New Era of Smart Hospitals: DRG and Hospital Asset Management Unlocking a Trillion-Yuan Market Opportunity [2019 VB100]
In March 2019, the National Health Commission held a press conference themed “Informatics Quality Control and Smart Hospital Construction.” At the conference, answers were provided to widely concerned issues such as the current status of informatization development and requirements for smart hospital construction. The scope of smart hospitals was clearly defined, primarily encompassing three major areas: “Smart Medical Care” for medical professionals, “Smart Services” for patients, and “Smart Management” for hospital administration.
In the New Era of Healthcare, How Can We Leverage Information Technology to Enhance Hospitals’ Operational and Management Efficiency, Thereby Improving the Quality and Safety of Medical Services and Making Hospitals “Smarter”?
To address this issue, numerous guests presented solutions at the “2019 Future Healthcare Top 100 Conference · Smart Hospital Construction Forum” hosted by VCBeat. Below is a summary of the speakers’ viewpoints, compiled and edited by VCBeat without altering their original meaning.
Zheng Jie, Director of the Beijing Medical Insurance Center
DRG: The Balance Between Management and Clinical Practice
What is DRG? DRG is informatization; it is big data. Without the support of informatization, there would be no DRG as we know it today.
The CHS-DRG framework introduced by the National Healthcare Security Administration on October 27 is undoubtedly of paramount importance, as it serves as the sole instrument for payment. Previously, numerous DRG versions existed; however, without being linked to financial mechanisms, they did not generate significant economic implications. With the implementation of CHS-DRG, the integration of DRG with economic incentives has become inevitable, and health informatization will advance to a new level alongside the maturation of DRG.
So, why has the national healthcare insurance system chosen DRG as the mainstream payment method for the future? The underlying principle lies in the word “balance.”
The equilibrium of DRG represents a balance between management and clinical practice, akin to a scale that must not tip excessively to either extreme. An extreme bias toward fee-for-service leads to significant issues, such as incentivizing overutilization, where physicians are motivated to prescribe expensive medications and high-cost consumables. However, given the limited resources of the medical insurance system, this payment model is unsustainable.
Extreme right-leaning policies also carry risks. Prior to 2010, the health insurance fund had a surplus, so cost containment measures were not implemented. The year 2012 marked a turning point, when the Healthcare Security Administration introduced the most stringent and extreme payment method: global budgeting on a hospital-wide basis. This ushered in an extensive era of cost containment. While this approach proved effective for administrators, it gradually gave rise to another problem: clinical development became constrained, leading to a lack of positive incentives for physicians.
In the future, we must strike a balance between management and clinical practice, which is what we refer to as DRG-based payment. This model involves bundled payments to hospitals on a per-disease basis, taking into account both managerial considerations and clinical needs. Specifically, reasonable cost standards are established for each disease entity to control health insurance expenditures. From a clinical perspective, physicians who demonstrate greater competence and capability can attract more patients, thereby generating higher revenue.
Prior to the implementation of Diagnosis-Related Groups (DRGs), the World Health Organization’s internationally recognized codes for disease diagnoses and surgical procedures were highly fragmented: there were 34,889 diagnosis categories and 13,002 surgical procedure codes. Furthermore, different diagnoses may require different treatment approaches, while the same treatment modality may be applied to various diagnoses. Consequently, the actual number of required codes exceeds 50,000, reflecting the considerable complexity of clinical practices.
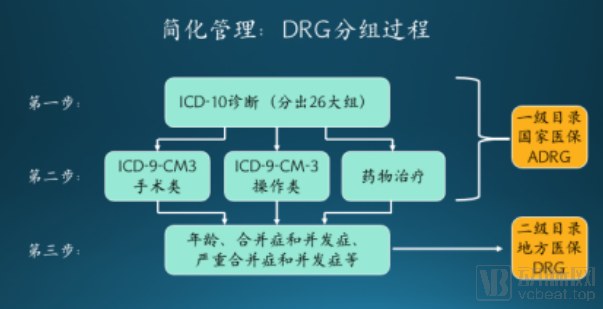
Following the implementation of DRGs, we integrated disease coding with procedural coding to transform complex and disordered clinical practices into a streamlined and systematic framework. Ultimately, over 50,000 code groups were consolidated into 600–800 DRG categories.
