Clarifying Six Key Issues in DRG Implementation: Insights from Deng Xiaohong, Director of the DRG Quality Control Center, NHC
Since the second half of 2019, Diagnosis-Related Groups (DRG) has become one of the most frequently discussed buzzwords in the healthcare industry. As an imported concept, it has raised numerous questions among government agencies, enterprises, hospitals, insurance providers, and even patients. To address these concerns, Deng Xiaohong, a counselor to the State Council and Director of the DRG Quality Control Center under the Medical Administration and Hospital Management Bureau of the National Health Commission, provided explanations and answered key questions regarding the DRG system and its applications at the recently held 4th National Diagnosis-Related Groups (DRG) Forum. A reporter from VCBeat (WeChat ID: VCbeat) attended the session and has summarized her insights.
The State Vigorously Promotes Pilot Work on DRG Payment Reform
First, it is essential to clarify the definition of DRG. DRG is the abbreviation for Diagnosis Related Groups, which translates to "Diagnosis-Related Groups" in Chinese.
The prospective payment system based on such a grouping scheme is known as DRG-PPS. PPS is the acronym for Prospective Payment System. DRG-PPS refers to the implementation of prospective payment for each Diagnosis-Related Group (DRG) by assigning a specific reimbursement rate corresponding to its relative weight.
Carry out foundational work related to DRG
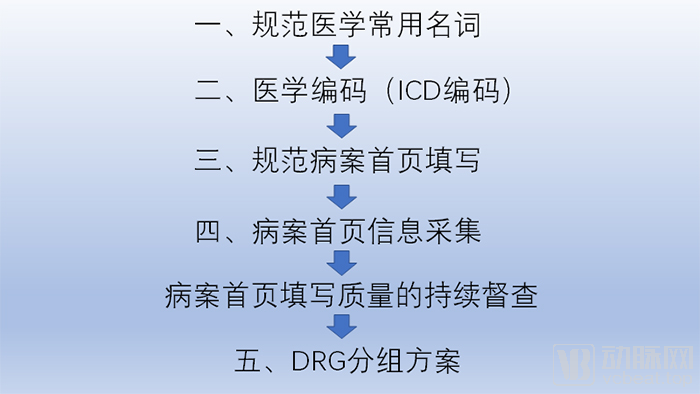
The basis for DRG grouping is the medical record front sheet, which must first be completed using standardized medical terminology.
Subsequently, ICD codes are standardized, with coding established on a one-term-one-code basis.
Standardizing the completion of the medical record face sheet is also fundamental to the implementation of Diagnosis-Related Groups (DRGs). Taking the average length of stay as an example, it is necessary to standardize the documentation criteria for admission and discharge dates; otherwise, inconsistencies in recording practices across hospitals will arise.
Meanwhile, continuous monitoring of the quality of medical record front page completion is required. Physicians who previously neglected the completion of the front page must place greater emphasis on standardized documentation, ensuring that no fields are omitted or incorrectly filled.
According to the current configuration, the completion rate of information on the homepage must reach 90%. Only by meeting this standard can patients be assigned to diagnosis-related groups (DRGs), and only then will the Healthcare Security Administration provide reimbursement.
Why Introduce DRG-Based Payment?
In recent years, medical service prices in China have risen significantly, outpacing both GDP growth and the increase in average social wages. If left unchecked, this trend could lead to a deficit in medical insurance funds. This would have a major impact on hospitals, for which nearly half of total revenue comes from medical insurance, and would also impose a heavy burden on patients.
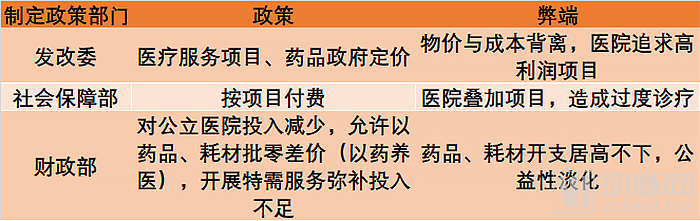
Therefore, it is essential to effectively control the unreasonable growth in medical expenses. One of the reasons for this irrational increase stems from unreasonable government pricing that severely deviates from actual costs, leading hospitals to pursue high-profit items to compensate for insufficient revenue from low-profit services.
Counselor Deng Xiaohong cited an example in which statistical data from a district/county hospital in Beijing showed that the number of patients with cerebral infarction increased by several hundred in that year. This anomaly drew the attention of relevant authorities, who subsequently launched an investigation.
