Chen Haixiao, Director of Enze Medical Center: DRG as the Path to Balance Cost, Efficiency, and Quality
Orthopedic surgeon Chen Haixiao assumed the position of President of Taizhou Hospital in Zhejiang Province at the end of 2001. He not only transformed Enze Medical Group into a value-driven community that “regards quality as life,” but also facilitated the adoption of the clinical pathway management system developed by Taizhou Hospital in more than 130 hospitals across China, delivering an outstanding “report card” for Taizhou Hospital.
Taizhou Hospital of Zhejiang Province is located in Taizhou, a city known as the “land of fish and rice.” It is affiliated with the Taizhou Enze Medical Center (Group) and shares common origins with Luqiao Hospital, Enze Maternity Hospital, and Enze Hospital. As the top executive of Taizhou Hospital, Chen Haixiao plays a pivotal role in strategic decision-making. In 2016, the General Office of the Zhejiang Provincial Health and Family Planning Commission issued the Notice on Applying Diagnosis-Related Groups (DRGs) to Evaluate Hospital Medical Service Quality and Performance, marking an initial trial of DRGs. Recognizing the potential of DRGs in hospital management, Chen Haixiao promptly introduced this management tool.
Over the past three years, Taizhou Hospital’s DRG payment reform has begun to yield tangible results: a DRG-based clinical performance evaluation system has been established; the hospital’s Case Mix Index (CMI) reached 0.9992, ranking second in Zhejiang Province, while its Relative Weight (RW) for complex cases ranked sixth province-wide. Both healthcare quality and performance indicators are among the top in the province.
However, at the same time, potential issues inherent in DRG itself have begun to emerge: upcoding, refusal to treat severely ill patients, overtreatment of minor conditions, increased out-of-pocket expenses, and readmissions due to excessively short hospital stays.
At the “4th National Diagnosis-Related Groups (DRG) Forum,” Director Chen Haixiao delivered a keynote address titled “DRG and Value-Based Healthcare: Balancing Cost, Efficiency, and Quality.” Speaking from the perspective of hospital decision-makers, he shared his in-depth insights into hospital operations management and discussed the challenges encountered during DRG implementation along with their corresponding solutions.

Chen Haixiao, Director of Enze Medical Center (Image source: Forum Organizer)
DRG is currently the focal point of discussions in the healthcare industry, with its implications and impact thoroughly analyzed by sector experts. Essentially, DRG is a case-mix classification scheme and serves as a critical tool for evaluating the quality and efficiency of medical services, as well as for determining health insurance reimbursements.
On October 16, 2019, the National Healthcare Security Administration issued the "Notice on Printing and Distributing the Technical Specifications and Grouping Scheme for the National Pilot Program of Diagnosis-Related Groups (DRG) Payment" (Yi Bao Ban Fa [2019] No. 36), officially sounding the clarion call for DRG payment system reform in China. Striding forward with determination, China is working toward the goal of "simulated operation in 2020 and actual implementation in 2021."
DRG grouping logic is classified into four levels: the first level categorizes diagnoses by clinical system and anatomical site; the second level classifies treatment modalities into surgical or medical categories; the third level defines basic groups, known as Core Diagnosis-Related Groups (A-DRG), based on disease severity and the complexity of treatment; the fourth level further subdivides these into specific DRGs according to factors such as patient age and discharge status.
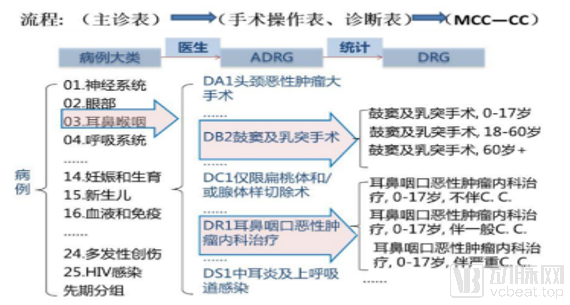
Example of DRG Grouping Logic (Image from Interviewee)
The goal of implementing DRG is to ensure the rational and effective utilization of medical resources.