The principles underlying patient grouping can be broadly broken down into three steps. First, based on patients’ medical record information and diagnosis codes, we initially categorize them into 26 major groups, encompassing 26 broad categories such as orthopedics, hematology, and endocrinology. Second, further stratification is performed according to the patients’ diagnoses to form Adjacent Diagnosis-Related Groups (ADRGs), also known as core DRGs. Specifically, patients are further grouped based on treatment modalities, surgical procedures, non-surgical interventions, and medication use, resulting in more than 400 subcategories.
Upon completion of the first two steps, the empirical component of clinical practice is concluded. At this critical third step, the importance of informatization and big data becomes evident. Since individual patient variations preclude the application of a single clinical pathway to all cases, it is essential to leverage big data to identify differences among patients within the same clinical pathway.
Upon completing the “third step” of “aggregating patient individual differences via big data,” the entire grouping process is concluded. The final number of groups formed ranges from approximately 600 to 800, which are heavily underpinned by “big data management.”
"Business opportunities" lie here.
Prior to the implementation of Diagnosis-Related Groups (DRG), medical coding was predominantly handled by hospital medical records departments, with minimal adoption of artificial intelligence or other technologies for automated coding. However, in the emerging DRG era, the volume of coding tasks will far exceed the capacity of human coders, necessitating technological assistance. Therefore, DRG serves as a test of hospitals’ foundational operational capabilities, propelling medical records management and coding to the forefront of healthcare administration.
Many hospital directors have increasingly felt the pressure that coding work places on hospitals in recent years. One director once said to me, “Director, I’ve realized that the medical records department was indeed undervalued in the past, with many retired head nurses assigned there as a form of semi-retirement. Going forward, I intend to completely overhaul the staff, replacing them with professional medical records personnel, because medical records hold the key to our hospital’s future financial lifeline.”
The hospital director is correct, but it should be clarified that the future economic lifeline will not be controlled by humans, but by information technology and artificial intelligence. Therefore, several tools optimized for intelligent coding in our hospital are bound to emerge, helping us identify reasonable opportunities within our health insurance management. I believe this is what is referred to as “business opportunities” in DRG.
Many people believe that a mature DRG system follows a “one-size-fits-all” approach, but CHS-DRG has broken this pattern. China’s DRG system adopts a two-tier directory structure for management. The first-tier directory, namely ADRGs, covers only the clinical aspects, whereas the development of the second-tier directory requires collaborative input and contributions from stakeholders.
The disparities among various provinces and municipalities cannot be overlooked; the national aggregated average data inevitably deviates from regional realities: there are gaps in economic development, levels of healthcare coverage, and disease spectra... Therefore, we encourage each province and municipality to independently determine weighting factors based on their own data and to formulate their own secondary catalogs.
When will DRG be officially implemented? Currently, the National Healthcare Security Administration has formulated a three-year plan. The goal for 2019 is to complete the top-level design, requiring the Administration to develop a national DRG scheme. In 2020, this scheme will be distributed to 30 cities, with each city selecting one hospital to conduct pilot simulations. By 2021, payment implementation will commence. This constitutes the overall three-year roadmap.
Therefore, the primary task in 2020 was to conduct simulation runs in pilot cities: hospitals uploaded information and data to us; we utilized this data to complete patient grouping, determining “which group each patient should be assigned to” and “how much the medical insurance would pay,” and then fed this information back to the hospitals, thereby concluding the entire simulation. No actual DRG-based operations were implemented during that year. We aimed to provide hospital physicians with ample time to prepare, allowing them to shift their mindset and independently reduce inefficiencies. Our goal was to avoid a scenario where hospitals incurred large-scale losses immediately upon policy implementation.
