Trends in Hot Biomarkers for Precision Immuno-Oncology Diagnostics
Around 2500 BC, the ancient Egyptian physician Imhotep recorded a patient’s symptoms in his medical notes: a bulging mass on the breast, hard and cold to the touch, dense like a hemangium, spreading beneath the skin. Although Imhotep was a renowned physician who provided detailed treatment protocols for various conditions in his manuscripts, he wrote only a single, brief line for this case of cancer: “There is no treatment.” This constitutes the earliest known historical record of breast cancer.
For thousands of years, cancer has been the greatest threat to human life and health. According to statistics from the 2017 Annual Report on Cancer Registration in China, approximately 10,000 people are diagnosed with cancer each year in China, averaging seven new cases per minute.
Immuno-Oncology Therapy (I-O) first emerged in the late 19th century. After more than 130 years of extensive exploration, it has finally come to be regarded as the most promising approach to conquering cancer. In September 2014, nivolumab, the world’s first PD-1 antibody drug, was launched in Japan, increasing the five-year survival rate for advanced non-small cell lung cancer from less than 5% to 16%.
Tumor immunotherapy refers to a therapeutic approach that achieves the killing of tumor cells by activating the body’s immune system. Its fundamental strategy involves activating the host’s own immune system—by relieving immunosuppression in the tumor microenvironment, enhancing the antigen-presenting function of antigen-presenting cells, and promoting the generation of T lymphocytes—thereby enabling the recognition and destruction of cancer cells.
The second decade of the 21st century witnessed the most rapid development in immunotherapy, with novel oncology treatment modalities such as immune checkpoint inhibitors targeting PD-1 and CAR-T cell therapy successfully translating from research achievements to clinical applications. Since 2014, a total of nine PD-1/PD-L1 drugs have been approved for marketing worldwide. According to data from Evaluate Pharma, the global market size for cancer immunotherapy reached $61.9 billion in 2016 and is projected to grow to $120 billion by 2021.
In China, immunotherapy demonstrates equally explosive growth. According to data from Menet, the market size of anti-tumor monoclonal antibodies at public medical institutions in China exceeded RMB 10 billion for the first time in 2018, with a growth rate of 41.36%, the highest among the nine subcategories of anti-tumor drugs. Since 2018, multiple new anti-tumor monoclonal antibody products, including toripalimab injection, sintilimab injection, and camrelizumab for injection, have been approved for marketing. Additionally, more than 20 PD-1 inhibitors are currently undergoing clinical trials in China.
Amid the fervor surrounding tumor immunotherapy, from R&D to clinical application, fiercely competitive market dynamics have become inevitable. At present, expanding indications and reducing prices are standard strategies employed by oncology immunotherapy manufacturers to capture market share. For instance, since its initial approval for the treatment of melanoma, pembrolizumab has expanded to cover more than 23 indications across 15 cancer types. Similarly, the six PD-1/PD-L1 monoclonal antibody drugs that have been successively launched in China exhibit a clear downward trend in pricing.
However, despite the intensifying market competition and the significant successes achieved by immunotherapy in oncology treatment, it is an undeniable fact that patient response rates remain consistently low across various types of immunotherapies.
As a critical component of personalized precision medicine, tumor immunotherapy employs omics data to identify the most suitable potential patients, thereby optimizing clinical outcomes; this approach represents the mainstream strategy for enhancing drug response rates. The FDA categorizes diagnostic methods used to assess the efficacy of immunotherapies into two types: “companion diagnostics” and “supplementary diagnostics.”
Companion diagnostics are mandatory tests for patients receiving corresponding drug therapies, providing essential information on the safety and efficacy of therapeutic products. The advantage of companion diagnostics lies in their ability to strictly stratify patients into two groups—biomarker-positive and biomarker-negative—based on predefined cut-off values. Only biomarker-positive patients are eligible for treatment, thereby ensuring that patients achieve maximal clinical benefit while maintaining medication safety. In contrast, complementary diagnostics are not mandatory for patients receiving corresponding drug therapies but can provide information relevant to individualized treatment, assisting physicians or patients in decision-making.
As immunotherapy becomes increasingly prevalent in clinical practice, precision immuno-oncology companion diagnostics have emerged as a new strategic battleground for providers of tumor-related genetic testing services. Currently, the FDA has approved biomarkers such as PD-L1 positivity and microsatellite instability-high (MSI-H) status to guide the clinical use of PD-1/PD-L1 inhibitors.
Identifying and appropriately configuring tumor immune diagnostic biomarkers is key to precision immuno-oncology diagnostics. Currently, genomic testing service providers primarily offer assays focused on popular biomarkers such as PD-L1 expression levels (TPS/CPS), MMR/MSI status, and TMB. They design different sequencing panels based on factors including indications, the tumor microenvironment, and clinical evidence.
