Global Liver Cancer Innovative Therapeutics Landscape: Insights Report
Liver Cancer, also known as primary liver cancer, is a relatively rare but highly fatal malignancy. Like other cancers, it originates from uncontrolled cell growth that subsequently invades the space of normal cells.
The liver is primarily composed of hepatocytes, but also includes cells arranged along the hepatic vasculature and biliary epithelial cells within the bile ducts. Different cell types in the liver can give rise to various benign and malignant tumors, which differ in etiology, treatment strategies, and prognostic assessment.
The incidence of liver cancer has been rising since the mid-1970s, and this upward trend is projected to continue at least until 2030. The global incidence of liver cancer is also on the rise. A study published in JAMA Oncology in December 2017 indicated that the global incidence of liver cancer increased by 75% between 1990 and 2015. Among all regions, sub-Saharan Africa and Southeast Asia had the highest incidence rates, while Mongolia’s incidence rate far exceeded that of any other country.
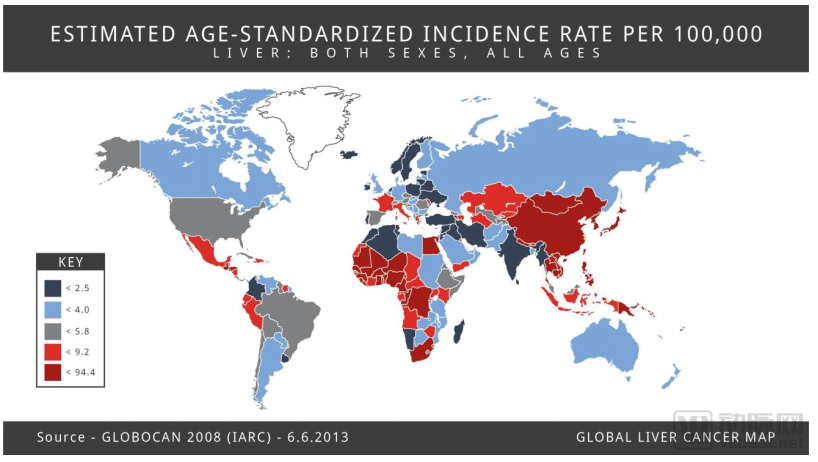
Global Distribution of Liver Cancer
According to estimates by the American Cancer Society, there were approximately 42,810 new cases of primary liver cancer and intrahepatic bile duct cancer diagnosed in the United States as of 2020 (30,170 in men and 12,640 in women). Worldwide, more than 800,000 people are diagnosed with liver cancer each year. In most regions globally, the incidence and mortality rates of liver cancer in men are two to three times higher than those in women. Liver cancer ranks fifth in terms of global case numbers, while it ranks second as the leading cause of cancer-related deaths among men.
Currently, liver cancer is the leading cause of the increase in cancer-related deaths in the United States. According to estimates by the American Cancer Society, approximately 30,160 people (20,020 men and 10,140 women) will die from primary liver cancer and intrahepatic bile duct cancer by 2020. Globally, liver cancer was the sixth most commonly diagnosed cancer and the fourth leading cause of cancer death in 2018, with approximately 841,000 new cases and 782,000 deaths annually.
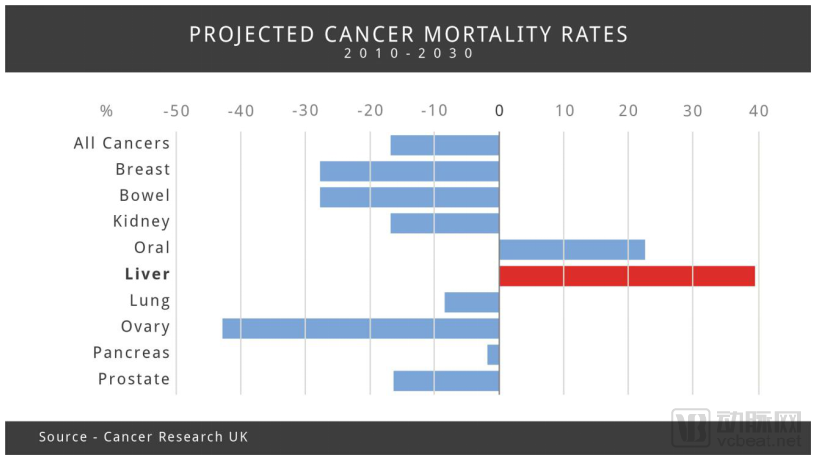
Mortality Rates by Cancer Type
This report aims to provide an overview of liver cancer and explore current therapies for patients with liver cancer and their caregivers, drugs under development, and future treatment prospects.
Liver cancer can be classified into two types. One is primary, meaning the cancer cells originate in the liver itself; the other is metastatic (secondary), meaning the cancer cells have spread to the liver from other parts of the body.
Primary liver cancer can be classified into the following types, depending on the specific cell type that undergoes malignant transformation.
· Hepatocellular carcinoma: The most common form of liver cancer in adults. Hepatocellular carcinoma can exhibit different growth patterns; some begin as a single tumor that gradually enlarges and spreads to other parts of the liver only in the late stages of the disease. Another form begins with multiple small cancerous nodules appearing in the liver, rather than a single tumor, which is also the most common presentation of hepatocellular carcinoma in the United States.
· Intrahepatic Cholangiocarcinoma (Bile Duct Cancer): Approximately 10% to 20% of cancers originating in the liver itself are intrahepatic cholangiocarcinomas, which arise from the cells lining the small bile ducts within the liver.
· Angiosarcoma: A rare form of cancer. It originates in the cells lining the blood vessels of the liver. Because these tumors grow rapidly and are often widely disseminated, they are typically difficult to remove surgically at the time of diagnosis. Chemotherapy and radiation therapy may help slow disease progression, but these cancers are usually difficult to cure.
