HeartFlow: Revolutionizing Cardiovascular Diagnosis with Non-Invasive FFR Technology and $1.5B Valuation

HeartFlow
Developer of Cardiovascular Diagnostic Medical Software
Throughout the long history of medical development, there exists a distinct category of physicians whose achievements extend beyond healing patients with their own hands. By innovating diagnostic and therapeutic approaches, they have revolutionized the clinical practices of physicians worldwide, thereby benefiting a broader patient population. A prime example is the German surgeon Kurt Semm, who pioneered minimally invasive surgery.
Christopher K. Zarins, a co-founder of the startup HeartFlow featured in this article, is also such a physician. As a doctor, he served as Chief of Cardiovascular Surgery at the University of Chicago Medical Center, one of the top 10 medical schools in the United States, for 17 years.
In 1993, he delivered a lecture at Stanford University on the theme of blood flow velocity and cardiac health. The audience consisted not of medical students, but of a group of young engineers from Stanford. These engineers frequently applied their expertise to research in aerospace, astronomy, transportation, and other fields. This lecture created an opportunity to integrate engineering with the diagnosis of cardiovascular disease.
Ten years later, Charles Taylor, a young engineer in the audience at the time, co-founded HeartFlow with Christopher K. Zarins in 2007. An idea sparked by that presentation has now grown into a unicorn valued at $1.5 billion.
To date, HeartFlow has raised a total of $467 million from investors including GE Ventures, Wellington Management, and BlueCross BlueShield Ventures. Its products are already in use in the United States, Japan, Canada, and other regions, with 40,000 patients worldwide having utilized HeartFlow’s CT-FFR solution.
In 2018, five medical device companies worldwide secured over $100 million in financing: PROCEPT BioRobotics raised $118 million; HeartFlow raised $150 million; Outset Medical raised $132 million; Butterfly Network raised $250 million; and Auris Health raised $220 million before being acquired by Johnson & Johnson for $3.4 billion.
Among them, PROCEPT and AURIS are surgical robot manufacturers, Butterfly focuses on handheld ultrasound, and Outset manufactures compact home dialysis machines. Unlike the aforementioned hardware manufacturers, HeartFlow is the only software-based diagnostic company in the group.
How Did HeartFlow Come into Being? What Are Its Future Development Directions? VCBeat (WeChat ID: vcbeat) conducted an analysis and investigation of HeartFlow, summarizing the following key information:
1. HeartFlow leverages technologies such as computational fluid dynamics, engineering, and artificial intelligence deep learning to simulate cardiac pressure and blood flow velocity based on static CT imaging data, thereby calculating the fractional flow reserve (FFR) and reducing unnecessary invasive examinations.
2. CT-FFR also has its limitations in practical application; furthermore, HeartFlow’s PCI procedure planning product has received FDA approval.
3. In terms of business model, HeartFlow adopts a cloud-based approach, where hospitals upload data to the cloud for professional computation by engineers. HeartFlow’s CT-FFR product is currently covered by the U.S. Centers for Medicare & Medicaid Services (CMS) and most commercial insurers.
Regarding artificial intelligence, there is a prevailing view that AI will ultimately replace humans. In reality, however, the adversary of AI is not humanity, but rather the unresolved challenges faced by humans. With its CT-FFR product, HeartFlow’s engineers have leveraged proprietary algorithms to replace expensive consumables, sparing patients from unnecessary invasive diagnostic procedures and reducing unwarranted interventional surgeries.
Cardiovascular and cerebrovascular diseases are the leading cause of death in humans. According to World Health Organization statistics, up to 15 million people worldwide die from cardiovascular and cerebrovascular diseases each year.
The primary clinical application of CT-FFR is in the management of chronic and stable atherosclerosis, which is highly prevalent in cerebrovascular and cardiovascular diseases. For many years, interventional therapy for this condition has been guided by imaging and morphological assessments. However, reliance solely on imaging and morphology has inherent limitations, as it cannot determine whether functionally significant ischemia is present. In recent years, continuous advancements in functional assessment, particularly the establishment of FFR standards, have addressed these shortcomings.
In the traditional diagnostic and treatment workflow, patients with chronic stable cardiovascular disease can undergo electrocardiography, echocardiography, PET-CT, and CTA upon hospital arrival to determine whether coronary angiography is indicated.
