Global Healthcare Violence Governance: A Pyramid Model Based on Comparative Analysis of 16 Countries
Recently, Dr. Yang Wen from the Civil Aviation General Hospital was maliciously attacked by a patient’s family member and passed away despite emergency rescue efforts. The Beijing Procuratorate has approved the arrest of the suspect on charges of intentional homicide. The National Health Commission held a press conference, expressing deep sorrow and outrage over the incident. It explicitly stated that this is not a doctor-patient dispute but an extremely serious criminal offense, and the perpetrator will inevitably face severe legal punishment.
Yes, we are deeply saddened by the loss of a physician and utterly enraged by the perpetrator’s actions. Nevertheless, we strive to restrain these emotions and calm ourselves to seek practical solutions, with the hope that healthcare workers will receive more effective protection in the future.
First, it is essential to clarify the conceptual framework. Regarding similar incidents, the prevailing terms currently used both domestically and internationally include “violence against medical personnel,” “violent injuries inflicted on medical staff,” “workplace violence in healthcare settings,” and “hospital violence.” Some Chinese scholars have defined this phenomenon as “medical violence,” referring to individual or collective acts of violence occurring within medical spaces (or domains) and directed at healthcare professionals or medical institutions. For individuals, this encompasses not only direct physical assaults but also psychological pressure tactics such as intimidation and threats. For institutions, it includes both direct infringing acts—such as property damage and physical injury to staff—and coercive behaviors that disrupt the normal operational order of the institution through violent threats.
Given that the concept of “medical violence” comprehensively captures the meanings of other common terms, does not emphasize whether the outcome is “injury” or “death,” and can describe violent incidents with a variety of outcomes, thereby offering broader applicability, we have adopted this concept in this article.
Applying this concept, we have examined and analyzed the current status of violence against healthcare workers and governance approaches in 16 countries, and will explore effective strategies to protect healthcare professionals from the following aspects:
1. Is medical violence a regional issue?
2. Are there discernible patterns in the measures taken by various countries to govern medical violence?
3. Based on the aforementioned patterns, what domestic experiences can be drawn upon for reference?
Certainly not.
Medical violence has become a global issue; it is widespread in both developing and developed countries, regardless of living standards or levels of civilization.
Characteristics and Commonalities of Healthcare Violence Across Countries
As early as 2002–2003, the World Health Organization (WHO), in collaboration with the International Labour Organization (ILO), the International Council of Nurses (ICN), and Public Services International (PSI), conducted a study on violence against healthcare workers (referred to by the WHO as “violence in the workplace in health care settings”), using eight countries as case studies, and published a research report.
We have selected and summarized certain dimensions from the research report as follows:

Types of Violence and Perpetrators in Countries Surveyed by the World Health Organization and Other Institutions on Violence in Healthcare Settings
Source: WHO official website; graphic by VCBeat
These eight countries have different political systems, healthcare systems, economic levels, ethnicities, and religious beliefs, yet they all face the problem of medical violence, which further illustrates the widespread nature of this issue. It just presents different characteristics in different regions, and the national conditions of different countries affect the types of violent behaviors.
In other countries, the National Survey of Nurses’ Work and Health conducted in Canada showed that 34% of surveyed nurses who provided direct care services in hospitals or long-term care institutions had experienced physical assault from patients.
A survey conducted by the Liaison Conference for the Promotion of Medical Safety at Private University Hospitals in Japan revealed that in 2012, 44.3% of healthcare workers in Tokyo had experienced workplace violence, including verbal or physical abuse and sexual harassment by patients.
According to The Guardian, data released by the UK’s National Health Service (NHS) in October 2018 showed that one in seven healthcare workers in the UK experienced workplace violence in 2017, marking a five-year high. Over the course of the year, an average of 200 incidents of violence against medical staff, varying in severity, occurred daily in the UK.
Although medical violence exhibits distinct characteristics across different countries, it shares a common feature: the perpetrators, particularly those committing physical violence, are predominantly patients, with relatives and visitors also accounting for a significant proportion of incidents.