At that time, the county hospital had acquired MRI equipment and mandated cranial MRI scans for all inpatients aged 55 and above upon admission, regardless of their underlying conditions. Given that many elderly patients exhibited lacunar cerebral infarction lesions on imaging, the hospital routinely added this diagnosis to their records. In reality, these patients were not hospitalized for this condition, nor did they receive any corresponding treatment during their stay.
Meanwhile, certain treatment modalities, such as acupuncture in traditional Chinese medicine (TCM), are gradually being abandoned by TCM hospitals due to their low prices, which are severely misaligned with costs. This has led to the gradual erosion of the traditional characteristics of TCM.
Long-term practice has demonstrated that government pricing of medical services has its limitations, and prices should be determined by market supply and demand.
Payment policies under the Ministry of Social Security’s medical insurance program also require corresponding adjustments. Historically, medical insurance reimbursement has been predominantly based on fee-for-service models, which has served as a significant policy driver encouraging hospitals to engage in excessive diagnostic and therapeutic procedures through the stacking of billable items.
Under a fee-for-service model, there are no specific caps on expenditures for even simple cases of the common cold; as long as the payment criteria are met, medications and diagnostic tests included in the reimbursement catalog are eligible for coverage. Consequently, treating a cold can incur costs exceeding one thousand yuan. In reality, as a self-limiting condition, most cases of the common cold resolve spontaneously within a week with adequate hydration and bed rest.
The third contributing factor is the reduction in fiscal subsidies to public hospitals by the Ministry of Finance, coupled with policies permitting hospitals to offset funding shortfalls through drug markups and the provision of special-needs medical services. This has significantly influenced hospital operational strategies. Hospitals are compelled to increase prescription volumes to boost revenue, while the expansion of special-needs services has diluted the public-welfare orientation of public hospitals.
These factors combined have led to a rapid increase in unreasonable medical costs at hospitals over the past few years. To address this issue, relevant authorities have implemented various policies aimed at finding solutions.
First, establish clinical pathways, implement project-based cost accounting, and apply for government adjustments to medical service pricing.
Under a fee-for-service payment model, hospitals cannot fully adhere to the principles of scientific rationality and cost-effectiveness when developing clinical pathways, often resulting in the addition of numerous testing and medication requirements. Furthermore, comprehensive government adjustments to medical service pricing are unlikely. Consequently, clinical pathways have not proven effective.
The emergence of clinical pathways is associated with the DRG payment model. Countries such as the United States implemented DRG-based payment first, after which hospitals developed clinical pathways to ensure medical quality and control healthcare costs. This stands in contrast to China, where clinical pathways were introduced prior to the adoption of DRG payment. Counselor Deng Xiaohong also noted that following the implementation of DRG payment, many clinical pathways formulated by hospitals in recent years may require adjustment.
The second approach is the global budget policy introduced by the medical insurance authorities. This policy sets a global budget for each hospital based on its total expenditures in the previous year. Hospitals exceeding the budget face penalties, while those with surplus funds receive rewards.
However, the implementation of this policy has yielded unsatisfactory results. First, there is significant variation in the number of patients and disease types treated by each hospital annually. Using the previous year’s expenditures to set targets for the following year incentivizes hospitals to avoid admitting complex and difficult cases to prevent budget overruns and ensure a surplus. Furthermore, taking Beijing as an example, a substantial proportion of patients at most major hospitals are from other regions. The local healthcare security administration’s policies apply only to Beijing-insured individuals and cannot regulate out-of-town patients. Consequently, Beijing hospitals may shift their focus to treating non-local patients as early as September when their insurance quotas are nearly exhausted, making it increasingly difficult for local residents to access inpatient care.
Relevant authorities also implemented a zero-markup policy for drugs and consumables, while simultaneously raising the pricing of medical services. However, new countermeasures quickly emerged. Diagnoses and treatments that could previously be completed with a single registration were split by hospitals into multiple visits across different departments, each requiring a separate registration fee ranging from tens to hundreds of yuan. The rise in medical costs has not been curbed.
Meanwhile, due to the increase in fees for specialist outpatient services, specialists who should be focusing on diagnosing and treating complex cases, teaching and training, and conducting scientific research have flocked to outpatient clinics. In fact, the vast majority of patients visiting general outpatient clinics do not require specialist care for diagnosis and treatment. This has led to a decline in the efficiency of medical services.
Following the failure of these policies, the National Healthcare Security Administration proposed DRG-based payment. Counselor Deng Xiaohong believes that, given the current realities, this may be an effective measure.