I have always maintained one point: rather than saying the future of DRG belongs to hospitals or pharmaceutical companies, it is more accurate to say that it belongs to our health informatics and artificial intelligence. In the future, a robust health informatics system and high-quality AI technology may become the decisive factors determining the economic lifeline of hospitals.
Lin Hui, Director of the Office of Internet and Artificial Intelligence, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine
“Connectivity” and “Synergy” Transforming Healthcare
The allocation of medical resources has long hindered the development of healthcare services in China. While we have consistently attempted to address this issue by “changing models,” technological advancement is equally crucial for the effective implementation of tiered diagnosis and treatment.
The proposal of the “Healthy China 2030” strategic plan signifies that Healthy China will shift from being “treatment-centered” to “health-centered.” To achieve this transition, it is essential to establish both a health education system and a medical service system.
The purpose of the health education system is to improve residents' health literacy, while the purpose of the medical service system is to ensure that people can access, afford, and receive effective medical care when they fall ill. These two systems complement each other, with the medical service system serving as the foundation. The key to building a robust medical service system lies in focusing on two aspects: strengthening primary care to provide a safety net, and establishing centers of excellence to lead innovation. Current healthcare reform policies are closely aligned with these two priorities, aiming to consolidate primary care and elevate top-tier medical capabilities. Ultimately, the new ecosystem of medical and health services revolves around these two pillars, forming a hierarchical diagnosis and treatment system characterized by vertical coordination, clear division of labor, and efficient operation.
The Internet and artificial intelligence (AI) play a pivotal role in advancing the construction of this system, leveraging their inherent technical characteristics and value propositions. The essence of the Internet lies in connectivity, which facilitates the formation of an integrated system that enables efficient operational collaboration and resource integration within the system. The essence of AI resides in algorithms, which emulate human-like thinking to enhance work efficiency and capabilities. By harnessing these two technologies, we can achieve collaborative synergy between tertiary and primary care institutions, strengthen the healthcare service delivery capacity at the grassroots level, and jointly promote the development of a comprehensive medical and health service ecosystem.
Let us first discuss the Internet. Taking Sir Run Run Shaw Hospital of Zhejiang University School of Medicine as an example, we have established the "Shaoyi Health Cloud Platform," achieving both vertical and horizontal connectivity. Vertically, supported by Sir Run Run Shaw Hospital, we leverage internet technologies to connect district- and county-level hospitals, township health centers/community health service centers, and village clinics/medical practices, thereby constructing a four-tier regional medical service system linking provincial, county, township, and village levels. Horizontally, we utilize the Internet to break down industry boundaries, focusing on healthcare while integrating regional commercial insurance, social security, bank payments, and pharmaceutical logistics, thus realizing collaborative coordination among the three key sectors of healthcare (medical services, health insurance, and pharmaceuticals). Through this vertical and horizontal connectivity, we have initially built a tiered diagnosis and treatment service system characterized by regional collaboration and coordination, achieving efficient integration of regional healthcare resources and operational synergy. This enables residents in the region to access more convenient, high-quality, efficient, and safe healthcare services.