PD-L1 Expression
PD-L1 expression is currently one of the three major predictive biomarkers used to determine whether patients with various solid tumors are suitable for treatment with PD-1/PD-L1 inhibitors. The primary clinical detection method is immunohistochemistry (IHC). Higher levels of PD-L1 expression suggest that the tumor is more likely to achieve immune escape through the PD-1/PD-L1 signaling pathway rather than other pathways. Early studies have shown that as PD-L1 expression increases, the efficacy of PD-1/PD-L1 inhibitors improves, disease control duration is prolonged, and patient prognosis is enhanced.
In May 2017, Roche’s oncology assay VENTANA PD-L1 (SP263) received FDA approval for market launch. This assay was initially used to guide treatment with AstraZeneca’s durvalumab in patients with locally advanced or metastatic urothelial carcinoma, providing information on tumor programmed death-ligand 1 (PD-L1) expression status. One year later, Agilent Technologies’ Dako PD-L1 IHC 22C3 pharmDx kit received FDA approval as a companion diagnostic for pembrolizumab in the treatment of cervical cancer.
Currently, there are five PD-L1 immunohistochemistry (IHC) assay kits: 22C3, 28-8, SP263, SP142, and 73-10. These five IHC antibodies are tested on two IHC platforms, DAKO and Ventana. Results from the Blueprint Project demonstrate that the 22C3, 28-8, and SP263 assays show concordant staining for tumor cells, whereas the SP142 assay detects fewer positive cells. Therefore, the 22C3 antibody exhibits generalizability in evaluating other immunotherapeutic agents.
The International Association for the Study of Lung Cancer compared multiple PD-L1 testing kits and found that the DAKO 22C3 assay kit outperformed other products in detection rate, accuracy, and overall reliability.
However, despite the many advantages of PD-L1 expression, it is not a truly reliable predictor of immunotherapy efficacy. While clinical evidence supports the utility of PD-L1 expression, it also provides contradictory findings. There are cases across different cancer types where patients with no PD-L1 expression still respond effectively to immune checkpoint inhibitors. For instance, in renal cell carcinoma, PD-L1 expression lacks predictive value. Furthermore, the predictive capability of PD-L1 expression is somewhat correlated with patients’ smoking history. The reliability of PD-L1 expression as a predictive biomarker varies depending on factors such as the underlying mechanism of PD-L1 expression, detection methods, threshold determination, and evaluation criteria.
MMR and MSI
MMR (Mismatch Repair), or mismatch repair, is a post-replicative DNA repair mechanism that maintains the fidelity of DNA replication and controls genetic mutations. MSI (Microsatellite Instability), or microsatellite instability, refers to any alteration in the length of a microsatellite in tumor tissue compared to normal tissue, caused by the insertion or deletion of repeat units, resulting in the emergence of new microsatellite alleles. It represents the level of tumor genomic mutations and indirectly reflects tumor immunogenicity.
In 2015, The New England Journal of Medicine published a study led by the team of Dr. Luis Diaz and Dr. Bert Vogelstein at Johns Hopkins University. The study demonstrated that immune checkpoint inhibitors are effective in a subset of patients with colorectal cancer.
In this study, researchers enrolled 41 patients with colorectal cancer, comprising those with deficient mismatch repair (dMMR) and proficient mismatch repair (pMMR), as well as patients with dMMR tumors of other histologies. All patients received pembrolizumab treatment every two weeks. The results demonstrated that, compared with pMMR colorectal cancer patients, dMMR patients exhibited longer progression-free survival (PFS) and overall survival (OS), as well as a higher response rate to treatment.
In May 2017, the FDA granted accelerated approval to the PD-1 inhibitor pembrolizumab (Keytruda) for the treatment of adult and pediatric patients with unresectable or metastatic solid tumors harboring the microsatellite instability-high (MSI-H) molecular signature—the first anticancer therapy approved by the FDA based on biomarker status rather than tumor origin.
On August 1 of the same year, the FDA granted accelerated approval to nivolumab for patients with colorectal cancer exhibiting high microsatellite instability (MSI-H) or deficient mismatch repair (dMMR). These two examples clearly demonstrate the critical role of MMR and MSI in tumor prediction.
However, the prevalence of MSI-H varies significantly across different cancer types. It reaches approximately 25% in endometrial and gastrointestinal cancers, whereas it is less than 5% in lung cancer and other malignancies. Furthermore, analysis of data from 100,000 cancer patients reveals that the vast majority (83%) of MSI-H cases fall within the TMB-H category. Notably, many patients with microsatellite-stable (MSS) tumors also respond well to immunotherapy. Therefore, relying solely on this biomarker would exclude a substantial number of patients who could benefit from such treatments.