2019 Will Be a Pivotal Year for DRG Implementation
Although DRG, an imported concept from abroad, has long been introduced to China, its nationwide practical implementation has only begun in recent years, with remarkably rapid development. Particularly since late 2018, the policy-driven orientation has become increasingly evident.
On December 20, 2018, the National Healthcare Security Administration issued the “Notice on Declaring National Pilot Programs for Diagnosis-Related Group (DRG) Payment,” launching the application process for the national DRG payment pilot programs.
In May 2019, the National Healthcare Security Administration, the Ministry of Finance, the National Health Commission, and the National Administration of Traditional Chinese Medicine jointly issued the “Notice of the National Healthcare Security Administration, the Ministry of Finance, the National Health Commission, and the National Administration of Traditional Chinese Medicine on Printing and Distributing the List of National Pilot Cities for Diagnosis-Related Groups (DRG) Payment” (No. 34 [2019] of the National Healthcare Security Administration).
Among other things, the Notice proposed a three-step approach of “top-level design, simulation testing, and actual payment” to ensure the completion of tasks at each stage, with simulated operations in 2020 and the launch of actual payments in 2021. Prior to the initiation of payment reforms, the newly established National Healthcare Security Administration began consolidating the numerous DRG versions currently used across China, so that DRG-based payments could be implemented once a unified national version was established.
Meanwhile, in 2019, the General Office of the State Council and the General Office of the National Health Commission successively issued the Opinions on Strengthening Performance Appraisal of Tertiary Public Hospitals (Guo Ban Fa [2019] No. 4) and the Notice on Issuing the Operational Manual for National Performance Appraisal of Tertiary Public Hospitals (2019 Edition), employing DRG indicators (CN-DRG) to conduct quality performance evaluations of public hospitals across China.
At this point, the relevant national authorities have completed the preliminary policy groundwork for Diagnosis-Related Groups (DRG), approaching it from the two dimensions of performance evaluation and health insurance payment.
Six Major Questions About DRG Application
So, what problems have hospitals encountered in the application of DRG? Counselor Deng Xiaohong has summarized the issues faced by hospitals in her work, identifying the following six problems.

Deng Xiaohong, Counselor of the State Council and Director of the DRG Quality Control Center under the Bureau of Medical Administration and Hospital Management of the National Health Commission
First, physicians are unclear about how inpatient medical records are grouped under the DRG system.
Secondly, how are DRGs used for hospital performance evaluation?
Third, how are DRGs used for health insurance payment?
Fourth, what is the relationship between the “Four Unifications” emphasized by the National Health Commission in previous years and the DRG grouping scheme?
Fifth, what are the differences between the nomenclature codes used in CN-DRG and those in other versions?
Finally, how should pilot hospitals for DRG-based payment actively respond?
How Inpatient Medical Records Are Grouped into DRGs
DRG differs significantly from the previous single-disease, single-procedure models. It not only considers the patient’s primary diagnosis and single treatment modality during hospitalization but also takes into account factors such as age, disease severity, comorbidities, and complications, thereby stratifying patients into multiple groups for management.
Taking Beijing as an example, inpatient cases collected annually by local hospitals cover approximately 20,000 disease types. DRG grouping categorizes these cases into several hundred groups. Each group contains diseases and treatments with similar characteristics, while there must be significant statistical differences between groups.
DRG grouping is based on the information contained in the medical record face sheet. Therefore, the completion of the hospital medical record face sheet is crucial for correct DRG assignment. In general, the medical record face sheet typically covers four categories of information: patient demographic data, disease diagnosis information, inpatient treatment information, and cost information.
Patient demographic information, including gender, age, national ID number, contact details, and payment method. The second category comprises diagnostic information for the current hospitalization, including the primary diagnosis leading to admission as well as related comorbidities and complications. The third category details the specific treatments received during this hospitalization, such as surgical procedures, medical management, radiotherapy, or chemotherapy. Finally, cost information covers the expenses incurred for each of the aforementioned diagnostic and therapeutic services.