Crime and Deaths Caused by Severe Violence
The severity of violent acts varies; perpetrators may face corresponding penalties for minor offenses or criminal charges for serious ones. The consequences also range in severity, from causing physical injury or psychological trauma to healthcare workers to, in the most extreme cases, resulting in their death.
According to the 2011 national crime statistics in the United States, violence in the healthcare sector accounted for 10% of all workplace violence. Due to the U.S. gun control regulations, some incidents of healthcare-related violence have manifested in severe forms. Statistical reports published in the Annals of Emergency Medicine indicate that between 2000 and 2011, a total of 150 shootings occurred in hospitals across the United States, with approximately 30% of these incidents taking place in emergency departments.
In 2018, a U.S. cardiologist was shot and killed; the suspect’s mother had died during a surgery performed by this doctor 20 years earlier, suggesting the shooting was an act of revenge motivated by long-held resentment.
Germany Has Also Experienced Shooting Incidents Targeting Physicians. According to media reports, in July 2016, a 72-year-old patient in Berlin, Germany, shot his attending physician before taking his own life; the physician also tragically died.
Physical injuries can be treated, and psychological trauma can be healed; however, the loss of life is irreversible and represents the outcome that no one wishes to see.
The WHO report highlights that various forms of violence also have indirect impacts on the supply of medical resources, which may include a decline in healthcare quality and the exodus of healthcare professionals from the industry, ultimately leading to an overall reduction in healthcare services and increased medical costs.
Given the myriad consequences of violence against healthcare workers, implementing effective protective measures for medical personnel has become a formidable task worldwide.
Certainly not.
We have collected measures adopted by various countries to address violence against healthcare workers through multiple channels. In addition to legal frameworks, these measures include specific approaches in areas such as healthcare administration, the development of hardware and software infrastructure, and hospital management.
Top-Level Design, Strengthening Punitive Measures
Laws, enforced by state coercive power, serve as the prerequisite and foundation for implementing other measures. Many countries have enacted legislation to protect healthcare workers and impose severe penalties on acts of medical violence.
In 2019, the Russian Federation adopted amendments to Article 151 of the Code of Criminal Procedure of the Russian Federation, entitled “Protection of the Life and Health of Patients and Medical Personnel.” The Chairman of the State Duma Committee on Healthcare stated that these amendments were landmark, as they introduced the phrase “obstruction of the provision of medical services” for the first time.
In September 2019, India released a draft law stipulating that acts of violence against doctors and other healthcare professionals would be punishable by imprisonment for three to ten years and fines ranging from 20,000 to 100,000 Indian rupees. Individuals who damage medical facilities could face up to five years’ imprisonment and a fine of up to 500,000 Indian rupees.
In 2018, the United Kingdom explicitly stated that prison sentences for individuals who assault healthcare workers would be doubled. Prior to this, the UK’s amended Criminal Justice and Immigration Act 2009 had already introduced the offense of “causing nuisance within National Health Service (NHS) facilities,” and the law also granted healthcare personnel the right to use reasonable force to remove disruptive individuals.
As of 2016, 38 U.S. states had enacted specific legislation to protect healthcare workers. For example, New York State passed the “Assault on Healthcare Workers Act,” which classifies assaults on on-duty healthcare personnel as felonies; after 2010, California enacted legislation requiring hospitals to maintain adequate staffing levels for both healthcare and security personnel during shifts.
In terms of strengthening hospital management through legislation, the U.S. National Labor Relations Act and the Occupational Safety and Health Act stipulate that all employers are responsible for ensuring the safety and health of their employees. These laws require hospitals to develop measures to prevent incidents of violence against medical staff; failure to do so will result in administrative penalties. In 2011, a psychiatric hospital in Maine was fined $6,300 by the Occupational Safety and Health Administration (OSHA) after 90 incidents of patients violently attacking doctors occurred over a two-year period.