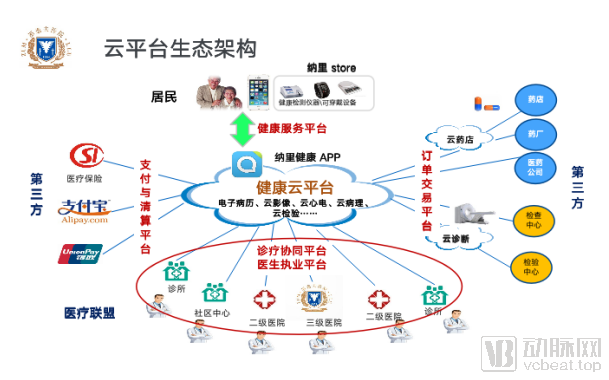
The cloud platform comprises three core business platforms: the Medical Collaboration Platform, the Family Doctor Contracting and Integrated Medical-Nursing-Care Platform, and the Resident Health Service Platform. These three platforms operate in synergy to form a complete closed-loop medical service system. Currently, the platform offers ten common service functions, including remote health consultations, appointment scheduling, online payment, two-way referrals between primary and tertiary care institutions, remote mobile referrals, integrated pharmaceutical services (Internet-based prescriptions plus drug delivery), regional coordination of examinations and laboratory tests, remote joint outpatient consultations/ward rounds, an Internet-based Education Academy, and family doctor contracting with integrated medical-nursing-care services. The realization of value from these functions truly fosters a pyramid-shaped regional medical service ecosystem characterized by vertical collaboration and win-win cooperation among all stakeholders.
# Revisiting Artificial IntelligenceThe biggest challenge currently facing the development of medical AI is not algorithmic issues, nor problems with R&D personnel, but rather the availability of medical data required for development.
Leveraging its robust foundation in hospital informatics, Sir Run Run Shaw Hospital now possesses 26.8 million complete electronic medical records and is exploring the use of this data to develop medical AI products.
Our inaugural product is a general-practice-oriented intelligent clinical decision support system, designed to enhance the clinical proficiency of primary care physicians and reduce rates of missed and misdiagnoses. The core technology underpinning this system combines “knowledge graphs + neural networks.” The knowledge graph is built upon existing medical knowledge bases, while the neural network models are trained on vast amounts of clinical data, ultimately enabling clinical decision-making that integrates both empirical experience and rule-based logic.
Next, we will leverage this system to extend development both front-end and back-end. On the front end, we will develop an intelligent health management system to provide the public with smart health assessments, health guidance, and triage services. On the back end, we will deepen our specialization in specific medical fields and diseases to help enhance the efficiency and capabilities of specialists and expert physicians.
Zhang Lehui, Operating Partner at Changling Capital
The Impact of DRG on Industry Strategy and the Fission of Management
DRG impacts industry policies, health economics, intra-industry social relations, and medical technologies. For instance, as a critical tool in health economics, DRG plays a vital role in actuarial calculations within the “Three-Medical Linkage” healthcare reform policies, which encompass medical insurance management, tiered diagnosis and treatment, and the separation of prescribing from dispensing.
In the DRG era, public medical institutions, pharmaceutical companies, and medical device manufacturers face opportunities amidst challenges, while for commercial health insurance providers and privately funded healthcare entities, opportunities outweigh challenges.
Public hospitals need to change their operational models. For example, due to the long-standing 15% markup policy, the pharmacy department failed to establish a service-based pricing system. With the disappearance of the “drug-revenue-subsidized medical care” model, the pharmacy department faces significant challenges. In the DRG era, however, the value of the pharmacy department has been reaffirmed.
Pharmaceutical and Medical Device Companies Face Challenges: Seizing Market Opportunities by Understanding the Differential Impact of DRG-Based and Fee-for-Service Payment Models on Medical Device Demand; Adapting to Healthcare Institutions’ Lean Management Needs by Diagnosis-Related Groups to Enhance Efficiency; and Aligning with Value-Based Healthcare Trends Through Technological Innovation.
Since DRG payment standards define the boundary between basic medical care and special-needs medical care for different disease groups, commercial health insurers should respond swiftly by leveraging health insurance technology to launch comprehensive coverage products for all disease groups.
Facing DRG payment standards, it is a market share competition that does not rely on "face recognition." Social capital in healthcare should leverage its operational flexibility to seize opportunities for rapid growth amidst existing reforms.