Coronary CTA visualizes the course and degree of stenosis of blood vessels through CT angiography and computer-based 3D reconstruction.
Coronary angiography, invented by Dr. Sones at the Cleveland Clinic in the United States, involves puncturing the radial artery at the wrist to advance a guidewire into the coronary arteries. A contrast agent is then injected to visually assess its filling pattern within the various coronary vessels. Filling defects indicate stenosis caused by atherosclerotic plaques. Based on the degree of stenosis, physicians determine whether stent implantation is necessary to dilate the vessel. Currently, the diagnostic criterion for coronary heart disease is a luminal stenosis of ≥50% as demonstrated by coronary angiography.
Assessing the presence of stenosis in patients through imaging modalities has certain limitations. Anatomical stenosis observed on imaging does not necessarily correspond to functional ischemia. This discrepancy is not limited to borderline lesions; even cases with severe stenosis on imaging may not exhibit functional ischemia. In such patients, revascularization can be deferred, and optimal medical therapy alone may achieve satisfactory outcomes.
For instance, among patients diagnosed with 50%–70% coronary artery stenosis via coronary angiography, percutaneous coronary intervention would constitute overtreatment in two-thirds of cases, whereas exclusive medical therapy might cause one-third of patients to miss the opportunity for beneficial intervention.
Fractional Flow Reserve (FFR) was introduced in the 1990s. FFR is defined as the ratio of the maximum blood flow achievable in the myocardial territory supplied by a coronary artery with stenosis to the theoretical maximum blood flow that would be achievable in the same territory under normal conditions.
Unlike coronary angiography, which only visualizes the degree of luminal stenosis, fractional flow reserve (FFR) can assess the actual impact of stenosis on distal blood flow. Furthermore, FFR accurately evaluates the relationship between coronary lesions and myocardial ischemia, thereby guiding rational treatment decisions and improving patient prognosis.
However, prior to the advent of CT-FFR, FFR measurement relied on expensive pressure guidewires, which were not only invasive but also costly.
HeartFlow’s technology leverages computational fluid dynamics and deep learning to calculate FFR values from CTA images, using algorithms to replace invasive pressure wires. CT-FFR offers a streamlined workflow, reducing unnecessary invasive tests and radiation exposure.
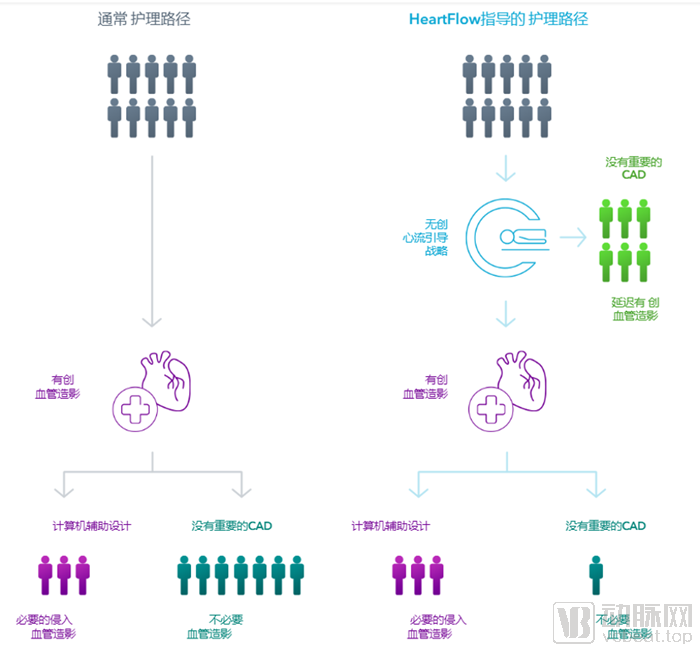
Impact of CT-FFR on Changes in the Diagnostic and Treatment Workflow
From a technical perspective, it is reported that HeartFlow’s computational method relies on finite element analysis. According to the instructions for use in its FDA clearance documentation, HeartFlow CT-FFR is a post-processing software designed for clinical quantitative and qualitative analysis. After acquiring CT DICOM data from patients with chronic coronary artery disease, the software calculates FFR values. The FFR calculation is derived through mathematical modeling, simulating blood flow pressure and velocity within a three-dimensional computer model reconstructed from static CT image data, thereby determining the FFR value.