· Hepatoblastoma: An extremely rare form of cancer that typically occurs in children, especially those under the age of 4. Although these tumors are more difficult to manage if they spread outside the liver, approximately two-thirds of children with this condition can be successfully cured through surgery and chemotherapy.
Secondary Liver Cancer (Metastatic Liver Cancer): In most cases, when cancer cells are found in the liver, the cancer did not originate there but has metastasized from other parts of the body (such as the pancreas, colon, stomach, breast, or lung). The naming and treatment of these tumors depend on their primary site of origin. In the United States and Europe, metastatic liver tumors are more common than primary liver cancer, whereas in many regions of Asia and Africa, the opposite is true.
Etiology and Risk Factors
Liver cancer is typically caused by mutations in the DNA of hepatocytes. One consequence of such mutations is that cells may begin to grow uncontrollably, eventually forming a tumor, which consists of a large mass of malignant cells. Many factors can increase the risk of developing liver cancer, including the following categories:
· Chronic infection with hepatitis B or C virus. This is the most significant risk factor for liver cancer worldwide. These viruses can be transmitted from person to person through sharing contaminated needles, unprotected sexual contact, and from mother to child during childbirth;
· Liver cirrhosis;
· Certain hereditary liver diseases, including hemochromatosis and Wilson's disease;
· Certain inherited metabolic disorders;
· Diabetes and/or obesity;
· Non-alcoholic fatty liver disease;
· Exposure to aflatoxin. Aflatoxin is a toxic substance produced by molds that grow on crops stored under poor conditions; these crops may be contaminated with aflatoxin, ultimately leading to contamination of foods derived from them. In the United States, food safety regulations limit contamination attributable to aflatoxin, but in certain regions of Africa and Asia, food contamination due to aflatoxin remains relatively common;
· Arsenic exposure;
· Excessive alcohol consumption.
Life Expectancy
The life expectancy of patients with liver cancer depends on the clinical stage of the cancer and the site of metastasis. Generally, patients who can undergo surgical resection to remove the cancer have higher survival rates, regardless of the cancer stage. The American Cancer Society provides survival rate statistics for various types of cancer based on data from the Surveillance, Epidemiology, and End Results (SEER) database maintained by the National Cancer Institute (NCI). The SEER database tracks the 5-year relative survival rates of liver cancer patients in the United States according to the extent of cancer spread. The 5-year relative survival rates for individuals diagnosed with liver cancer, stratified by cancer stage, are as follows:
Localized disease indicates that the cancer remains confined to the liver, encompassing Stage I, Stage II, and certain Stage III cancers. The 5-year relative survival rate for patients with localized liver cancer is approximately 31%.
Regional disease indicates that the cancer has spread to nearby organs or lymph nodes adjacent to the liver, encompassing Stage IIIC and Stage IVA cancers. The 5-year relative survival rate for regional-stage liver cancer is approximately 11%.
Distant metastasis refers to the spread of cancer to distant organs or tissues, which is equivalent to stage IVB cancer. The 5-year relative survival rate for metastatic liver cancer is approximately 3%.
Most cases of liver cancer are initially diagnosed due to symptoms they cause, including sudden weight loss, loss of appetite, nausea or vomiting, hepatomegaly, splenomegaly, pain in the abdomen or near the right scapula, abdominal distension or ascites, pruritus, and jaundice. If a combination of symptoms and physical examination findings suggests the possibility of liver cancer, patients will undergo further testing, including imaging studies, laboratory tests, and liver biopsy.
Ultrasound is typically the preferred modality for liver examination, capable of detecting tumors developing within the liver; if abnormalities are identified, further testing can be conducted to determine whether cancer is present.
Imaging examinations use X-rays, magnetic fields, or sound waves to create images of the interior of the human body.
Computed Tomography (CT) Scan is an X-ray examination that can generate detailed images. A CT scan of the abdomen can detect various types of liver tumors and provide information on the size, shape, and location of any tumors in the liver or other parts of the abdomen, as well as nearby blood vessels.
Magnetic Resonance Imaging (MRI) scans use radio waves and strong magnets, rather than X-rays, to create detailed images of soft tissues within the body. They can differentiate between benign and malignant tumors, visualize blood vessels inside and around the liver to assess for blockages, and help determine whether liver cancer has metastasized to other parts of the body.
Angiography is an X-ray technique used to examine blood vessels. During the acquisition of X-ray images, angiography outlines the vascular structure by injecting a contrast agent or dye into the arteries. This technique can also visualize the arteries supplying blood to liver tumors, helping physicians determine whether the cancer is resectable and plan the corresponding surgical procedure. Additionally, it can be used to guide certain types of non-surgical treatments.
If the imaging results are inconclusive, other types of tests may be performed, including the following:
Biopsy: A biopsy involves removing a tissue sample for examination to determine whether it is cancerous. In some cases, the only way to confirm the presence of liver cancer is to perform a biopsy and send the sample to a pathology laboratory for further analysis.
Laboratory tests can help diagnose liver cancer and identify potential causes. These tests also assess the function of the liver and other organs, thereby guiding treatment decisions.
Alpha-fetoprotein (AFP) Blood Test. AFP is a protein found at high levels in adults with liver disease, liver cancer, pregnancy, or other cancers. Elevated AFP levels may indicate that a patient has liver cancer. This test is also useful for individuals already diagnosed with liver cancer. AFP levels can help determine viable treatment options and monitor treatment progress, as effective therapy should result in decreased AFP levels. Additionally, this test can be used after treatment to detect potential signs of cancer recurrence.
Other tests include those for viral hepatitis, liver and kidney function, coagulation, and complete blood count.
