enhancing the coordination, continuity, and integration of medical services.
2015: Healthcare Reform Enters an Upgraded Phase, Facing Three Major Challenges
In 2015, Sanming City issued the “Opinions of the CPC Sanming Municipal Committee and the Sanming Municipal People’s Government on Further Deepening the Reform of the Medical and Healthcare System.” The Sanming healthcare reform entered a phase of systemic upgrading, with breakthrough areas similar to those at the outset of the 2012 launch, focusing primarily on institutional frameworks, pharmaceuticals, hospitals, and medical personnel.
Systemic Breakthroughs primarily involve dismantling the restrictions on bianzhi (staffing quota) management in public hospitals, weakening bianzhi management for public hospitals at Level II and above, replacing the approval-based system for bianzhi utilization with a record-filing system, rationally determining staffing scales for public hospitals at all levels, and granting public hospitals autonomy in recruitment and hiring. In accordance with the requirements of the modern hospital management system, the administrative ranks of directors of public hospitals at Level II and above shall be de-emphasized, and a contract-based appointment system for hospital directors shall be implemented. Directors shall be appointed by the healthcare reform leading group at the corresponding level, with a term of five years per term and a maximum of two consecutive terms, thereby promoting the professionalization and specialization of public hospital leadership. Leaders of health administrative departments at all levels are strictly prohibited from concurrently serving as directors of public hospitals.
To sustain the motivation of healthcare professionals, Sanming City has structured its income distribution system around the principles of “more pay for more work,” “higher compensation for superior performance,” and “equal pay for equal work regardless of employment status (within or outside the established staffing quota).” Priority is given to frontline clinical staff, key positions, core professional personnel, and those who have made outstanding contributions. In principle, the distribution of the total wage bill is allocated as follows: 50% to physicians, 40% to nursing staff, and 10% to administrative and logistical management teams. Meanwhile, the implementation of the annual salary system has been extended to primary healthcare institutions.
Regarding pharmaceuticals, on the basis of continuing to implement price-capped procurement for drugs, Sanming City has implemented centralized tendering and procurement for all medical consumables (including diagnostic reagents) used clinically by healthcare institutions across the city. If a healthcare institution can procure medical consumables (diagnostic reagents) at a price more than 10% lower than the municipal procurement price for the same type of product, it is permitted to conduct independent procurement, and reimbursement will be provided at the same rate as that under the medical insurance scheme.
Furthermore, starting from April 1, 2015, Sanming City implemented a unified drug formulary, diagnosis and treatment catalog, and service standards for its Urban Employee Basic Medical Insurance, Urban Resident Basic Medical Insurance, and New Rural Cooperative Medical Scheme, achieving the “Three Unifications.” Concurrently, differentiated reimbursement policies were introduced to further favor primary healthcare institutions, thereby promoting tiered diagnosis and treatment.
These measures have not only saved funds from the medical insurance pool and increased the overall income of healthcare professionals, but also laid the foundation for subsequent centralized procurement of drugs and consumables, as well as reforms in medical insurance payment methods.
However, at this time, Sanming City still faces a series of issues. For example:
Low bargaining power for pharmaceuticals and medical consumables. Due to small procurement volumes, it is difficult to significantly reduce drug prices through negotiations, particularly for imported original-brand drugs and consumables, imported equipment, and domestically exclusive drugs.
The "three medical insurances" at the national level in China have not yet been unified, and local unification still encounters detailed issues in implementation.
Weak primary healthcare resources hinder the implementation of tiered diagnosis and treatment, thereby impeding the overall progress of healthcare reform.
2016: Further Breakthroughs in Institutional Innovation; Establishment of the Healthcare Security Administration to Consolidate Functions
In response to the aforementioned issues, Sanming City achieved two major breakthroughs in 2016: the joint drug procurement initiative of the “Sanming Alliance” and the establishment of the Sanming Healthcare Security Administration.
In March 2016, the Sanming Medical Security Fund Management Center pointed out in a notice that Sanming City had established a drug procurement alliance with cities such as Ningbo, Wuhai, Yuxi, and Zhuhai, and other cities would join successively. By October 2016, when the procurement was launched, the alliance included not only the aforementioned cities but also six healthcare reform pilot cities in Hebei Province—Tangshan, Handan, Cangzhou, Hengshui, Xingtai, and Zhangjiakou—as well as 28 demonstration counties, along with participants such as Taiyuan and Ordos.