In terms of duration, the HeartFlow computation process takes several hours before physicians can receive the analysis. HeartFlow’s product is available on both desktop and mobile devices.
However, it is worth noting that CT-FFR also has its limitations. HeartFlow’s CT-FFR analysis is not applicable to patients with suspected acute coronary syndrome or complex congenital heart disease, those who have previously undergone coronary artery bypass grafting (CABG), or individuals with a body mass index (BMI) >30.
Secondly, for patients with coronary artery metal stents, implanted pacemakers and artificial valves, severe arrhythmia, or excessive coronary artery calcification, their physical conditions can affect the quality of CT data acquisition, directly impacting the validity and accuracy of HeartFlow CT-FFR analysis.
Although HeartFlow’s first product was CT-FFR, the company has since expanded its cardiovascular imaging portfolio and developed another major product, the HeartFlow Planner.
CT-FFR is already well-established, while the HeartFlow Planner enables physicians to perform real-time virtual modeling. Using virtual models, physicians can explore multiple clinical scenarios for vascular interventions one by one, review and modify treatment plans before entering the catheterization laboratory, thereby serving as a tool for planning percutaneous coronary intervention (PCI) procedures.
First, physicians can use the planner to annotate cardiovascular stenosis. For regions requiring surgical intervention, physicians can assess whether modifying the degree of stenosis in the modeled vessels would impact blood flow.
On September 13, 2019, HeartFlow’s surgical planning product also received FDA approval.
From a business model perspective, HeartFlow’s approach involves hospitals uploading data to the cloud, where it is processed using algorithmic software combined with extensive clinical expertise.
Currently, it is being used in more than 200 institutions across the United States, the United Kingdom, Europe, Canada, and Japan, and has been applied to 40,000 patients to date.
Both CTA and HeartFlow Analysis (the two steps of the CT-Flow pathway) are commercially available. It is reported that the Centers for Medicare & Medicaid Services (CMS) and most major commercial insurers have included HeartFlow Analysis in their insurance reimbursement coverage.
Statistical data from the HeartFlow official website shows that HeartFlow Analysis reduces unnecessary angiograms and invasive procedures by 83%.
HeartFlow stated that hospitals incorporating HeartFlow into their care and diagnostic strategies reduced the total healthcare system cost per patient by more than $4,000 after one year. The average annual cost per patient under conventional care strategies was $12,145, compared with $8,127 for the HeartFlow-guided strategy. After accounting for the $1,500 cost of HeartFlow analysis, this represented a 26% reduction in costs.
HeartFlow’s founding story can be described as a perfect example of how technology can effectively enhance quality of life and longevity. However, the emergence of this technology was largely serendipitous. It was the encounter between an engineer and a senior chief of vascular surgery that gave rise to this innovative technology.
In 1993, Charles Taylor, the founder of HeartFlow, was pursuing his Ph.D. in Engineering at Stanford University. He attended a lecture delivered by Christopher K. Zarins, then Chief of Vascular Surgery and later co-founder of HeartFlow. Upon hearing Dr. Zarins discuss the relationship between blood flow and cardiac health, the young engineer suddenly realized that the computational modeling techniques he had been researching for several years could be applied to quantify arterial blood flow in patients.
With this bold idea, Charles Taylor completed his doctoral research alongside Chris and Tom Hughes, professors of mechanical engineering at Stanford University. The research focused on computational modeling of arterial blood flow and marked the first application of blood flow simulations to medical imaging data in arteries.
Charles Taylor later became a professor at Stanford University, where he continued his research on computer simulation technology. It was not until 2007 that he co-founded HeartFlow with Professor Christopher K. Zarins. From then on, the company’s journey proceeded smoothly.
In 2011, HeartFlow obtained CE certification and began sales in Europe;
In 2014, HeartFlow’s CT-FFR product received FDA de novo 510(k) clearance for marketing in the United States.
In 2015, it was marketed in Canada and secured 150 patents worldwide. The following year, it entered the Japanese market.
In 2017, a partnership with Siemens was announced.
In 2019, HeartFlow Planner received FDA approval.
HeartFlow’s success has also spurred the development of a large number of startups focused on CT-FFR, and a cohort of companies specializing in CT-FFR has emerged in China. On January 15, 2020, a CT-FFR product was approved in China. How this market will evolve in the future remains to be seen.