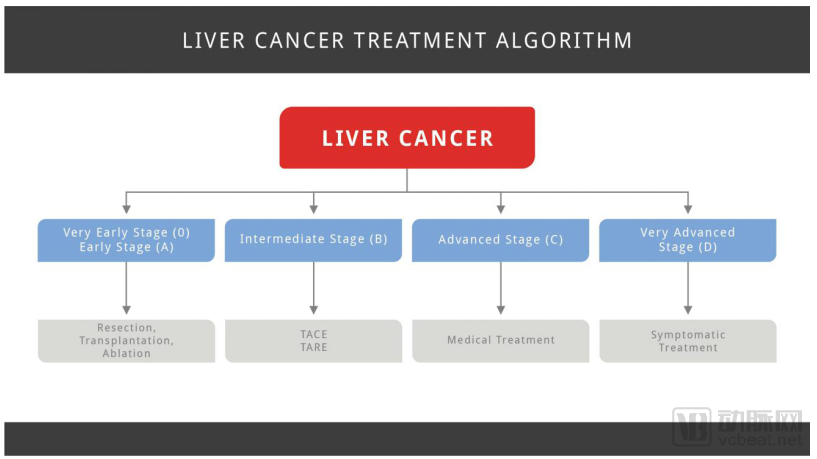
Current treatment modalities for liver cancer include surgery, ablation, embolization therapy, radiation therapy, targeted therapy, chemotherapy, and immunotherapy. The specific treatment approach depends on the stage of the liver cancer.
· Surgery: The optimal treatment options for liver cancer are surgical resection (removal of the tumor via surgery) or liver transplantation.
· Ablation: Ablation is a treatment method that destroys liver tumors without the need for surgical resection. This technique is typically used in patients found to have only small tumors, for whom surgery is not a favorable option (usually due to poor health status or impaired liver function).
· Embolization is a procedure that involves injecting substances directly into the hepatic artery to block or reduce blood flow to tumors in the liver. Embolization therapy is used for patients who are not candidates for surgical resection or ablation therapy and whose tumors have not spread beyond the liver.
· Radiation therapy uses high-energy rays to kill cancer cells.
· Chemotherapy (referred to as chemotherapy)
Targeted Therapy: This is a cancer treatment that uses drugs or other substances to more precisely identify and attack cancer cells while sparing healthy cells. Targeted therapy can also be combined with other treatments, such as chemotherapy, to identify and target cancer cells. Targeted therapies for liver cancer include Bayer’s Nexavar (sorafenib) and Eisai’s Lenvima (lenvatinib). In cases where sorafenib becomes ineffective, alternative treatments are used, including Bayer’s Stivarga (regorafenib), Ipsen’s Cabometyx (cabozantinib), and Eli Lilly’s Cyramza (ramucirumab).
Immunotherapy, also known as immune checkpoint inhibitors, works by harnessing the body’s own immune system to detect and destroy cancer cells. Examples of immunotherapies include Merck’s Keytruda (pembrolizumab) and Bristol Myers Squibb’s Opdivo (nivolumab), both of which target PD-1. PD-1 is a protein found on T cells, a type of immune cell, that normally helps prevent immune cells from attacking other cells in the body. By blocking PD-1, these drugs enhance the immune system’s ability to target cancer cells, thereby shrinking certain tumors or slowing their growth. These medications may also be used in patients with liver cancer who have previously been treated with the targeted therapy Nexavar (sorafenib).
 Staging of Liver Cancer
Staging of Liver Cancer
Various therapies are currently being explored through clinical trials. In addition to the targeted therapies and immunotherapies listed above, common targets and mechanisms in clinical trials also include:
· Alpha-fetoprotein (AFP) inhibitors: Alpha-fetoprotein (AFP) is a diagnostic marker for hepatocellular carcinoma (HCC). There is a direct correlation between elevated serum AFP levels and poor prognosis. Elevated AFP concentrations are observed in approximately 70% of patients with hepatocellular carcinoma.
· Multikinase inhibitors exert their effects by inhibiting multiple intracellular and cell-surface kinases. Some of the kinases targeted by these drugs are involved in tumor growth and the metastatic process of cancer cells, thereby indirectly reducing the growth and replication of tumor cells.
· Fibroblast Growth Factor Receptor 4 (FGFR4) Inhibitors: FGFR4 is a tyrosine kinase receptor for FGFs and participates in various cellular processes. In many common solid tumors and hematologic malignancies, hyperactivation of FGFR4 is closely associated with amplification of its specific ligand, FGF19, and it also functions as an oncogene driving carcinogenesis and disease progression.
· PD-1 Antibodies: Programmed cell death protein 1 (PD-1) is an inhibitory receptor that is overexpressed on certain tumor cells and leads to immune suppression by reducing T-cell activity in the human body. Anti-PD-1 monoclonal antibodies block the PD-1 receptor, thereby relieving T-cell inhibition and activating the body’s immune response against tumor cells.
· TGFβ: Transforming growth factor-β (TGF-β) is a family of structurally related proteins that regulate a wide range of cellular functions in the human body. In advanced-stage cancer, TGF-β promotes tumor cell growth, enhances tumor invasiveness, and accelerates metastasis; therefore, elevated TGF-β activity is generally associated with adverse clinical outcomes.
· A3 adenosine receptor (A3AR) agonists: A3AR exerts anti-inflammatory, anticancer, and cytoprotective effects against ischemia. The expression of this receptor is upregulated in inflammatory and cancer cells.
In January 2020, 892 clinical trials were underway, encompassing various stages such as patient recruitment, pre-recruitment, trial initiation, and suspension of patient enrollment. Among these, 255 were industry-led and funded studies, while the remainder were funded by U.S. government agencies, universities, hospitals, and other institutions. A total of 721 studies were drug-based interventional trials, with the rest being observational studies. Geographically, 315 trials were conducted in the United States, while the others were distributed globally. By phase, there were 192 Phase I trials, 285 Phase II trials, and 115 Phase III trials. The remaining trials were in Phase IV or fell into other categories, including behavioral modification or observational studies, all of which employed dietary therapy and device-based monitoring.