Zhu Haiwen, Co-founder and General Manager of HealthEngine Medical
Medical Equipment Maintenance Enters the Era of Intelligent "Full Lifecycle Management"
When we fall ill, what we want is to find the most professional doctors for the most timely diagnosis and treatment in the shortest time. Meanwhile, physicians require the most accurate and up-to-date data to serve as the basis for their clinical decisions. However, few people ever consider the question: “Do the medical devices themselves meet the required standards, and can they provide accurate data?”
For example, my home mercury sphygmomanometer broke, so I went to a pharmacy and used a mercury sphygmomanometer from a well-known brand for measurement. The doctor took my blood pressure three times and obtained three different results. In our logic, a mercury sphygmomanometer should not produce deviated results, as it is a basic and simple tool. However, the fact remains that any instrument, from thermometers to CT scanners, can malfunction.
This is the mission of HealthEngine. As a professional medical equipment management company, we aim to address such challenges through our work.
What Is the Current State of Medical Equipment Management? In healthcare institutions, medical equipment management is lacking, the status and role of clinical engineering departments are marginalized, manufacturers monopolize technical support and spare parts, and in-house maintenance capabilities are insufficient.
Unreasonable role assignments lead to inadequate management. The absence of a comprehensive lifecycle management system results in an inability to monitor equipment operational status, leaving critical gaps in tracking the functional status and utilization efficiency of each device.
Furthermore, the lack of quality control and insufficient biomedical engineering maintenance capabilities are also significant issues at present. This problem stems from the relationship between production relations and productive forces; outdated production relations fail to adequately meet the demands of advanced productive forces, which reflects the current general state of medical equipment management.
However, this sector boasts a market size of RMB 200–300 billion. According to data referenced in the Blue Book on the Development of China’s Medical Device Industry, the annual total sales volume of medical devices amounts to several hundred billion yuan, while the total stock of medical equipment assets reaches the trillion-yuan scale, maintaining an annual growth rate of 20% to 30%. For tertiary hospitals, expenditures on medical equipment management account for approximately 4% to 8% of their total assets, whereas for secondary hospitals, this figure ranges from 1% to 3%. This presents significant potential opportunities.
To address challenges and seize opportunities, the philosophy of medical equipment management among hospitals, markets, and investors has undergone significant changes in recent years, primarily manifested in three aspects: standardization, informatization, and intensification. Standardization is achieved through medical equipment management platforms covering the entire lifecycle or via technical means to establish comprehensive operational protocols for medical equipment. Intensification involves the emergence of integrated third-party management companies that consolidate all medical equipment within a hospital or across several departments for unified management. Informatization drives the professional advancement of clinical engineers, enabling them to master maintenance skills for a wider range of products.
HealthEngine aims to seize opportunities through these changes. As a high-tech enterprise specializing in the intelligent management of medical equipment, we leverage our independently developed medical equipment management platform, internet-based technologies, and the mining and application of big data from medical devices to achieve automated management. This approach enhances equipment utilization efficiency, reduces costs, mitigates various operational risks, and ensures the proper functioning of medical equipment.
In terms of business model, HealthEngine leverages a full-lifecycle medical equipment management platform to achieve intelligent management of medical devices, thereby improving operational efficiency and reducing costs.
In the future, HealthEngine aims to shape the future of medical equipment management by leveraging its advantages, including standardized specifications and professional, efficient services.
Zhai Xuelian, Vice President of Zhuojian Technology
A true internet hospital must cover the entire process, including pre-consultation, during-consultation, and post-consultation stages.
From the overall perspective of the healthcare sector, policy-driven initiatives are fostering an increasingly open environment, while “Internet + Healthcare” has proven in practice to be one of the key tools for enhancing efficiency in future healthcare delivery.