When procurement volume in a single location is too small, multiple locations can join forces. The original intention of the “Sanming Alliance” was to leverage volume-based bargaining to secure lower drug prices and higher supply rates. At this point, alliance members have stronger negotiating power, requiring pharmaceutical companies to have the capacity to supply products at the same price to all cities within the alliance simultaneously. Previously, if a pharmaceutical company abandoned the Sanming market due to Sanming’s healthcare reforms, it might have been feasible. However, with the formation of the alliance, such an approach warrants careful reconsideration.
The “Sanming Alliance”’s exploration of cross-regional joint procurement also accumulated experience for the subsequent national-level promotion of the “4+7” centralized drug procurement.
To address the issue of unified management of the “three medical insurances,” Sanming City achieved a more significant systemic breakthrough in 2016 by establishing the Medical Security Administration Bureau, the first of its kind in China. The Sanming Medical Security Bureau consolidated responsibilities previously dispersed across the Human Resources and Social Security Department, the Health and Family Planning Commission, the Finance Department, and the Medical Insurance Management Center. It also integrated drug procurement functions into the Medical Insurance Management Center, thereby completely severing financial transactions and interest chains between hospitals and pharmaceutical suppliers.
In 2016, Fujian Province also established the Provincial Healthcare Security Administration Committee and set up its office, integrating all healthcare security management functions previously dispersed across multiple departments, including Health and Family Planning, Civil Affairs, Finance, and Social Security. This change not only served as one of Fujian Province’s supportive measures for the Sanming healthcare reform, enabling better coordination between provincial and municipal institutional structures and functions, but also facilitated the promotion of the Sanming healthcare reform experience at the provincial level.
In 2018, the National Healthcare Security Administration (NHSA) selected Sanming City for its inaugural field survey shortly after its establishment, underscoring Sanming’s pivotal role as a “strategic purchaser” of healthcare insurance funds. By integrating urban and rural medical insurance systems, reforming drug procurement and bidding mechanisms, and improving payment methods, Sanming effectively promoted the coordinated development of healthcare services, health insurance, and pharmaceuticals—known as the “Three-Medical Linkage”—thereby accumulating valuable experience for the advancement of national healthcare insurance initiatives.
2017: Building Close-Knit Medical Consortia and Breaking Through Health Insurance Payment Reform
After years of systemic breakthroughs, the Sanming healthcare reform has achieved horizontal integration among medical care, health insurance, and pharmaceuticals. Entering 2017, the coordinated development of these three sectors shifted its focus to in-depth advancement.
In 2017, Sanming City leveraged the establishment of general hospitals as a vehicle to comprehensively build close-knit medical consortia and promote the decentralization of high-quality medical resources to the grassroots level. By the end of 2017, the city had established 10 county-level general hospitals and two close-knit medical consortia in urban districts, initially establishing a tiered diagnosis and treatment system characterized by initial consultations at the primary care level, two-way referrals, separate management of acute and chronic conditions, and coordinated care between upper- and lower-level institutions.
On the one hand, medical consortiums can facilitate the downward flow of high-quality medical resources. Within each consortium, tertiary medical institutions should leverage their professional and technical expertise to enhance the service capabilities of primary and secondary care facilities by dispatching medical personnel to conduct outpatient services, clinical mentoring, teaching rounds, and operational guidance.
On the other hand, the development of medical consortia can lay the foundation for reforms in health insurance payment systems. Taking Youxi County in Sanming City as an example, Youxi County Hospital and Youxi County Traditional Chinese Medicine (TCM) Hospital integrated their resources to establish the Youxi County General Hospital. Following the integration, both the County Hospital and the County TCM Hospital were incorporated as whole entities into the General Hospital, becoming its medical branches, while township health centers were designated as subsidiary branches.
Prior to integration, medical institutions within the county competed for a share of the health insurance fund “cake.” After integration, payments from the health insurance fund were directed to the Medical Consortium (i.e., the General Hospital), requiring all member institutions to align their objectives and collaborate through coordinated division of labor.