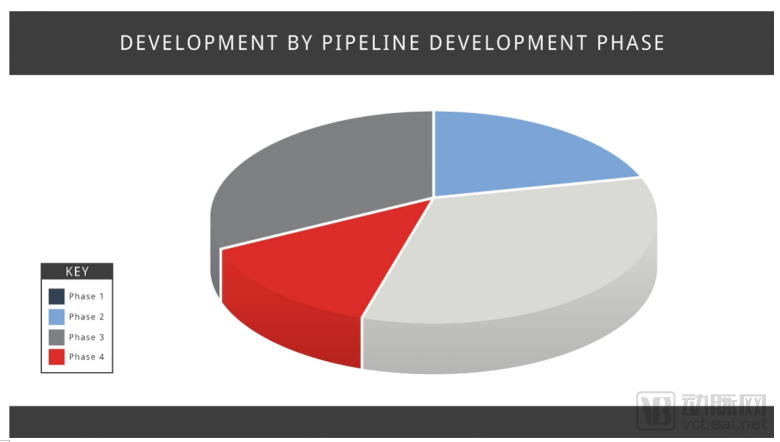
Distribution of Clinical Trial Phases for Liver Cancer
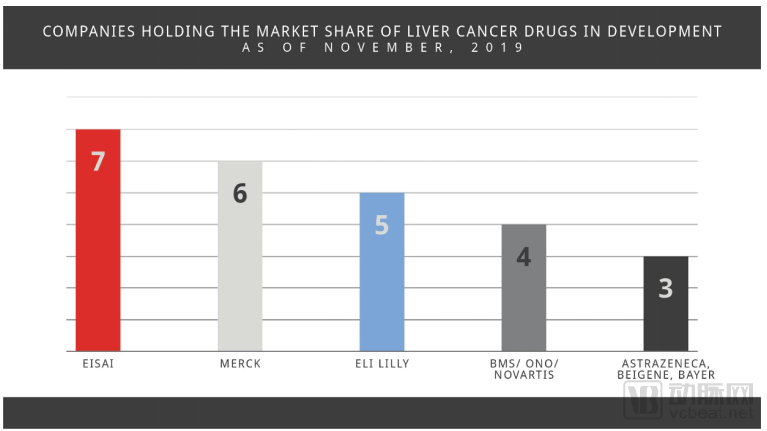
The liver cancer market comprises pharmaceutical and biotechnology companies of various sizes. Eisai dominates the market share, with seven ongoing studies, followed by Merck & Co. (six studies), Eli Lilly (five studies), Bristol Myers Squibb, Ono Pharmaceutical, and Novartis (four studies each). AstraZeneca, BeiGene, and Bayer trail behind, with three studies each.
 Top Five Clinical Trials for Liver Cancer. Note: This report does not constitute a comprehensive statistical analysis of clinical drug trials and may inadvertently exclude certain drugs under development or in clinical trials, particularly those outside the United States.
Top Five Clinical Trials for Liver Cancer. Note: This report does not constitute a comprehensive statistical analysis of clinical drug trials and may inadvertently exclude certain drugs under development or in clinical trials, particularly those outside the United States.
Eisai is evaluating the kinase inhibitor lenvatinib as monotherapy for liver cancer and assessing it in various combinations across seven Phase I and Phase III studies. Lenvatinib, marketed under the brand name Lenvima, has been approved by the FDA for patients with thyroid cancer, renal cell carcinoma, and unresectable hepatocellular carcinoma.
Merck & Co. is evaluating pembrolizumab and tepotinib through six studies, including Phase I/II, Phase II, and Phase III trials. Pembrolizumab is a programmed death receptor-1 (PD-1) blocking antibody that has been approved for marketing in multiple cancer indications. Clinical studies are assessing the efficacy of pembrolizumab as monotherapy and in combination with lenvatinib. Meanwhile, Merck is also investigating the clinical efficacy of tepotinib, a c-Met receptor tyrosine kinase inhibitor, whose Phase I/II clinical trial results were disclosed in June 2018.
Eli Lilly and Company has developed two drugs targeting hepatocellular carcinoma (HCC) across five studies: galunisertib (LY2157299) and ramucirumab. Galunisertib is a potent small-molecule antagonist that specifically inhibits transforming growth factor-beta receptor I (TβRI). The results of its Phase II clinical trial were published in *Liver International* in April 2019. The trial demonstrated that galunisertib had a manageable safety profile in patients with HCC. Lower baseline alpha-fetoprotein (AFP) levels and responses in AFP or TGF-β1 levels (versus non-response) were associated with longer survival. Ramucirumab is a human vascular endothelial growth factor receptor 2 (VEGFR2) antagonist. It has been approved for the treatment of gastric cancer, non-small cell lung cancer, colorectal cancer, and AFP-high hepatocellular carcinoma.
Bristol-Myers Squibb and Ono Pharmaceutical are collaborating to evaluate the efficacy of nivolumab as a monotherapy, incorporating data from four studies. Nivolumab is a programmed death receptor-1 (PD-1) blocking antibody. It has been approved under the brand name Opdivo for various cancers, including accelerated approval for the treatment of patients with hepatocellular carcinoma (HCC) who have previously received sorafenib therapy.
Novartis is currently conducting multiple clinical trials, four of which are evaluating PDR001 as monotherapy and in combination therapies. PDR001 is a fully humanized anti-PD-1 monoclonal antibody being assessed in combination with the following agents: Novartis’s monoclonal antibody NIS793 (targeting transforming growth factor-beta [TGF-β]); capmatinib (INC280), an oral and highly potent MET inhibitor licensed to Novartis by Incyte Corporation in 2009; and sorafenib (Nexavar).