Zhuojian Technology’s Smart Internet Hospital stems from its “All-in-One” solution, formed by integrating all product lines over the past eight years. The Smart Internet Hospital has now advanced to version 3.0. At this stage, the Internet Hospital not only enables patients to register and make payments online, but also provides hospital-side services such as text-and-image consultations, video consultations, and medication delivery. Furthermore, it integrates internal hospital resources—including medical technology departments and inpatient beds—to serve patients, thereby assisting physicians in managing both outpatient and inpatient care through a framework of “one intelligent engine plus five centers.” By adopting this professional, intelligent, full-process patient management model that combines online and offline services, Zhuojian Technology ensures that its Internet Hospital truly meets patient needs. Behind these services, Zhuojian’s Internet Hospital 3.0 leverages an intelligent engine powered by a medical knowledge base and disease-specific rules to connect various entities, serving patients while providing efficiency support to healthcare institutions.
Internet Hospital 3.0 delivers professional, intelligent, end-to-end internet-based medical services that encompass pre-hospital, in-hospital, and post-hospital health care. This model genuinely helps hospitals reduce health management costs and improve diagnostic and treatment efficiency, aligning with the overarching direction of China’s healthcare reform policies. Furthermore, from an intra-hospital perspective, this model is poised to provide greater value in chronic disease management, scientific research, and clinical medication studies in the future.
So, are internet hospitals truly a necessity for every hospital? In the thirty-year history of medical informatization, internet hospitals are merely young newcomers, representing the first time that in-house physicians and various resources have been genuinely made available online to serve patients. Hospital operations are inherently complex, and establishing an internet hospital involves nearly all departments across the institution. If hospitals merely perform the “mandatory actions” without strategic depth, they will fail to generate incremental revenue, inevitably turning the internet hospital into a cost center rather than a profit driver. Drawing parallels from other industries, not all restaurants offer food delivery services; however, those that do not are invariably impacted by the rise of delivery-focused competitors. Medical institutions, as even more complex operational entities, face similar dynamics. Engaging in internet hospital services must be viewed as a long-term commitment requiring deep cultivation. From this perspective, today’s internet hospitals are still only in their initial stages.
Ge Qiuju, Founder of Depin Medical
Smart Nursing: An Imperative
As the saying goes, “30% treatment, 70% nursing,” yet there is always a gap between ideal and reality.
China currently has approximately 8 million healthcare professionals. The number of registered nurses surpassed 4 million in 2019; while this figure appears substantial, it is not so in reality.
From an international perspective, the doctor-to-nurse ratio in the UK, US, and Japan is approximately 1:4, whereas in China it stands at 1:1. The shortage of nursing staff has, to some extent, contributed to the occurrence of doctor-patient disputes, while nurses themselves often face significant inequities in terms of compensation and working conditions.
Against this backdrop, improving nursing efficiency and enhancing nurses' compensation have become urgent priorities.
Driven by this demand, Suzhou Depin Medical Technology Co., Ltd. has developed Smart Nursing Solutions. As various industries leverage intelligent methods to achieve their goals, the nursing sector must also enhance efficiency through digitalization.
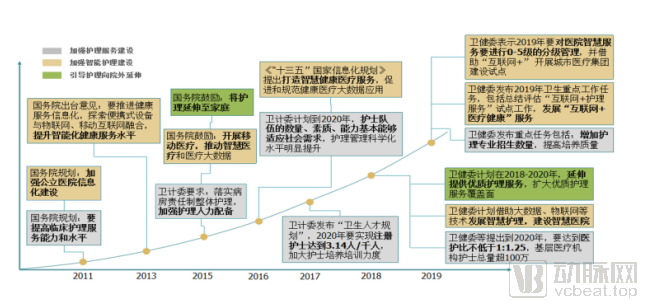
In this regard, national policies have provided substantial support, aiming to leverage policy measures to heighten the attention of hospitals, physicians, patients, and enterprises toward nursing talent and care quality; to facilitate the upgrade of nursing services from informatization to intelligentization; and to encourage the extension of nursing services beyond hospital settings.