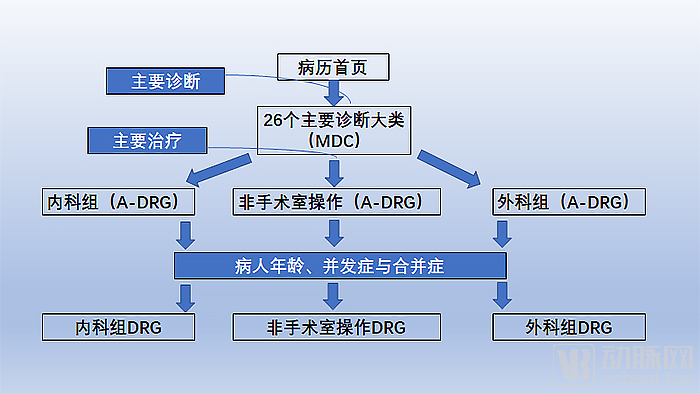
DRGs are grouped based on this information. Cases are first assigned to one of 26 Major Diagnostic Categories (MDCs) according to the principal diagnosis. This classification follows the ICD framework, organized by anatomical systems rather than by clinical specialties commonly used in hospitals. Under this classification scheme, diabetes is categorized under endocrine disorders.
Next, DRGs are further subdivided based on the primary treatment modality for the disease. Cases treated with medical (non-surgical) management are assigned to medical groups, while those treated surgically are assigned to surgical groups. Taking neurological disorders as an example, if surgery is required, the case is classified under neurosurgery; if conservative treatments such as thrombolytic therapy for cerebral thrombosis are employed, it should be categorized under neurology.
Certainly, certain aspects of China’s specific healthcare context require special handling during this grouping process. For instance, in addition to surgical procedures, the traditional fee schedule includes interventional diagnostic and therapeutic procedures. Strictly speaking, such invasive procedures should be categorized under surgeries. However, within China’s healthcare system, interventional procedures are performed across multiple departments, including internal medicine, radiology, and surgery, with some hospitals even establishing dedicated interventional medicine departments. Moreover, an interventional procedure may transition into a surgical operation at any time; for example, when stent implantation is deemed necessary following confirmation via interventional diagnostics. Therefore, non-operating room procedures, such as interventional diagnostics and therapies, are classified separately into a distinct procedural group.
Subsequently, experts in each clinical specialty categorized the diseases within their respective fields into several major groups based on the complexity of the conditions and the difficulty of treatment.
This grouping process is primarily based on clinical experience. Taking obstetrics and gynecology as an example, all surgeries related to malignant tumors, such as radical surgery for ovarian cancer and cervical cancer, are grouped separately; outpatient procedures, including intrauterine device (IUD) removal, IUD insertion, dilation and curettage (D&C), and induced abortion, form another group; among inpatients undergoing surgery, those who undergo hysterectomy are placed in one group, while those who do not undergo hysterectomy are placed in another.
Consequently, the seemingly diverse array of surgical cases was ultimately categorized into four or five groups. Theoretically, variations in costs and length of stay within each group should fall within one standard deviation of the mean, with statistically significant differences observed between groups.
Such grouping is performed by clinicians based on their clinical experience. During the design phase, statistical calculations must also be conducted using data collected from hospitals to confirm whether there are sufficient differences between the groups.
This level of grouping is referred to as A-DRG. Currently, the National Healthcare Security Administration only defines groupings down to the A-DRG level; more granular subgroupings below this level are further refined by individual provinces and municipalities to address the significant regional disparities across China.
A-DRGs require further stratification based on patient age, comorbidities, and complications. For instance, although both a 28-year-old adult and an 88-year-old elderly patient with sequelae of stroke, diabetes, and various other chronic conditions are hospitalized for acute appendicitis, they differ significantly in length of stay, hospitalization costs, and future disease progression.
This marks the completion of the entire DRG grouping process.
The next step after completing DRG grouping is to assign different weights to each group, based on the average cost per hospitalization. The emphasis on a single hospitalization episode is intended to avoid complications arising from departmental transfers during the stay. For instance, a patient admitted to the gynecology department for uterine fibroids may be transferred to the oncology department after being diagnosed with lung cancer upon examination. In such cases, the discharge record would reflect treatment in two departments, making it inappropriate to set weights using this approach.
Counselor Deng Xiaohong further illustrated this point with a past case in Beijing. At that time, a patient was hospitalized for nine months at a certain hospital due to uterine fibroids, incurring exorbitant costs and sparking significant public outcry. Subsequent investigation revealed that while the patient was indeed admitted for uterine fibroids, lung cancer was detected during preoperative examinations. The patient was then transferred to the oncology department for lung cancer treatment, before being transferred back to the gynecology department for management of the uterine fibroids. Following a hysterectomy, the patient developed deep vein thrombosis in the lower extremities. These combined factors resulted in the patient’s prolonged hospitalization of up to nine months.
In this example, the error lies in the fact that two separate hospital admissions should have been recorded based on different admission diagnoses: first for lung cancer, and subsequently for uterine fibroids.
The calculation of group weights is straightforward: it is the ratio of the average cost of a specific group to the average hospitalization cost for all diseases.