AstraZeneca is currently conducting three Phase III clinical studies to evaluate the efficacy of durvalumab, a human immunoglobulin G1 kappa (IgG1κ) monoclonal antibody that blocks the interaction between programmed death-ligand 1 (PD-L1) and PD-1. Durvalumab has been approved for the treatment of non-small cell lung cancer under the brand name Imfinzi. The ongoing studies include EMERALD-2 (monotherapy versus bevacizumab or durvalumab in combination), EMERALD-1 (transarterial chemoembolization [TACE] monotherapy versus TACE combined with durvalumab and bevacizumab), and HIMALAYA (durvalumab plus tremelimumab combination therapy and durvalumab monotherapy versus sorafenib). In June 2017, the safety and clinical activity of durvalumab monotherapy were reported.
Bayer has three ongoing studies. One study is evaluating regorafenib for the treatment of patients diagnosed with unresectable hepatocellular carcinoma in real-world settings. Another Phase 1b clinical study, conducted in collaboration with Merck & Co., is assessing the combination of regorafenib and pembrolizumab for the treatment of patients with advanced hepatocellular carcinoma (HCC) who have not received comprehensive prior therapy. The third study is evaluating the efficacy of copanlisib, a kinase inhibitor, in combination with nivolumab for the treatment of patients with solid tumors.
BeiGene is evaluating tislelizumab (BGB-A317), a humanized monoclonal antibody targeting the immune checkpoint receptor PD-1, and sitravatinib, an inhibitor that selectively inhibits receptor tyrosine kinases and split-family receptors. BeiGene is currently conducting three clinical trials to assess tislelizumab as monotherapy (Phase II); tislelizumab in combination with sorafenib (Phase III); and sitravatinib as monotherapy and in combination with tislelizumab (Phase I/II).
Exelixis is conducting the Phase III COSMIC-312 trial and the Phase I/II COSMIC-021 trial to evaluate the combination therapy of cabozantinib and atezolizumab. Cabozantinib is a targeted agent that inhibits the activity of tyrosine kinase receptors, including MET, AXL, VEGF receptors, and RET. At the 2018 ASCO Gastrointestinal Cancers Symposium, data from the Phase III CELESTIAL trial were presented, demonstrating that cabozantinib significantly improved overall survival and post-progression survival in patients with advanced hepatocellular carcinoma who had previously received sorafenib, compared with placebo, without introducing additional safety concerns.
Immunitor has developed hepcortespenlisimut-L (Hepko-V5), a once-daily oral immunotherapeutic vaccine. The results of the Phase II trial were published in the Journal of Hepatocellular Carcinoma in April 2017. This open-label study evaluated the immunotherapeutic vaccine in 75 patients with advanced hepatocellular carcinoma, and 90% of the patients remained alive after 12 months of follow-up. Furthermore, after a median treatment duration of 2 months, alpha-fetoprotein (AFP) levels decreased in 50 of the 75 patients, indicating that two-thirds of the study population responded to the immunotherapy, as a decline in AFP is positively correlated with tumor shrinkage.
Hengrui Medicine is investigating camrelizumab (SHR-1210), a humanized monoclonal antibody targeting the PD-1 receptor. A Phase II study is currently recruiting patients with primary liver cancer or biliary tract cancer to evaluate the efficacy of SHR-1210 in combination with either apatinib (a tyrosine kinase inhibitor that selectively inhibits VEGFR2) or chemotherapy (FOLFOX4 or GEMOX regimens).
Another Phase III study is currently enrolling patients with advanced hepatocellular carcinoma who have not previously received systemic therapy. Patients in this study will receive combination treatment with camrelizumab plus FOLFOX4 (chemotherapy). Previous Phase II clinical trial results indicated that camrelizumab combined with either FOLFOX4 or GEMOX chemotherapy was well tolerated, demonstrating significant efficacy based on objective response rate and disease control rate.
Roche is conducting Phase II and Phase III studies (IMbrave050 and IMbrave150) to evaluate the combination of atezolizumab (a humanized monoclonal antibody targeting the PD-L1 protein) and bevacizumab (a VEGF inhibitor). In October 2019, results from IMbrave150 demonstrated that this combination prolongs both overall survival and progression-free survival in patients. Atezolizumab had previously been approved for the treatment of lung cancer under the brand name Tecentriq. Bevacizumab has also been approved for multiple types of cancer under the brand name Avastin.
Namodenoson (CF-102), owned by Can-Fite BioPharma, is a small-molecule oral drug with high affinity and selectivity for the A3 adenosine receptor (A3AR). In September 2019, Can-Fite successfully completed an End-of-Phase II meeting with the U.S. FDA regarding its recently completed Phase II study on the treatment of hepatocellular carcinoma (HCC). During the meeting, the FDA agreed to Can-Fite’s proposed design for a pivotal Phase III trial to support the submission and approval of a New Drug Application. Can-Fite expects to initiate this study in the second half of 2020.
Innovent Biologics is conducting a Phase II/III study (ORIENT-32) to evaluate the combination of sintilimab and IBI305 (a bevacizumab biosimilar). Sintilimab is a fully human IgG4 monoclonal antibody that specifically binds to PD-1 expressed on the surface of human T cells, thereby blocking the immune escape pathway of cancer cells, while reactivating T cells and releasing cytokines to kill tumor cells. IBI305 is a biosimilar candidate of bevacizumab, a recombinant humanized anti-VEGF monoclonal antibody for injection.