TMB
Tumor Mutational Burden (TMB) refers to the number of detected gene mutations per million bases. The number of somatic mutations in different cancers ranges from 0.01 mutations/Mb to over 400 mutations/Mb, and some of these mutations can be transcribed and expressed as peptide antigen epitopes or tumor neoantigens.
Theoretically, cancer patients with a higher burden of gene mutations generate more neoantigens, making their cancer cells more distinct from normal cells. This increases the likelihood of recognition by immune cells and enhances the potential for therapeutic benefit.
In 2014, scientists analyzed whole-exome sequencing (WES) data from patients treated with CTLA-4 antibodies and discovered a correlation between tumor mutational burden (TMB) and treatment efficacy, marking the first application of TMB in immunotherapy. In 2015, researchers again used WES to analyze lung cancer patients treated with PD-1 antibodies, finding that high TMB was positively correlated with clinical outcomes; these results were published in the prestigious journal Science. In 2016, a retrospective analysis of WES data from the CheckMate 026 clinical trial revealed that patients with high TMB who received PD-1 inhibitor therapy achieved significantly greater clinical benefit compared to those receiving chemotherapy. Consequently, TMB began to attract worldwide attention.
TMB truly began to gain prominence following the advent of multi-gene panel sequencing. Early TMB studies employed whole-exome sequencing (WES), which was cost-prohibitive, prompting efforts to replace WES with panel-based sequencing. In 2018, prospective study data on panel-based TMB assessment were released; both CheckMate 227 and CheckMate 568 demonstrated that patients with advanced non-small cell lung cancer (NSCLC) and a TMB ≥10 mutations/Mb derived greater benefit from immunotherapy.
Subsequently, the European Society for Medical Oncology (ESMO) and the National Comprehensive Cancer Network (NCCN) incorporated tumor mutational burden (TMB) as a potential biomarker into their respective guidelines, based on data from the CheckMate 227 and CheckMate 568 trials. This development sparked a surge in the development of panel-based testing products by genetic testing companies, including numerous domestic firms in China.
However, TMB, which had been surging ahead, has recently encountered a setback.
First, the survival outcomes of Bristol Myers Squibb’s (BMS) nivolumab in combination with ipilimumab (Yervoy) were found to be independent of tumor mutational burden (TMB). In recent years, BMS has actively explored molecular biomarkers including PD-L1, TMB, MSI, and TILs. However, in March 2019, new clinical trial data demonstrated no difference in survival outcomes between patients with high or low tumor TMB levels. Following discussions with the U.S. Food and Drug Administration (FDA), BMS withdrew its supplemental Biologics License Application.
Almost simultaneously, Merck & Co., which is highly experienced in the clinical application of biomarkers, also encountered setbacks after incorporating tumor mutational burden (TMB) as a biomarker into multiple clinical trials. Furthermore, at the 2019 ESMO Congress, which concluded in early October, Professor Corey Jay Langer from the United States announced that in the KEYNOTE-021 trial, TMB was not associated with survival outcomes in patients treated with pembrolizumab in combination with chemotherapy.
In fact, TMB is an investigational biomarker for which no industry standards or consensus have yet been established. There is a lack of standardization in panel design, algorithms, and cut-off values for classifying TMB as high or low. Consequently, TMB results generated by different testing laboratories across various clinical trials are not comparable. Clinical application must be based on evidence from clinical performance validation and prospective studies.
Sequencing studies centered on a single biomarker to predict the efficacy of immunotherapy represent a common design paradigm for mainstream biomarker products. Admittedly, continuously iterated single-biomarker sequencing products can, to some extent, stratify patients who are likely to benefit; however, regardless of the biomarker employed, they suffer from high false-positive and false-negative rates. In other words, current methods for predicting immunotherapy response face a dilemma wherein selected patients with high biomarker levels fail to respond to immunotherapy, while some patients with low biomarker levels exhibit a favorable response.
Therefore, researchers have increasingly focused on patient stratification using multiple biomarkers.
Researchers have found that previously underappreciated metrics, such as loss of heterozygosity in human leukocyte antigens (HLA-LOH) and tumor neoantigen burden (TNB), can serve as adjuncts to the aforementioned mainstream indicators, further enhancing the specificity of efficacy prediction. VCBeat interviewed industry experts on the predictive mechanisms underlying these less-common biomarkers.