Assuming a region has 3 million discharged cases per year, with an average hospitalization cost of 15,000 yuan. The average cost for vaginal delivery in the region is 5,000 yuan; its ratio to 15,000 yuan is 1/3, i.e., a group weight of 0.33. Correspondingly, the cost for coronary artery bypass grafting (CABG) in the region is 300,000 yuan, so its weight should be 20.
Based on such grouping and weighting, administrative departments can not only use DRGs to evaluate the performance of inpatient medical services but also manage inpatient medical costs. Compared with previous approaches, this management model offers significant advantages.
How DRGs Are Used in Hospital Performance Evaluation
Historically, regulatory authorities have primarily evaluated hospitals based on average length of stay (ALOS) and average hospitalization costs. However, for a cohort of 1,000 inpatients, hospitals that predominantly treat complex cases will naturally exhibit higher ALOS and average costs. Evaluating hospitals using such metrics incentivizes them to subconsciously avoid admitting critically ill patients, as a higher volume of severe cases adversely affects their performance indicators.
DRG does not employ such a calculation method; it accounts not only for the severity and complexity of diseases but also for the difficulty of treatment modalities. However, DRG is not a panacea; it is designed specifically to manage short-stay cases in large hospitals, such as those involving acute and critical illnesses, emergency resuscitation, and inpatient surgeries.
Among current payment schemes, community services, outpatient services, traditional Chinese medicine (TCM) hospitals, and long-term rehabilitation and nursing hospitals are also included. Counselor Deng Xiaohong believes that community services, outpatient services, long-term care services, and traditional TCM services (i.e., holistic diagnosis and treatment in the traditional sense, utilizing regulatory therapies to facilitate disease recovery and long-term care) are not suitable for DRG-based payment.
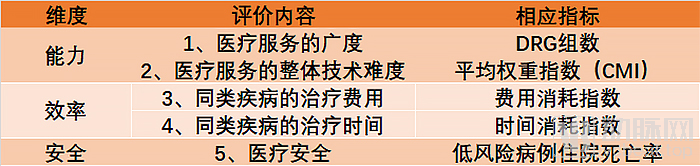
The primary focus of medical administration departments is to ensure healthcare quality and patient safety. Historically, hospital evaluations have often been limited to hardware metrics, such as the number of beds, equipment, staff with senior professional titles, publications, and research projects, lacking an objective indicator to assess the level of clinical performance. DRG precisely addresses this gap by enabling the evaluation of healthcare service capability across three dimensions: capacity, efficiency, and safety.
DRG-based evaluation of medical capability is primarily achieved through two indicators: the number of covered DRG groups and the Case Mix Index (CMI). These two indicators represent the breadth and depth, respectively, of a hospital’s medical service capabilities.
The number of covered DRG groups serves as a metric for assessing a hospital’s comprehensive service capacity; greater coverage indicates more extensive technical capabilities. For instance, if the obstetrics and gynecology department comprises 10 DRG groups and a hospital has managed cases across all 10 groups over the past year, this demonstrates that the department offers comprehensive services. Similarly, if one general hospital covers more than 400 DRG groups in a given year while another covers only slightly over 200, the latter is considered to have insufficient comprehensive service capacity.
Case Mix Index (CMI) is used to measure the technical complexity of overall medical services; a higher CMI indicates greater complexity. Assuming the average CMI for hospitals in a certain region is 1, Hospital A has an average CMI of 1.5 with the same number of cases, while Hospital B has only 0.7. Clearly, Hospital A demonstrates a higher level of technical proficiency, whereas Hospital B exhibits a lower level.
In addition, efficiency is also an important metric. The average cost and average time after weight adjustment can measure the efficiency of hospitals.
Finally, there is safety. Regulatory authorities need to pay special attention to low-risk inpatient mortality rates, as this indicator is associated with issues in a hospital’s clinical care or management.
These indicators have begun to be adopted in the evaluation of the front page of medical records in public hospitals across China, particularly the average case weight and medical safety indicators. It is reported that the results will be released soon.
How Are DRGs Used for Health Insurance Payment?
So, what are the differences between using DRGs for health insurance payment and for hospital performance management? Counselor Deng Xiaohong believes that when the same grouping scheme is applied to payment, the health insurance department needs to determine the rate based on DRG weights, i.e., the amount paid by the health insurance department for each weight.
The National Healthcare Security Administration publicly discloses the total annual expenditure, and dividing this amount by the total relative weight yields the conversion factor. For instance, if Beijing allocates RMB 20 billion annually for short-term acute inpatient care, dividing this expenditure by the sum of relative weights for all short-term acute patients across all hospitals in Beijing from the previous year determines the conversion factor.