By establishing unified disease diagnosis classifications and fixed payment standards, and implementing global budget management and control for hospitals, hospitals must reduce costs to achieve profitability. This helps incentivize hospitals to strengthen medical management, reduce induced medical expenses, and thereby ensure the standardized and rational use of medical resources.
Globally, low-value medical services that offer little to no benefit to patient treatment and recovery, or even have varying degrees of negative impact on patients, as well as medical services delivered in unsafe or inefficient ways, remain prevalent. This indicates that while reducing low-value care is a challenging and gradual endeavor, it constitutes the right approach to healthcare.
Hospitals must pursue innovation and improve health quality and outcomes while reducing costs.
At the 2016 World Economic Forum, the Chinese government, in collaboration with the World Bank and the WTO, released Deepening China’s Healthcare System Reform: Building a Value-Based High-Quality Service Delivery System, marking the “birth” of value-based healthcare in China.
Value-based healthcare requires hospitals to break away from traditional service models and adopt a “patient-centered” approach. While providing medical treatment, hospitals must comprehensively consider patients’ medical costs, treatment outcomes, and needs to deliver high-value services. However, this is not something hospitals can achieve alone; China’s current realities dictate that health insurance is also a key stakeholder.
Rising healthcare costs, driven by increasing demand for services and technological advancements, have created a conflict with the limited availability of medical and health insurance resources.
Physicians believe that value lies in being evidence-based and therapeutically effective. From the patient’s perspective, value is defined by achieving a cure while minimizing costs. In health economics, value is measured as health outcomes per unit of cost. Meanwhile, calculating costs and evaluating health outcomes are not straightforward tasks and require a lengthy process.
Based on this, in 2007, the Institute for Healthcare Improvement (IHI) proposed the Triple Aim to optimize healthcare system performance: improving the patient care experience, improving the health of populations, and reducing per capita healthcare costs. American scholars have suggested defining value-based healthcare using three dimensions: quality, cost, and patient experience.

The Relationship Between Value-Based Healthcare and Quality, Experience, and Cost (Image from the Interviewee)
In 2016, when the concept of value-based healthcare was proposed across the Pacific Ocean, Zhejiang Province initiated the construction of a DRG performance platform and began collecting detailed grouping data for each case. Taizhou Enze Medical Center Group, to which Taizhou hospitals belong, also joined hands with Hangzhou Huoshu Technology to commence DRG development.
Huoshu Technology, a medical big data enterprise under the Sky Group, specializes in DRG-based health insurance management. It pioneered China’s first hospital-side data platform for health insurance cost control. With a team of nearly 100 professionals in big data and healthcare, the company has established deep collaborations with over 100 tertiary hospitals across China and serves as a strategic technology partner for Alibaba Health’s “City Brain” initiative.
In this development process, Huoshu Technology has been progressing step by step, adhering to the strategy of “laying the foundation, identifying issues, and building systems.”
Under the DRG payment reform, hospitals must transition from a revenue-generation model to a cost-control model, while physicians face the imperative to enhance quality and efficiency in their clinical practices within the framework of regional benchmarks. Consequently, hospitals need to establish a closed-loop data management system to pinpoint issues. Huoshu Technology engages in the pre-, mid-, and post-settlement phases, implementing process control, appeal management, and data analysis to identify the root causes of problems.
For hospitals, it is crucial to balance the relationship between medical quality and cost control under the DRG payment system, and to identify high-quality and effective medical solutions. Taizhou Hospital has established and controlled the basis for DRG payments by grouping cases according to DRGs, integrating clinical pathways, conducting comparative analyses against actual hospital costs, and referencing the social average cost per disease type.
In 2019, Taizhou Enze Medical Center Group was honored with the National Quality Award in China’s healthcare sector for its high-quality lean management. This initiative helped balance the reimbursement amounts from medical insurance with the hospital’s actual medical costs, resulting in a 7% decrease in the proportion of pharmaceutical expenditures, a reduction of 0.7 days in the average length of stay, and a gradual decline in the proportion of cases with extremely high or low cost weights.