In fact, while the principle of TNB in predicting tumor immune response shares similarities with TMB, there are fundamental differences. Within the tumor microenvironment, gene mutations undergo transcription and translation, ultimately being presented as peptide fragments on the cell surface by MHC molecules. T cells identify tumors by recognizing tumor-specific peptides. These specific peptides are also known as tumor neoantigens; the higher the number of tumor mutations, the greater the probability of generating neoantigens, thereby increasing the likelihood of triggering a T cell-mediated immune response.
“Currently, TMB is used to quantify tumor mutations, with the corresponding metric for neoantigen quantification being TNB, defined as the number of neoantigens detected per million bases in the coding region of the tumor genome,” an industry insider explained to VCBeat. “Therefore, it can be said that TMB indirectly reflects tumor immunogenicity, whereas TNB directly reflects tumor immunogenicity.”
However, the process from gene mutation to neoantigen generation involves a series of complex steps. “High tumor mutational burden (TMB-H) does not necessarily correlate with high tumor neoantigen burden (TNB-H),” emphasized the expert. Real-world study data indicate that there are clinically observed patients with TMB-H but low tumor neoantigen burden (TNB-L), and these patients are unlikely to respond to immunotherapy. Therefore, using a dual-parameter model combining TMB and TNB for assessment can improve predictive accuracy.
Interestingly, another biomarker, HLA, which predicts immunotherapy response rates, also correlates with the tumor neoantigen burden (TNB) status in specific patients. HLA refers to protein molecules located on the surface of antigen-presenting cells that are responsible for antigen presentation. The number of HLA alleles is exceptionally large, with 17,331 identified to date. Each HLA allele can exhibit different affinities for presenting the same neoantigen. Loss of heterozygosity in HLA leads to impaired immune surveillance mediated by neoantigen recognition, thereby facilitating immune escape of mutant tumor clones and resulting in a high tumor mutational burden (TMB).
The accuracy of HLA as a biomarker for predicting immune response rates is also strongly correlated with the levels of other biomarkers in the tumor microenvironment. At the ASCO conference, which concluded in September 2019, researchers reported that loss of heterozygosity (LOH) in HLA class I genes is a potential factor contributing to resistance to PD-1/PD-L1 inhibitors among Chinese cancer patients with high tumor mutational burden (TMB-H). Therefore, relying solely on germline HLA typing in patients overlooks the actual status of HLA in tumor cells and fails to accurately guide immunotherapy. Concurrent detection of TMB and HLA LOH in tumor cells can more effectively identify patients who are likely to benefit from immunotherapy.
Immunotherapy has emerged as a focal point in oncology research in recent years, with PD-1/PD-L1 checkpoint inhibitors achieving remarkable success in cancer treatment. To maximize the benefits for more patients receiving PD-1/PD-L1 inhibitor therapy, it is imperative to identify effective predictive biomarkers without delay.
Based on current results, it appears difficult to rely on a single biomarker to predict the efficacy of immunotherapy. In fact, whether considering mainstream markers such as PD-L1, MMR, and TMB, or those currently receiving less attention, such as HLA and TNB, their underlying principles for predicting immune response are interrelated. Therefore, improving the accuracy of immune response prediction by integrating different biomarkers and designing well-structured large-panel testing products seems to be an inevitable path forward.
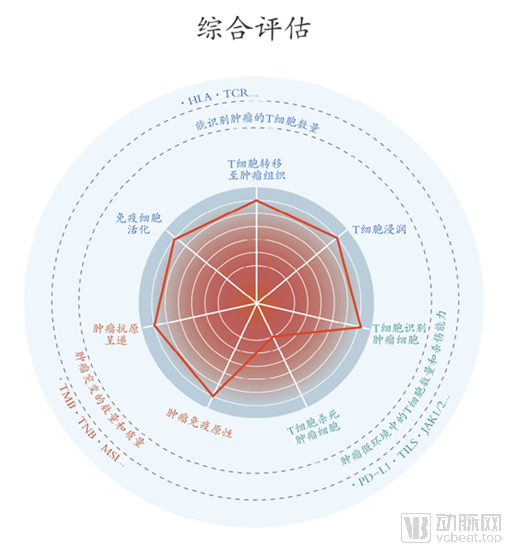
In future studies, constructing appropriate predictive models based on population-level drug efficacy data and incorporating multidimensional test results (including but not limited to gene sequencing, immunohistochemistry, and proteomics data) may be key to predicting the efficacy of immunotherapy. Such models would comprehensively evaluate indicators such as drug target genes, tumor mutational burden (TMB), tumor neoantigen burden (TNB), HLA typing and loss of heterozygosity, immune pathway genes, immune resistance genes, and genes associated with hyperprogressive disease following immunotherapy. We look forward to the day when this goal is achieved sooner through the joint efforts of researchers worldwide in relevant fields, thereby bringing greater benefits to all humanity from cancer immunotherapy.