After this system has been in operation for several years, the Healthcare Security Administration will be able to inform hospitals of the annual conversion factor based on the budget. This is because healthcare insurance revenue is predictable, determined by local socioeconomic development and the average social wage, and the total relative weight units are also known.
During hospital settlement, each case is assigned to a specific Diagnosis-Related Group (DRG) with a fixed weight. The inpatient cost is calculated by multiplying the weight by the payment rate. The amount payable by medical insurance is determined by multiplying this cost by the reimbursement ratio, with the remaining balance borne by the patient.
Currently, the maximum reimbursement rate published by medical insurance authorities can reach up to 90%, but its calculation involves numerous restrictive conditions. These restrictions include non-coverage for expenses below the deductible threshold and above the annual cap, as well as the division of eligible expenses into fully reimbursed and partially reimbursed categories. Additionally, reimbursement ratios vary across different regions. These factors make the calculation of medical insurance payments highly complex.
Counselor Deng Xiaohong believes that DRG-based payment is more transparent and easier to calculate than previous medical insurance payment policies. Taking a certain surgical procedure as an example, an elderly patient with comorbidities may incur costs of RMB 20,000, while a younger patient may only require RMB 3,500, with corresponding relative weights of 1.5 and 0.2, respectively. If the social insurance fund increases by 5% in a given year, the conversion factor can be raised by 5%. Consequently, the original reimbursement amount of RMB 20,000 would increase to RMB 24,000, and the RMB 3,500 amount would rise to nearly RMB 3,700. Conversely, if the average societal wage decreases by 5%, medical insurance funding would also decrease by 5%, and so forth.
The same principle applies to hospitals. Each hospital’s admitted patients are assigned a total weight, and the Healthcare Security Administration need only pay the hospital a global budget based on the payment rate, with any surplus refunded or deficit covered at year-end. The payment rate can be dynamically adjusted in response to fluctuations in healthcare insurance fund revenues, making the calculation straightforward and transparent.
Under the DRG payment system, the Healthcare Security Administration will determine budgets through negotiations with hospitals, without intervening in specific diagnosis and treatment processes. Physicians will naturally control costs while ensuring quality of care, as any budget surplus will become hospital revenue, largely translating into compensation for medical staff. In fact, pharmaceutical costs currently account for over 60% of total expenses in Chinese hospitals, compared to an international average of less than 15%, leaving approximately a 50% margin for cost containment. This incentivizes hospitals and physicians to proactively manage costs.
Meanwhile, hospitals must also prioritize nursing care. In China, the pricing for nursing services deviates significantly from actual costs. For instance, in Beijing, the rate for Level I nursing care remained at just RMB 7 per day for two decades. As a result, hospitals have become increasingly reluctant to recruit nurses, leading to nurse-to-bed and nurse-to-physician ratios in nearly all Chinese hospitals falling below the standards issued by the Ministry of Health.
In fact, high-quality nursing care can significantly enhance the overall quality of medical services. Otherwise, even a high-quality surgical procedure may be substantially compromised by inadequate nursing care, potentially leading to patient safety incidents. Notably, the labor cost of nurses is considerably lower than that of physicians. Therefore, Counselor Deng Xiaohong argues that hospitals must also place greater emphasis on nursing care following the formal implementation of Diagnosis-Related Groups (DRG).
“By starting with a sound payment policy to address all the current shortcomings in clinical practice, healthcare reform can succeed and costs can be controlled only when physicians take the initiative to manage expenses,” stated Deng Xiaohong.
What is the relationship between the “Four Unifications” emphasized by the National Health Commission in recent years and the DRG grouping scheme?
On November 17, 2016, Li Bin, then Director of the National Health and Family Planning Commission, stated in his address at a sub-forum of the 3rd World Internet Conference that the “Four Unifications” for standardized management of clinical data would be achieved by the end of 2016, laying a solid foundation for DRG-based payment.
As the foundational standard for DRG implementation, the “Four Unifications” encompass clinical medical terminology, disease classification coding, surgical procedure coding, and documentation standards for the medical record face sheet.
Among these, as a national pioneer in Diagnosis-Related Groups (DRG), the Beijing Municipal Hospital Administration Institute began researching DRG as early as 1988. Meanwhile, the Beijing Health Information Center started collecting terminology from the front pages of medical records submitted by hospitals across the city in 2003, establishing a terminology database based on an extended clinical version of disease and procedure classifications. After organizing experts from all clinical specialties to validate the terminology, the *Terminology for Disease Diagnoses and Surgical Procedures* was published in 2015.