After five years of reform, the Sanming healthcare reform has yielded advantages in multiple areas, including government administration, hospital systems, and drug pricing. Building on this foundation, further exploration of payment models is required to reduce medical costs, enhance medical quality and safety, curb unreasonable growth in pharmaceutical and medical expenses, and improve the efficiency of health insurance fund utilization.
2018: Implementation of C-DRG Payment Reform to Reduce Medical Costs
Implementing inpatient fee payment based on Clinical Diagnosis-Related Groups (hereinafter referred to as C-DRG) in public hospitals at the county level and above is a key measure for Sanming to deepen healthcare reform. The C-DRG payment system was implemented starting January 1, 2018. Meanwhile, Sanming City is one of the three pilot cities selected by the National Health Commission for C-DRG reform.
In accordance with the documents issued by the Sanming Municipal Healthcare Security Administration and the Health Commission, C-DRG is divided into 788 groups based on factors such as the severity of the disease, the complexity of treatment methods, and the actual level of resource consumption, with pricing and payment implemented on a group basis. C-DRG payment and charging adhere to the principle of “same disease, same treatment, same price” within hospitals of the same tier, establishing payment standards across two levels: secondary hospitals and tertiary hospitals.
For insured patients whose medical expenses incurred at public hospitals at the county level or above are settled according to the C-DRG grouping fee standards, no deductible shall apply. Costs shall be shared between the individual and the pooled fund in specified proportions. For urban employee basic medical insurance, individuals bear 30% and the pooled fund covers 70% at both secondary and tertiary hospitals. For urban and rural resident basic medical insurance, individuals bear 30% and the pooled fund covers 70% at secondary hospitals, while at tertiary hospitals, both the individual and the pooled fund bear 50% each.
Medical expenses incurred by insured patients during hospitalization at designated primary healthcare institutions (community health service centers and township health centers) shall be settled based on the actual total medical costs of hospitalization, with no deductible applied. Costs shall be shared proportionally between the individual and the pooled fund, with the individual bearing 20% and the pooled fund covering 80%.
Prior to this, Sanming City had already explored various composite payment methods, such as per-visit average cost and diagnosis-related group (DRG) payments, gradually expanded the number of diseases covered under single-disease payment reforms, and promoted refined management of medical insurance. C-DRG represents a further attempt at reforming the payment and charging model.
In 2018, after excluding special cases, 62.88% of discharged patients from hospitals at or above the secondary level in Sanming City were settled under the C-DRG payment system, resulting in a relative savings of RMB 12.8352 million in medical expenses.
2019: Advancing C-DRG and Linking It to Compensation Assessment
Deepening the reform of health insurance payment methods and accelerating the pilot implementation of Diagnosis-Related Groups (DRG)-based payment have been key initiatives vigorously promoted by China’s national healthcare system in recent years. After achieving initial success in the first year of its C-DRG payment and charging reform pilot, Sanming City further refined the program in 2019.
In 2019, for insured patients hospitalized in hospitals within the pooling area, if the actual medical expenses incurred were lower than the C-DRG group-based payment standard, the patient’s out-of-pocket payment was calculated based on the actual expenses, and the difference from the group-based payment standard was covered by the pooling fund; if the actual medical expenses incurred were no more than three times the C-DRG group-based payment standard, settlement was made according to the group-based payment standard.
For example, a patient covered by the Urban and Rural Resident Basic Medical Insurance was hospitalized at a county-level general hospital, with a C-DRG bundled payment standard of 5,000 yuan. Under the previous policy, if the patient’s actual medical expenses amounted to 4,600 yuan, the individual would be responsible for 1,500 yuan in treatment costs. Following the implementation of the new policy this year, the patient is only required to cover 30% of the actual medical expenses, i.e., 1,380 yuan, thereby reducing the out-of-pocket burden by 120 yuan. The difference is reimbursed by the medical insurance fund.
To strengthen the implementation of the C-DRG payment and charging reform, Sanming City further deepened the compensation system reform in public hospitals in 2019. The total amount of wages distributable by a hospital in the current year is determined annually based on the results of the annual performance assessment. This total wage bill consists of four components: the hospital’s total annual wages, performance-based incentive funds for C-DRG assessments, performance-based incentive funds for integrated chronic disease management, and income from family doctor contract services. The surplus generated from the China Diagnosis-Related Groups (C-DRG) payment and charging reform projects is incorporated into the hospital’s medical service revenue.