Regeneron is collaborating with Sanofi on a Phase II trial in patients who have undergone surgical tumor resection, with indications including liver cancer. The trial aims to evaluate the efficacy of cemiplimab as a neoadjuvant monoclonal antibody therapy. Cemiplimab is a programmed death-1 (PD-1) blocking antibody that has been approved for the treatment of patients with metastatic cutaneous squamous cell carcinoma under the brand name Libtayo.
TaiRx is evaluating the combination of CVM-1118 and sorafenib. CVM-1118 modulates vasculogenic mimicry (VM), a mechanism associated with tumor metastasis and poor clinical prognosis. It has been reported that VM is particularly active in hypoxic tumors when patients are treated with potent VEGF inhibitors such as sorafenib.
Yiviva has developed YIV-906 (PHY906, KD018), a botanical drug candidate inspired by an 1,800-year-old classic Chinese herbal formula, for the treatment of various gastrointestinal symptoms, including diarrhea, nausea, and vomiting. Extensive clinical and preclinical studies have indicated that YIV-906 may exhibit synergistic anticancer activity and reduce gastrointestinal toxicity associated with cancer therapies, including sorafenib. The Phase 2 trial will investigate the efficacy and mechanism of action of YIV-906 as an adjunct to sorafenib in patients with hepatitis B virus–related or other forms of hepatocellular carcinoma.
Abivax is investigating ABX196, a synthetic glycolipid agonist capable of activating invariant natural killer T (iNKT) cells. Phase I clinical trials in healthy subjects have been completed, demonstrating its safety, tolerability, and effective activation of iNKT cells. Current studies are evaluating the combination of ABX196 with nivolumab.
AVEO Oncology is collaborating with AstraZeneca to evaluate the combination of tivozanib and durvalumab. Tivozanib is an oral, once-daily VEGF tyrosine kinase inhibitor. AVEO Oncology licensed tivozanib from Kyowa Kirin in 2006, and it has been approved for the treatment of advanced renal cell carcinoma (RCC) in the European Union, Norway, New Zealand, and Iceland. Interim results from Phase I/II studies reported in January 2018 demonstrated the efficacy and safety of the combination therapy.
Boston Biomedical has two drugs in development: napabucasin (BBI-608) and amcasertib (BBI-503). Although patient enrollment for related drug trials has ceased, two clinical trials targeting hepatocellular carcinoma are currently ongoing. Napabucasin is an oral formulation that inhibits cancer cell stemness by targeting STAT3. Amcasertib is an oral formulation designed to inhibit cancer stemness pathways, such as Nanog, by targeting stemness kinases.
Eureka Therapeutics is developing an autologous T-cell product (ET140202) for adults to treat alpha-fetoprotein (AFP)-positive/HLA-A2-positive hepatocellular carcinoma. This product involves genetically modifying autologous T cells to express a T-cell receptor mimic (TCRm) construct that targets tumor-specific intracellular antigens, thereby mediating cytotoxic activity. Data from the first-in-human proof-of-concept (POC) study conducted in China in September 2018 demonstrated that ET140202 has a favorable safety profile, with no observed cytokine release syndrome or drug-related neurotoxicity.
Genoscience Pharma has developed a quinoline derivative, GNS561. This drug is a novel class of oral small molecules capable of inducing multiple cellular effects, such as inhibiting autophagy, inducing apoptosis, and regulating the cell division cycle. The ongoing Phase I/II clinical trials were expected to be completed in January 2020.
Medivir is developing MIV-818, generically known as troxacitabine, an oral nucleoside analog that precisely targets the liver and exhibits high levels of antitumor activity. Clinical trials for this drug have enrolled patients with hepatocellular carcinoma, intrahepatic cholangiocarcinoma, and solid tumors with liver metastases.
OBI-3424, a novel small-molecule drug under investigation by OBiO Biopharma (Taiwan, China), selectively targets cancer cells with high overexpression of aldo-keto reductase 1C3 (AKR1C3) and can selectively release DNA alkylating agents with anticancer effects in the presence of the AKR1C3 enzyme. AKR1C3 overexpression has been found in many treatment-resistant or difficult-to-treat cancers, including hepatocellular carcinoma. In June 2018, phase I/II clinical trials of this drug began in patients with solid tumors, including hepatocellular carcinoma and castration-resistant prostate cancer.
Polaris Pharma (Taiwan, China) is evaluating the efficacy of ADI-PEG 20 (pegylated arginine deiminase). This enzyme inhibits the growth of arginine-dependent cancer cells by depleting arginine. Phase I/II clinical trials of ADI-PEG 20 are underway in various tumor types, including hepatocellular carcinoma (HCC).
Teclison has developed a hypoxia-selective cytotoxin named tirapazamine (TPZ). When combined with transarterial chemoembolization (TACE), TPZ selectively creates a sustained hypoxic environment within liver tumors to activate the compound. Conversely, in normal liver tissue or other non-hypoxic organs, the compound remains inactive, thereby avoiding adverse effects on healthy tissues. Although patient enrollment has ceased, three clinical trials involving this drug remain active.
Adaptimmune is conducting a Phase I clinical study of ADP-A2AFP, a T-cell product engineered to target alpha-fetoprotein (AFP). The trial is evaluating the efficacy of this T-cell therapy in patients who are HLA-A*02-positive and exhibit high levels of AFP protein in their blood or tumors.
Amgen and Merck are collaborating on the MASTERKEY-318 study. This trial involves the intratumoral injection of talimogene laherparepvec into liver tumors, combined with systemic administration of pembrolizumab, to evaluate the efficacy of this combination therapy in patients with hepatocellular carcinoma. Talimogene laherparepvec is an oncolytic immunotherapy derived from herpes simplex virus type 1 (HSV-1) that has previously been approved for the treatment of melanoma under the brand name Imlygic.
Blueprint Medicines has developed fisogatinib (BLU-554), an oral, potent, and irreversible FGFR4 inhibitor. The company is advancing this drug for the treatment of patients with FGFR4-driven hepatocellular carcinoma, with Phase I clinical trials currently underway and expected to conclude in October 2020.