Queensland, Australia, has also enacted similar legislation, under which violent assaults on healthcare workers can result in a maximum prison sentence of 14 years.
While there are laws to abide by, law enforcement must also be strict.
In 2017, a cancer patient in California, dissatisfied with the outcomes of his treatment, left a note at home stating his intention to shoot dead the three physicians who had been treating him. When police located him, they discovered two semi-automatic handguns and a white rubber mask in his vehicle. Ultimately, prosecutors charged the patient with three felony counts, including premeditated murder.
Medical Administration: Mobilizing Multi-Stakeholder Participation
Once the law establishes a framework outlining mandatory and prohibited actions regarding medical violence, relevant healthcare authorities can formulate policies based on this foundation to mobilize multi-sectoral participation in violence governance, encompassing both the prevention of violent acts and research into such behavior.
Since 2009, U.S. hospital accreditation bodies have incorporated the management of workplace violence into their accreditation standards, thereby incentivizing healthcare institutions to refine their safety protocols.
In 2015, the French Ministry of Health issued 30 guidelines to comprehensively safeguard the security of healthcare workers through holistic regulations. These guidelines not only pertain to the newly established Committee for Improving Healthcare Worker Safety but also involve medical institutions, law enforcement agencies, and judicial authorities, thereby fully leveraging the leading role of the health sector.
Several countries have conducted specialized research on the root causes of violence and the patterns of violent behavior.
For example, the Australian Patient Safety Foundation has established an incident monitoring system to conduct statistical analysis of conflicts in healthcare settings from an epidemiological perspective. The analysis indicates that patient-related factors include mental disorders, altered consciousness, alcohol intoxication, or drug dependence.
The American Journal of Emergency Medicine has published studies indicating that patients with mental illness, a history of violence, or under the influence of drugs and alcohol are the primary perpetrators of common violence in emergency departments.
A report from the Murcia Autonomous Community in Spain noted that among healthcare-related violent incidents occurring between 2006 and April 2008, 70% of perpetrators were male, with 80% of them under the age of 40. Causes of these violent assaults included unmet healthcare needs, delays in sick leave approvals and diagnostic tests, and noncompliance with medical guidelines provided by healthcare or support staff.
Studying the characteristics and patterns of violent behavior can facilitate the more effective development of prevention mechanisms.
Hardware and Software Configuration, Dual Online and Offline Protection
With institutional frameworks established at both the legal and medical administration levels, localities have systematically improved the hardware and software infrastructure of healthcare institutions in accordance with their specific local conditions.
In terms of hardware, the primary focus is on equipping facilities with security screening and defense systems. For instance, the U.S. healthcare system has implemented security measures to strengthen hospital safety. Hospitals are required to install metal detectors and employ armed guards, with individuals undergoing security checks before entering the facility. In certain cases, even patients on stretchers are subjected to metal detector screening. Currently, many healthcare institutions in the United States have made it standard practice to establish security personnel, install additional security screening equipment, and provide emergency call buttons.
In Russia, the Kemerovo Regional Ministry of Health has equipped physicians with stun guns, which they are permitted to carry without a license. These devices serve as a means of self-defense in the event of an attack on medical personnel. Vyacheslav Vaneyev, a weapons expert, argues that, in reality, it is impossible to assign a law enforcement officer to accompany every physician. Therefore, doctors should be provided with necessary defensive weapons, as their immediate response in such situations naturally includes protecting their lives, health, and even dignity.
In terms of software, leveraging information technology to strengthen security prevention and control is a key component of infrastructure development. For instance, some hospitals in Portland, United States, have established networked databases of prior violence records, which has reduced violent incidents by 91%.
In-Hospital Management: Strengthening Protection at the Last Meter
Since medical violence occurs within healthcare institutions, regardless of the efforts made at the aforementioned levels, it cannot be separated from the internal management of these institutions. This can be described as the "last meter" of protection for medical staff, which is the protection that can take effect immediately when a violent incident occurs.