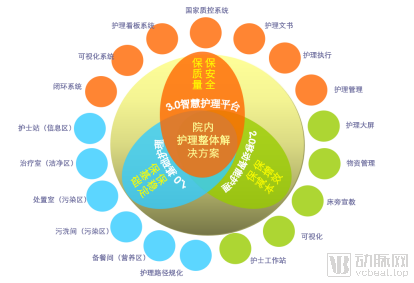
To advance the upgrading of nursing services, we have adopted “Internet + Nursing Services” as our primary model and launched a SaaS platform for out-of-hospital care. This system enables standardized nursing practices across all grassroots community settings outside the hospital, extending care to homes and specifically serving elderly individuals as well as those with disabilities or partial disabilities.
Within the hospital, we focus our system on discipline development, nursing quality, operational efficiency, and cost savings. By leveraging technologies such as artificial intelligence and the internet, and while ensuring data security, we structure and visualize the entire nursing workflow to break down information barriers and enhance nursing efficiency.
To date, Suzhou Depin Medical Technology Co., Ltd. has served more than 300 hospitals, established 10,000 nursing units, and covered approximately 500,000 hospital beds. Moving forward, we will continue to advance smart nursing solutions, enabling more hospitals and patients to benefit from next-generation nursing services.
Chen Lianzhong, CTO of Goodwill E-health Info Co.,Ltd.
CDSS Needs to Truly Align with Clinical Practice
From the expert systems of the past to today’s AI-powered Clinical Decision Support Systems (CDSS), we have always endowed them with immense potential for innovation.
Whereas traditional navigation systems merely provided route directions to a destination, modern navigation platforms offer real-time traffic updates and trip cost estimates. Similarly, we envision Clinical Decision Support Systems (CDSS) delivering genuine, actionable clinical support to physicians.
The healthcare industry has always been policy-driven, with grading requirements propelling the rapid development of the CDSS market. However, CDSS itself is evolving toward clinical applications, prompting the market to consider: what problems can CDSS truly solve? At present, CDSS can enhance physicians’ capabilities in scientific research and clinical decision-making.
Current CDSS must fulfill four key requirements: First, it must adhere to evidence-based medicine, which serves as the fundamental basis of CDSS. Second, it must integrate real-world data; relying solely on traditional evidence-based medicine makes it difficult for CDSS to align with actual clinical scenarios in hospitals. Third, it must adapt to clinical workflows. Since healthcare is a dynamic process, a major challenge for CDSS is effectively leveraging data collected during the consultation process to enhance patient care. Fourth, it must be tailored to different user groups. Primary care hospitals and advanced medical institutions have distinct needs, so CDSS solutions must be customized accordingly.
So, how will it develop in the future? CDSS that can solve clinical problems is an inevitable trend. We cannot merely use CDSS for rating purposes, as this is not its true value. Therefore, we need to develop in-depth CDSS and continue to explore this field.
Hualian Medical CEO Liu Feng: Big Data Research Lacks Longitudinal Pathways and Scientific Orientation
Nowadays, many practical problems in patients' lives can be solved with data. There are also enough data processing platforms on the market, but the gap between data has not been bridged, and data has not been truly utilized.
Why has the current situation arisen? There is a lack of an integrated platform to support process standardization and outcome translation, connecting data application, storage, analysis, and visualization, digitalization of health and medical information, data production, and regulatory support departments into a unified system. This disconnect has led to a gap between data generation and data utilization. Hualian Medical aims to build such an industry-spanning comprehensive platform to maximize the utilization of data.
To this end, Hualian Medical has developed a data aggregation platform that processes data using big data GP+Hadoop+massive data retrieval and positioning+AI pattern matching, and adopts alliance distributed blockchain to ensure data security and immutability, thereby achieving cross-hospital data sharing.
In terms of business model, we pursue a dual-track strategy targeting both B2B and B2C markets. Our B2B services include Contract Research Organization (CRO) solutions and real-world data studies, while our B2C offerings leverage our mobile app to provide cardiovascular disease risk prediction for Chinese residents.