Chipscreen Biosciences is evaluating the efficacy of Chiauranib, a drug that simultaneously targets VEGFR, Aurora B, and CSF-1R—key kinases primarily associated with tumor angiogenesis, tumor cell mitosis, and the chronic inflammatory microenvironment. Chiauranib has demonstrated broad preclinical antitumor efficacy and holds the potential to become a best-in-class tyrosine kinase inhibitor. The current Phase Ib clinical trial is enrolling patients with advanced hepatocellular carcinoma.
Immatics has developed IMA202, an ACTengine product that enhances the function of patients’ own T-cell receptors (TCRs) via lentiviral transduction. This approach essentially “reprograms” patients’ T cells to attack tumor cells. Currently, the associated Phase I trial is enrolling patients with solid tumors expressing melanoma-associated antigen 1 (MAGEA1). The trial is being conducted in collaboration with the MD Anderson Cancer Center.
Incyte is currently enrolling patients in an open-label (both participants and investigators are aware of the study design and treatment assignment) Phase I trial to evaluate the response to INCB062079 in patients with advanced hepatocellular carcinoma and other malignancies. INCB062079 is an oral, bioactive, selective FGFR4 inhibitor with potential antitumor activity.
Provectus Biopharmaceuticals is investigating PV-10, an injectable formulation of rose bengal disodium. Provectus’s experimental data indicate that upon cellular contact, PV-10 selectively accumulates in the lysosomes of cancer cells, disrupting them and inducing cancer cell death. A Phase I clinical trial is currently underway, evaluating intralesional single-dose injections of PV-10 in patients with hepatocellular carcinoma or hepatic metastases who are not candidates for surgical resection, transplantation, or other potentially curative therapies.
Therapure Biopharma is in the early stages of testing TBI302, a hemoglobin-conjugated floxuridine compound. Floxuridine is an effective chemotherapeutic agent used to treat hepatic tumors. Therapure’s protein-drug conjugation platform technology leverages hemoglobin—the natural protein responsible for transporting oxygen to tissues in the human body—to link drugs with hemoglobin, thereby improving drug delivery and transport to specific sites of action while minimizing effects on non-target tissues.
Below is a sample of companies developing and researching drugs and other therapies in preclinical laboratory settings. Data collected from these preclinical trials will be used to determine whether drugs and therapies will evolve as they progress into human clinical trials.
Auransa is an artificial intelligence (AI)-driven biotechnology company dedicated to developing precision medicines. It is currently advancing the drug candidate AU-409, which was generated using the company’s proprietary AI-powered SMarTR™ engine. The SMarTR engine addresses disease heterogeneity by leveraging gene expression profiles to predict either the patient populations likely to respond to a drug or the compounds effective for specific patient subgroups. Preclinical data related to AU-409 were presented in September 2019 at the 13th Annual Meeting of the International Liver Cancer Association (ILCA) in Chicago. The results demonstrated that AU-409 exhibited promising antitumor activity in preclinical orthotopic liver cancer models and significantly reduced tumor burden in humanized models. Auransa is poised to initiate clinical trials for AU-409, with Phase I human testing expected to commence in the first half of 2020.
Sirnaomics is evaluating the preclinical candidate drug STP705, which consists of two siRNAs targeting the TGF-β1 and COX-2 genes, delivered via a peptide nanoparticle delivery system based on histidine-lysine copolymer (HKP). Preclinical data indicate that STP705 can inhibit the growth of HuCCt-1 (a human cholangiocarcinoma cell line) xenograft tumors in nude mice.
SFA Therapeutics is developing SFA001, a microbiome-based therapeutic. This drug was developed from natural substances through SFA Therapeutics’ proprietary discovery process, which matches metabolites with adjuvants to treat chronic inflammatory diseases. Based on preclinical studies in transgenic HBx animal models (a mouse model of hepatitis B), the U.S. Food and Drug Administration (FDA) granted orphan drug designation to SFA001 in October 2019. In these experiments, SFA001 significantly reduced both the number and size of hepatocellular carcinoma (HCC) tumors. Furthermore, studies in two different HCC animal models demonstrated that the mechanism of action of SFA001 is not associated with chemical toxicity.
In the United States and globally, given the rising prevalence and high mortality rate of hepatocellular carcinoma (HCC), there is an urgent need for novel prevention and treatment strategies to reduce its incidence and impact. These strategies may include vaccine development, advanced screening technologies, various types of neoadjuvant therapies, cutting-edge ablation techniques, targeted therapies, and the identification of specific biomarkers (proteins).
Vaccine Therapy
Personalized Peptide Vaccines (PPV) are an immunotherapeutic approach that involves injecting multiple tumor-associated peptides as immunogenic antigens into patients to elicit tumor-specific immune responses, thereby augmenting the patient’s pre-existing immune capacity. Furthermore, advances in genomics and bioinformatics have facilitated the development of personalized peptide vaccines derived from neoantigens. These vaccines have demonstrated safety and feasibility in clinical trials.
The results of the feasibility study on personalized peptide vaccines (PPV) were published in the journal *Cancer Science* in September 2017. In this article, the PPV peptides were selected from 31 candidate peptides based on data from 26 patients with hepatocellular carcinoma (HCC) refractory to local therapy (Cohort 1) and 30 patients with HCC refractory to both local and systemic therapies (Cohort 2). At the end of the first cycle consisting of six vaccinations, immune responses were successfully enhanced in 57% or 46% of patients in Cohort 1, and in 54% or 52% of patients in Cohort 2. Among most patients who responded positively to the treatment, an increase in serum albumin levels was observed by the end of the second cycle.