As previously mentioned, the World Health Organization (WHO) conducted a study on violence in healthcare settings, using eight countries as case studies. Based on these findings, the WHO released the Framework Guidelines for Addressing Workplace Violence in Healthcare Settings. Although these guidelines are non-binding and primarily serve as recommendations, they still provide a valuable reference for countries worldwide.
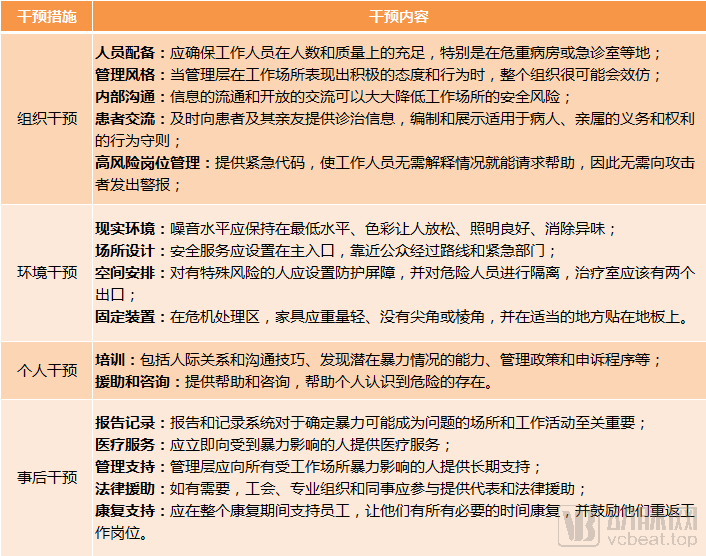
Excerpts from the WHO’s “Framework Guidelines for Addressing Violence in Health Workplaces”
Source: WHO official website; graphic by VCBeat
The Guidelines propose interventions for violence in healthcare settings across four dimensions: pre-incident organizational, environmental, and individual interventions, as well as post-incident interventions. These measures offer corresponding recommendations ranging from facility design and spatial layout in healthcare institutions, to the management and training of medical staff, and further to legal aid and rehabilitation support for those who have suffered violent injuries.
The fact that in-hospital management protocols in some countries align with those outlined in the Guidelines further demonstrates their feasibility.
For example, Australia minimizes the occurrence of medical violence in hospital design by: optimizing the clinical environment to reduce patients’ negative emotions, such as improving consultation efficiency, ensuring care quality, and shortening waiting times for admission; maintaining quietness in public waiting areas to minimize noise disturbance; and optimizing consulting room layouts to reduce the risk of attacks on healthcare workers, such as planning rapid escape routes, installing dual exits, and preventing staff from being surrounded.
In Australia, in the event of medical violence, whether it is the attacked medical staff or the staff who discovers the violent situation, they only need to call the switchboard, inform "Code Black", and report the location. If there is no time to make a phone call, immediately press the emergency button on the wall, and the security department will arrive in time.
In addition, countries such as the United States, Australia, and the United Kingdom have also developed guidelines for preventing and controlling violence against healthcare workers.
Taking the "Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers," issued by the U.S. Department of Labor’s Occupational Safety and Health Administration (OSHA) in 2004, as an example, the main contents include: management commitment and employee participation, emphasizing that hospital administrators and frontline healthcare workers must collaborate through the establishment of teams or committees; the requirement to establish threat assessment teams to conduct thorough analyses of violent incidents; safety and health training, requiring all employees to be aware of potential safety hazards and to respond effectively to violence against healthcare personnel through established procedures; and recordkeeping and evaluation processes, emphasizing the retention of documentation that reflects the factual truth to facilitate further handling of incidents and improvement of related work.
Healthcare institutions may develop corresponding management systems in accordance with this guideline.
A critical component of the guidelines is the implementation of training programs. Since law enforcement may arrive at the scene after violent acts have already ceased, even with the most rapid response to incidents of healthcare-related violence, it is imperative that hospital personnel possess the capability to manage such emergencies. Countries including the United States, the United Kingdom, and Australia have also incorporated corresponding training into the statutory obligations of hospital employers.