At the national level, the Chinese Medical Association, as the specialized body responsible for formulating nationwide medical terminology, was authorized by the National Committee for the Examination and Approval of Scientific and Technical Terms to establish the Working Committee on the Examination and Approval of Medical Terminology as early as 1986, with the aim of standardizing medical scientific and technical terms in China. In recent years, it has published and finalized 17 specialized volumes.
Building on this foundation, China launched the initiative to develop standardized clinical medical terminology in 2015. Led by the Beijing Health Information Center, with the participation of the Terminology Review Office of the Chinese Medical Association, Peking Union Medical College Hospital of the Chinese Academy of Medical Sciences, and the First, Second, and Third Hospitals affiliated with Peking University Health Science Center, the project was initiated under the leadership of Counselor Deng Xiaohong. Through several years of effort, the revision of the 2018 Edition of Common Clinical Medical Terminology has just been completed and published by the People’s Medical Publishing House.
Beijing has also taken the lead in China in the development of DRG grouping schemes. At the beginning of this century, Beijing’s social security department sought to pilot DRG-based payment and launched the second round of work on DRG grouping schemes. In 2008, BJ-DRG was successfully developed and began to be applied in medical institutions for the evaluation of clinical specialty severity and for medical payment purposes.
Subsequently, in 2014, Beijing Municipality collaborated with the National Healthcare Security Administration to launch the 2014 version of the CN-DRG grouping scheme, based on BJ-DRG. This scheme was later updated in 2018, resulting in the release of the 2018 version of the CN-DRG grouping scheme.
Currently, CN-DRG has been promoted in hospitals for quality performance evaluation, covering more than 600 medical institutions across 29 provinces and municipalities nationwide. This includes health commissions in 16 provinces and municipalities, as well as 38 information software companies that have signed contracts to use the system.
What are the differences in noun coding used by CN-DRG compared to other versions?
In 2016, the Statistical Information Center of the National Health and Family Planning Commission released a disease classification and coding standard based on ICD-10, known as the Statistical Version (or National Standard Version). It is called the Statistical Version because, historically, China’s use of the ICD standard was primarily for disease statistics, which did not require clinicians to specify every individual disease or surgical procedure in detail.
Therefore, this version contains many statistical terms, such as “tuberculosis of other specified organs.” In clinical practice, however, physicians use specific terminology, such as pulmonary tuberculosis or renal tuberculosis. By comparison, the statistical classification is less detailed and more general.
The surgical procedure classification standards based on ICD-9-CM-3, issued by the Information Center of the National Health Commission, also include terms with obvious statistical connotations, such as “Other puncture of skull base,” “Other incision of brain,” and “Other operations on mouth.”
This standard largely follows China’s historical technical conventions for ICD coding and is suitable for disease statistical analysis. However, further refinement is required when applying it to clinical evidence-based medical research and DRG grouping.
The CCHI (Classification and Coding of Healthcare Service Items), released by the Health Development Research Center of the National Health Commission, was designed to align with the payment framework established by the National Development and Reform Commission, and is commonly referred to as the “payment version.”
The paid version also contains certain terminology that diverges from clinical conventions. For instance, the billing item “radical total gastrectomy” actually encompasses two distinct surgical procedures in clinical practice: total gastrectomy with esophagojejunostomy and total gastrectomy with esophagoduodenostomy. Additionally, procedures such as extrafascial total hysterectomy are not listed in the CCHI and must be categorized under other directories.
Therefore, although the paid version can help hospitals address billing issues, its overly broad definition makes it unsuitable for both clinical documentation practices and evidence-based medical research.
In contrast, the CN-DRG based on the Beijing Clinical Version has always been refined to the 7th digit. Hospitals can use the full code to specify particular clinical procedures.
CCHI cannot be mapped to the currently used ICD-9-CM3. A forced transition would render 26 years of accumulated data and records discontinuous, thereby disrupting related coding techniques, computer software, and evaluation methodologies.
At the same time, CCHI is essentially unable to engage in international exchanges or share and leverage advanced international data analysis technologies and software.
In 2019, after designating 30 pilot cities for Diagnosis-Related Groups (DRG) payment, the National Healthcare Security Administration issued a total of 15 standards to better promote DRG-based payment and unify standards.