The link between hepatitis B infection and the subsequent development of liver cancer underscores the need to establish global hepatitis B vaccination programs. According to an article published in Frontiers in Biosciences, studies have observed a strong correlation between hepatitis B vaccine coverage and a decline in hepatocellular carcinoma incidence in regions where the vaccine is widely used. The article cites several other studies indicating that both the prevalence and mortality rates of hepatocellular carcinoma are reduced following HBV vaccination.
Advanced Screening Technologies
Several novel blood tests are currently under investigation. Researchers aim to determine whether these tests can detect liver cancer earlier than the combination of serum alpha-fetoprotein (AFP) testing and ultrasonography. The biomarkers under study include des-gamma-carboxy prothrombin (DCP), glypican-3, osteopontin (OPN), and Golgi protein 73. In addition, studies are evaluating whether computed tomography (CT) and magnetic resonance imaging (MRI) can replace ultrasonography as the imaging modality for liver cancer screening.
· Des-gamma-carboxy prothrombin (DCP) is an abnormal form of the coagulation protein prothrombin. Elevated DCP levels are associated with an increased risk of hepatocellular carcinoma recurrence. The risk of having liver cancer is 36.5% in patients with elevated DCP results, compared to 7.6% in those with negative DCP results.
· Given that Glypican-3 (GPC3) is highly expressed in hepatocellular carcinoma cells but is absent or expressed at low levels in normal adult tissues, clinical studies are evaluating its potential as a biomarker for targeted therapy and the diagnosis of hepatocellular carcinoma. Recent clinical trials have demonstrated the promise of GPC3 as both a diagnostic molecule and a therapeutic target for immunotherapy in hepatocellular carcinoma.
· Osteopontin (OPN) is a multifunctional protein that serves as a signaling molecule in the human immune and vascular systems. Relevant studies have demonstrated that OPN is highly expressed in hepatocellular carcinoma (HCC) tumor tissues and is correlated with tumor grade, stage, and recurrence. Furthermore, research indicates that elevated serum OPN concentrations are associated with adverse postoperative outcomes, declined liver function, lower Child-Pugh scores, as well as reduced disease-free survival and overall survival. These findings suggest that OPN may offer new therapeutic avenues for hepatocellular carcinoma.
· Golgi protein 73 (GP73) has emerged as a serum biomarker for liver cancer. Numerous studies have demonstrated an association between GP73 and liver diseases, particularly hepatocellular carcinoma, suggesting its potential as a novel serological marker for early diagnosis. An article published in *Cell Proliferation* in October 2018 conducted a retrospective analysis of GP73 and summarized global research data on the relationship between GP73 and liver diseases across various clinical settings.
Neoadjuvant Therapies
Neoadjuvant therapy involves the administration of certain adjuvant therapeutic agents prior to the definitive primary treatment for cancer. The purpose of neoadjuvant therapy is to reduce the size or extent of the cancer before definitive treatment, thereby facilitating surgical resection without compromising tumor control rates, improving surgical success rates, and reducing postoperative complications associated with extensive surgery. Types of neoadjuvant therapies include targeted therapy, chemotherapy, drug ablation, embolization, and radiation therapy.
A clinical study published in the Journal of Clinical Oncology in July 2019 aimed to compare the therapeutic efficacy of neoadjuvant three-dimensional conformal radiotherapy (RT) combined with hepatectomy versus hepatectomy alone in patients with hepatocellular carcinoma and portal vein tumor thrombus (PVTT). The study demonstrated that, for patients eligible for curative resection, neoadjuvant radiotherapy yielded superior postoperative survival outcomes compared to surgery alone.
In addition, a novel ablation technology known as irreversible electroporation (IRE), or the Nanoknife, does not rely on traditional hyperthermic or cryogenic mechanisms to destroy cancer cells. Instead, it employs high-voltage pulses to create permanent nanoscale pores in cell membranes, thereby inducing cancer cell death. This approach may offer therapeutic benefits for certain hard-to-treat cancers.
Targeted Therapy
Based on recently approved drugs and those currently being launched, we have found that targeted drug therapy is a major focus in the development of many anticancer agents. Targeted cancer therapies work by interfering with specific molecules involved in the growth, progression, and spread of cancer cells, thereby inhibiting tumor growth and metastasis. Targeted cancer therapies are also referred to as “molecularly targeted drugs,” “molecular targeted therapy,” or “precision medicine drugs.”
Targeted therapy differs from standard chemotherapy in certain aspects:
· Targeted therapies act on specific molecular targets associated with cancer, whereas most standard chemotherapy agents act on all rapidly proliferating cells, including both normal and cancerous cells in the human body.
· Targeted therapies are specifically designed to interact with their targets, whereas many standard chemotherapeutic agents were identified simply because of their ability to kill cells.
· Targeted therapies typically exert an inhibitory effect on cell growth (i.e., they prevent cell proliferation), whereas conventional chemotherapy agents are cytotoxic (i.e., they kill cells).
Over the past decade, the treatment landscape for liver cancer, or hepatocellular carcinoma (HCC), has undergone significant changes. Since the approval of Nexavar in 2007 as the first pharmacological therapy, six additional novel drugs have been introduced sequentially. The next phase in oncology drug therapy may involve exploring various combination regimens and further developing immune checkpoint inhibitors and cellular immunotherapies to provide more patients with opportunities for remission.
The future of liver cancer treatment may also focus on the analysis of molecular pathways, some of which are known to influence the growth of hepatocellular carcinoma (HCC) itself. Theoretically, these molecular pathways could be leveraged to slow, halt, or reverse the progression of HCC. With advances in human drug development, personalized therapies for liver cancer cells based on biomarkers, molecular pathways, and immune responses are poised to deliver significant breakthroughs.
Translation: Zhou Qianyun
Source: https://www.biospace.com/article/insight-report-liver-cancer/