Training for relevant personnel in the United States includes specialized rapid-response training, programs to avoid accidental injury by law enforcement, and personal safety training, requiring management staff to learn how to identify high-risk situations. Security personnel must undergo specialized training for healthcare settings, which includes analyzing aggressive patients and various types of disruptive behaviors.
Training in Australia primarily focuses on violence prevention techniques and simulation exercises. This includes studying behavioral and psychological aspects related to violence, as well as individual coping strategies for prevention, such as self-control when facing attacks, communication skills to de-escalate tense situations, and the appropriate attitude to maintain when confronted with medical violence. Through these drills, trainees can quickly master the relevant prevention systems.
Strengthen Publicity and Promote Public Participation
Although the healthcare setting primarily involves two main parties—medical providers and patients (the latter including their relatives and visitors)—and may appear straightforward on the surface, in reality, every member of the public may become part of the patient group at different stages of life. Therefore, patients require both in-hospital and out-of-hospital interventions.
In hospitals, Australia emphasizes a zero-tolerance stance on violence and strengthens institutional deterrence by posting warning signs against hospital violence in public areas such as reception and waiting rooms. This approach aims to foster harmonious doctor-patient relationships through clear deterrence.
Internationally, there is a consensus on adopting a zero-tolerance stance toward violence against healthcare workers outside hospital settings, and this concept needs to be widely promoted. Spain has designated April 20 as the “National Day Against Violence Toward Healthcare Workers” to commemorate a family physician who was murdered by a patient in 2009. Spanish scholars believe that this observance can raise societal awareness of violence against medical personnel, encourage professionals to combat such violence, and leverage social media to create related topics that engage the general public.
"Through in-hospital and out-of-hospital education and publicity, raising public awareness may nip some potential medical violence in the bud."
Given the significant differences in healthcare systems, economic environments, and cultural backgrounds, it is difficult to claim that the practices of any single country can be simply replicated and directly applied. By synthesizing the measures adopted by the aforementioned countries and drawing on their transferable insights or commonalities, we believe that addressing medical violence is a systemic endeavor that cannot rely solely on legislation or hospital management.
Thus, we summarize a “pyramid” governance model that proceeds top-down, from top-level design to public participation, with the aim of providing reference for healthcare management in China.
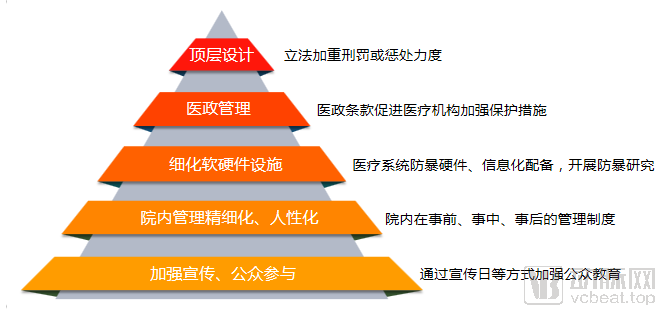
“Pyramid” Model of Measures to Prevent and Control Medical Violence in Various Countries, Chart by VCBeat
The “Pyramid” model consists of five tiers. At the top, legislative bodies are tasked with refining the legal framework and imposing stricter penalties for acts of medical violence. Next, healthcare regulatory authorities should strengthen administrative oversight, formulate relevant policy provisions, and encourage more active participation from medical institutions, research organizations, and non-governmental entities in violence prevention and control. Following this, regions should equip themselves with appropriate hardware and software infrastructure for violence prevention, tailored to local conditions. At the hospital level, specific measures must be implemented regarding spatial layout, management protocols, and post-incident intervention. Finally, it is crucial to enhance public awareness and foster a zero-tolerance attitude toward medical violence through robust publicity campaigns.