As a result, the enthusiasm of medical staff to improve healthcare efficiency and reduce medical costs under the C-DRG model has been further stimulated.
A review of the eight nodes reveals that the Sanming healthcare reform actually follows this trajectory:
First, implement reforms to the government and hospital management systems;
Second, pharmaceutical reforms were primarily driven by joint procurement, enhanced medication monitoring, and the elimination of drug markups.
Third, advance health insurance reform by integrating the three basic medical insurance schemes and continuously improving payment methods.
Fourth, healthcare reform should be driven primarily by the continuous improvement of compensation systems and the adjustment of medical service prices.
These steps follow a sequential order while undergoing continuous iterative optimization; they are interconnected and advance in synchrony, thereby giving rise to the data trends presented at the beginning of this article.
Since the launch of healthcare reform in Sanming City, more than 120 policy documents on healthcare reform have been formulated and implemented. During the implementation process, Fujian Province has not only provided support and impetus but also replicated and promoted the “Sanming experience” at the provincial level.
For example, Fujian Province has established an integrated platform for the procurement, distribution, payment, and supervision of pharmaceuticals and medical consumables across the province. Building on the pilot program for centralized drug procurement and use initially launched in Xiamen City, the entire province implemented this initiative in June this year. By enabling province-wide sharing of transparent pricing information for medical devices and high-value medical consumables through the platform’s “price disclosure” mechanism, average prices have been reduced by 22.6%.
Fujian took the lead nationwide in completing reforms to its medical insurance management system, exploring the establishment of a provincial-level pooling mechanism for the basic medical insurance fund for urban employees on the basis of municipal-level pooling. In 2019, a provincial adjustment fund was raised at 30% of the actual contributions collected in each locality that year. A total of RMB 7.513 billion was raised in the first three quarters, with RMB 7.206 billion allocated to various pooling areas. Six pooling areas benefited from this initiative, receiving a total of RMB 604 million.
In terms of reforming medical insurance payment methods, the number of diseases covered by case-based charging and payment across the province has reached over 700, while Nanping City and three other provincial- and municipal-level hospitals are steadily advancing the pilot program for Diagnosis-Related Group (DRG) charging and payment.
Furthermore, Fujian Province selected 44 hospitals to pilot the provincial modern hospital management system, introducing a “package” of measures including target annual salary systems for hospital directors, total wage bill verification, and hospital performance assessments. This has achieved full coverage of compensation system reforms in public hospitals, with the average annual growth rate of medical staff’s wage income reaching 12.3% in recent years.
Sanming’s healthcare reform initiatives—including the tripartite coordination of medical services, health insurance, and pharmaceuticals; the two-invoice system; annual salary systems; integration of the three basic medical insurance schemes; and the establishment of healthcare security administrations—have been elevated to national top-level design.
On November 15 this year, the Leading Group for Deepening the Reform of the Medical and Healthcare System under the State Council issued the “Notice on Further Promoting the Experience of Fujian Province and Sanming City in Deepening the Reform of the Medical and Healthcare System.” The notice requires all provinces to formulate work plans for promoting the healthcare reform experiences of Fujian Province and Sanming City and furthering healthcare reforms, based on their actual conditions. These plans must specify concrete tasks for local prefecture-level cities and relevant departments within each region and ensure their implementation.
An overview of the current stage of deepening healthcare reform reveals that, compared to the environment at the outset of the Sanming healthcare reform, a solid foundation has now been established. Health commissions, healthcare security administrations, and drug administration authorities at all levels have clearly defined powers and responsibilities. The centralized volume-based procurement of pharmaceuticals has been expanded nationwide, with an increased variety of procured items, further enhancing the government’s bargaining power.
The design of top-level systems, as well as the direction and trends of reform, are no longer in question; the focus for various regions lies in having the willingness and determination to achieve breakthroughs, formulating appropriate measures based on local conditions, and ensuring their effective implementation.
“Nothing is impossible to a willing heart.”
Data in this article are sourced from the official websites of the Sanming Municipal Healthcare Security Administration, the Sanming Municipal Health Commission, the Sanming Municipal People's Government, and the National Health Commission.