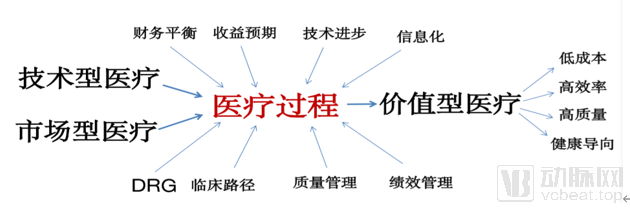
Pathways to Achieving Value-Based Healthcare (Image from the interviewee)
As a key instrument in healthcare insurance payment reform, what does the comprehensive rollout of Diagnosis-Related Groups (DRGs) truly mean for hospitals? How will it impact hospital performance management, and how will it influence clinical practices? Drawing on the implementation experience at Taizhou Hospital, Chen Haixiao shares insights into the impact of DRG implementation on medical practices and the healthcare market from five perspectives.
Following the implementation of DRG-based payment in hospitals, over-treatment practices are curbed, and the growth rate of inpatient treatment costs is controlled and reduced, allowing large hospitals to accelerate patient turnover. The average cost per hospitalization exhibits a pattern of initially rising before declining. As large hospitals admit a higher proportion of critically ill patients than smaller ones, policy permits them to receive certain payment adjustments; consequently, payment points rose significantly during the initial implementation phase before stabilizing.
However, for general hospitals that are limited to performing only simple surgeries (or those with a high volume of inpatient cases not requiring surgical intervention), the lower reimbursement points and the continued decline in average length of stay have resulted in more pronounced financial pressure.
It is important to note that while inpatients benefit from DRG-based payment, outpatient expenses for outpatients may increase. Due to the bundled payment for individual cases, it has become standard practice to shift non-surgical services out of inpatient care, leading to a trend where medical costs are transferred to pre-admission tests and post-discharge outpatient visits. However, if payers strengthen oversight of inpatient care and expand collaboration with primary care clinics, they can still ensure their overall revenue stability.
Bundled payment for disease categories has led to a reduction in hospital length of stay, but also decreased hospital revenues. To break even or increase income, some hospitals have responded by increasing the number of disease-related groups and expanding their service capacity. When encountering complex cases that exceed their technical capabilities, hospitals may transfer patients to other facilities to protect their revenue streams. Regulatory authorities can address this issue by monitoring inappropriate hospitalizations and fragmented admissions. This situation also serves as a wake-up call for healthcare institutions: for difficult and complex cases, a case-by-case analysis remains essential.
Notably, DRG-based payment facilitates the monitoring of hospitals’ medical practices, clinical outcomes, and financial revenues and expenditures by patients, society, and health insurance programs, thereby enabling the assessment of healthcare service efficiency, quality, and patient satisfaction.
The primary intent of Diagnosis-Related Groups (DRGs) is to control healthcare insurance costs. Although DRGs offer unique advantages in ensuring medical quality and safety, optimizing hospital operations, and enhancing performance management, they inherently possess certain limitations. For instance, DRGs are not applicable to outpatient cases, rehabilitation cases, cases requiring prolonged hospitalization, or cases where the diagnosis and treatment modalities are identical but there are significant disparities in resource consumption and treatment outcomes.
Moreover, as an imported concept, DRG faces numerous issues in derivative applications beyond health insurance payment, and significant challenges remain in adapting it to the local context in China.
DRG-based payment has been implemented in more than 40 countries worldwide. Experience has demonstrated that DRG is not only a health insurance payment mechanism and a tool for performance and quality management, but also an innovative approach to promoting the optimized allocation of healthcare resources. However, like two sides of a coin, it has both advantages and disadvantages. Chen Haixiao believes that hospitals should adopt “DRG-style hospital management thinking” to understand the transformation and continuously improve their management capabilities.