Specifically, across five dimensions and in light of the current situation in China, we identify the following key points:
1. Legislative aspects. Recently, China’s first foundational and comprehensive law in the field of health and healthcare, the Basic Healthcare and Health Promotion Law, has been enacted. It explicitly stipulates that the personal safety and human dignity of healthcare professionals shall be inviolable, and their legitimate rights and interests are protected by law. Any organization or individual is prohibited from threatening or endangering the personal safety of healthcare professionals or infringing upon their human dignity. The state shall take measures to safeguard the practice environment for healthcare professionals.
The Basic Healthcare and Health Promotion Law also explicitly designates medical institutions as “public places.” The legal community holds that codifying hospitals as public places means they are no longer classified as internal security units under the Regulations on Internal Security Protection of Enterprises and Public Institutions. Consequently, the applicable laws for corresponding incidents may differ, potentially leading to variations in the severity of penalties or sentencing.
If acts of medical violence are suspected of constituting crimes, the relevant provisions of the Criminal Law shall also apply. Therefore, from a legal perspective, there is already a statutory basis in place; what remains essential in practice is the strict enforcement of the law.
2. Medical Administration Management. Collaborate with public security and other departments to establish more comprehensive emergency response mechanisms, and take the lead in liaising with universities and research institutions to strengthen research on violence prevention and control, thereby providing better reference for emergency response mechanisms.
3. Regarding hardware and software facilities. Whether hospitals should uniformly install metal detectors is debatable, particularly in the emergency department, where every second of resuscitation can be critical to a patient’s life. If this procedure delays routine medical care, the drawbacks would outweigh the benefits; therefore, decisions should be based on the specific circumstances of each hospital. Additionally, whether physicians should be equipped with self-defense weapons such as tasers is also questionable, as improper use could inadvertently turn these devices into tools for assailants to harm others.
However, on the software side, consideration could be given to establishing a database akin to a “prior record of medical violence” archive, and companies might even explore providing digital solutions for the prevention and control of violence in hospitals.
4. In-hospital management. Reasonably establish escape routes for physicians and install accessible alarm devices; rationally allocate existing medical resources and optimize the healthcare environment; conduct training and drills to enhance the emergency response capabilities of medical staff in the face of unexpected incidents; following any violent incident, both administrators and healthcare professionals must uphold a firm stance of zero tolerance toward violence.
5. Public Education. Posting relevant slogans within hospital premises serves as a deterrent, and this low-cost approach is entirely feasible; existing legal provisions can be printed on these materials. For external publicity, while it may not be necessary to establish a “National Day Against Violence Toward Medical Personnel,” we currently have Chinese Doctors’ Day on August 19 and International Nurses Day on May 12. In the past, these days attracted attention primarily from healthcare professionals, with discussions focusing largely on the hardships and dedication of medical staff. Going forward, these occasions should be leveraged to intensify campaigns promoting zero tolerance for violence against healthcare workers, using public service advertisements and promotional videos in public spaces and on social media platforms.
In the face of violence that has already occurred, we may not be able to take direct action, nor do we wish to cause further harm through emotional reactions. However, we can contribute our modest efforts through the aforementioned words and ideas, striving to make the world a better place.
References:
Feng Lei, Conflict and Governance: A Study on the Manifestations of Medical Violence in China and Governance Strategies, Science Press
Si Ling, Zhang Xue, et al., “Countermeasures and Implications for Hospital Violence Prevention in Australia,” Chinese Health Quality Management, Vol. 23, No. 6
Jiang Kaiming, Zhao Min. Research on the Phenomenon of Violence Against Medical Personnel Abroad and Prevention and Control Strategies. Medicine & Philosophy, November 2018, Vol. 39, No. 11A
Li Wei, Zhang Xue, et al., “Research on Hospital Violence in the United States and Its Implications for China,” Medicine & Philosophy, November 2014, Vol. 35, No. 11B
“How to Curb Violence Against Medical Staff? These Countries Have Tough Measures to Tackle ‘Medical Disturbances’,” The Beijing News International Affairs