The National Healthcare Security Administration has commissioned the Beijing Municipal Healthcare Security Administration to unify the four major DRG systems: C-DRG, BJ-DRG, CN-DRG, and CR-DRG. These versions are widely applied in China. The C-DRG system is led by the Development Research Center of the National Health Commission. The BJ-DRG is a scheme implemented by the Beijing Municipal Healthcare Security Administration. As previously mentioned, CN-DRG actually shares the same origin as BJ-DRG. The difference between the two lies in the fact that the former has been continuously updated for hospital performance evaluation, while the latter was not updated because DRG-based payment had not yet been implemented at that time. The CR-DRG system is primarily used in certain county-level hospitals in Yunnan and Shaanxi provinces as part of DRG pilot programs.
Since C-DRG utilizes CCHI codes, it cannot be mapped to other coding systems and was ultimately excluded from the integration. By merging the remaining three versions, the National Healthcare Security Administration established a unified grouping scheme, namely CHS-DRG, also known as the National Healthcare Security DRG.
CHS-DRG categorizes diagnoses into 26 major groups based on ICD-10, which are further classified into 376 A-DRG groups according to treatment methods. Taking regional differences into account, CHS-DRG does not provide further subdivision at the national level but instead delegates this task to individual provinces for detailed refinement. Consequently, there will be variations in DRG classifications across different provinces.
How the Healthcare System Aligns with DRG Implementation
Counselor Deng Xiaohong offered her recommendations on how provincial health systems should specifically implement Diagnosis-Related Groups (DRG). She argued that the implementation of DRG must first standardize clinical terminology, as well as unify versions and ICD codes.
Subsequently, a unified local entity is required to centrally collect the front-page data of medical records from all hospitals. This entity could be the health administrative department, the healthcare security administration, or even a designated hospital or third-party company. The key requirement is the centralized collection of front-page medical record data from multiple hospitals, coupled with expert-led supervision and inspection of medical record quality. Otherwise, an excessive volume of low-quality data will compromise evaluation outcomes, potentially resulting in the denial of healthcare insurance reimbursements.
Meanwhile, health authorities should regularly release medical evaluation results and facilitate negotiations between hospitals and medical insurance agencies to scientifically and reasonably determine payment rates and reimbursement ratios. It is essential to conduct scientific evaluation and maintenance of Diagnosis-Related Groups (DRGs). The establishment of DRG payment rates and reimbursement ratios should be based on an analysis of statistical data accumulated over the year, rather than being unilaterally determined by either the medical insurance authorities or hospitals alone.
Hospital administrators must standardize the front sheet of medical records and ensure the quality of data entry. Meanwhile, hospitals need to place great emphasis on medical record coding. Coders must correctly understand the diagnoses, surgeries, and procedures documented by physicians, possess extensive coding knowledge and experience, have a solid grasp of relevant clinical knowledge, and thoroughly review the entire medical record. Taking Beijing as an example, due to the current high priority placed on coding by hospital administrators, career prospects for students majoring in health information management are excellent; they are often recruited by large hospitals before graduation.
Hospitals must also prioritize information technology infrastructure, not merely by establishing workstations in operating rooms, ICUs, and wards, but also by automatically integrating all diagnostic and laboratory results into the Hospital Information System (HIS).
Hospitals should also prioritize the balanced development of their medical specialties; otherwise, they will face significant gaps in the breadth of case-mix group coverage.
Hospitals should also prioritize medical quality and cost control. Cost control is of paramount importance, necessitating a change in the currently widespread unreasonable medical practices.
For private hospitals, the implementation of Diagnosis-Related Groups (DRG) will also be a positive development, enabling insured patients to receive their entitled medical insurance reimbursements.
Given that pharmaceuticals and medical consumables account for as high as 60% of the total cost structure in Chinese hospitals, compared with international advanced levels (11% in the Hong Kong Special Administrative Region and only 4% in Germany), there is actually significant room for cost control.
By reducing the costs of pharmaceuticals, consumables, and unnecessary tests, hospitals can reallocate these savings to increase revenue from medical services, creating a virtuous cycle.
Therefore, hospitals need to adopt proactive incentive measures: namely, accurate and rapid diagnosis (misdiagnosis incurs costs); effective and high-quality treatment and nursing care without complications (complications generate additional expenses); well-organized collaboration processes within and between departments (such as timely scheduling of imaging examinations and feedback of laboratory results, as waiting incurs additional costs); immediate initiation of treatment after diagnosis without waiting (preoperative examinations completed in outpatient settings to avoid occupying hospital beds); continuous emphasis on clinical pathways; and appropriate bed capacity with a sufficient volume of specialized cases (excessively large hospitals raise operational costs and create difficulties for patients seeking medical care).