All services are data-driven, enabling us to leverage data more effectively and deliver superior service quality. In the future, the Hualian team will continue to explore data mining and applications, harnessing big data to truly transform healthcare services.
At the forum, VCBeat released the "2019 Industry Development Report on Smart Healthcare." VCBeat reviewed over 200 technology enterprises, deconstructed the pathways for smart hospital development, and defined a handbook for smart hospital construction. Through our in-depth and comprehensive research and analysis, we aim to provide highly valuable references for all stakeholders involved in smart hospital development.
The new generation of national leaders has elevated the digital economy to a strategic priority, proposing the deep integration of digital technologies—such as the internet, big data, and artificial intelligence—with the real economy, so as to develop the digital economy and build a Digital China. Consequently, digital innovation will become a new growth point and driver for China’s economic development. Digital innovation refers to the application of new technologies, including the internet, big data, artificial intelligence, and the Internet of Things (IoT), to various stages such as research and development, production, distribution, and sales. This empowers existing industrial operational mechanisms and models, reduces costs, improves efficiency, and promotes faster and better industrial development.
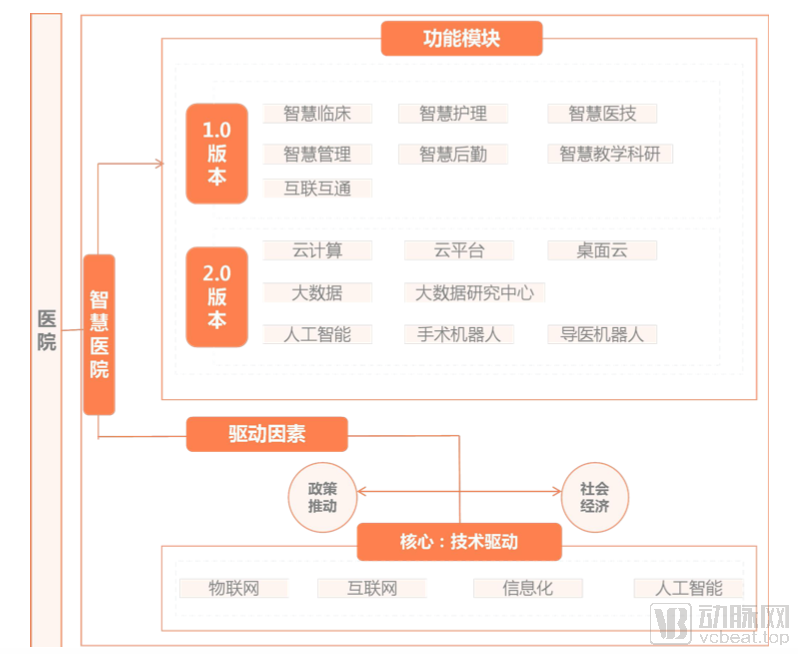
Under the guidance of policy, “Smart Hospitals” have emerged. A smart hospital is neither a mere accumulation of technologies nor a synonym for any single function. Rather, it is a healthcare institution characterized by informatization, internet integration, and intelligence. Informatization refers to the establishment of multi-dimensional data systems and their integration across various dimensions within the hospital. Internet integration denotes the deployment of mobile applications that enable medical staff and patients to input and output data throughout the pre-consultation, during-consultation, and post-consultation phases. Intelligence involves the application of big data, cloud computing, Internet of Things (IoT) technologies, automated equipment, robotics, and intelligent workflow and operational management systems. Smart hospitals facilitate interconnectivity among patients, medical personnel, healthcare institutions, and medical devices, thereby enhancing hospital operational efficiency and optimizing the experience of medical services across the pre-consultation, during-consultation, and post-consultation stages.
The above is an excerpt from the report. To download the full report, please scan the mini-program QR code below.
