Empowering Epidemic Early Warning with Big Data: Comprehensive Applications in Disease Control
Unlike in the past, China’s technological capabilities have now improved significantly, even leading globally in certain fields, particularly in innovative technologies such as cloud computing, big data, and artificial intelligence. In the current epidemic prevention and control efforts, we have armed ourselves with high-tech solutions, turning these technologies into powerful weapons against the outbreak. They have been widely applied in areas including epidemic tracking and source identification, transmission pathway analysis, predictive modeling of disease progression, and resource allocation.
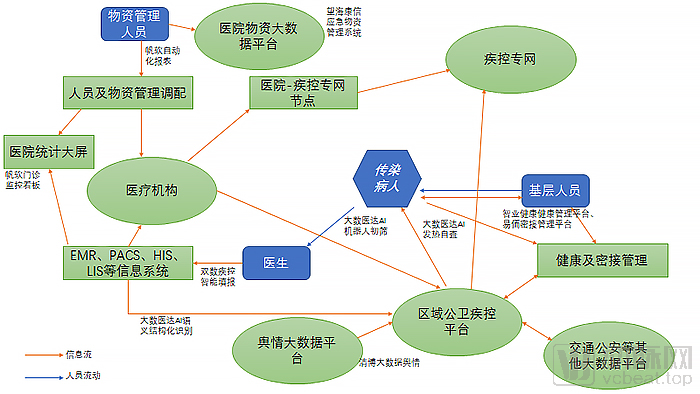
Application of Big Data in Disease Control and Prevention (Graphic by VCBeat, for reference only)
What Contributions Has Big Data Made to the Current Epidemic Prevention and Control? What Potential Role Can It Play in Future Disease Control and Prevention? VCBeat (WeChat ID: Vcbeat) Has Compiled an Overview.
Big Data Is Indispensable for Disease Control Warning and Monitoring, Provided the Data Are “Real”
According to media reports, on December 26, 2019, Zhang Jixian, Director of the Department of Respiratory Medicine at Hubei Provincial Hospital of Integrated Chinese and Western Medicine, was surprised to find that three other similar entries had already been recorded in the electronic medical record system that morning, all containing the same three keywords: “fever,” “cough,” and “Huanan Seafood Market.”
Experienced physician Zhang Jixian detected anomalies and reported them on December 27 to the vice president, as well as to the departments of hospital infection control and medical affairs. The hospital promptly submitted the data to the Jianghan District Center for Disease Control and Prevention in Wuhan. By December 29, the number of similar cases had risen to seven, prompting Zhang Jixian to report again to the hospital. The hospital immediately convened a multidisciplinary consultation. Subsequently, Hubei Provincial Hospital of Integrated Chinese and Western Medicine directly reported to the Disease Control and Prevention Divisions of both the Hubei Provincial and Wuhan Municipal Health Commissions.
Zhang Jixian is regarded as the “first person to report the epidemic,” and Hubei Provincial Hospital of Integrated Chinese and Western Medicine was the first hospital to officially report the outbreak.
The earliest case reported in public records dates back to December 8, 2019. During the following two weeks, other hospitals in Wuhan also began receiving similar cases. According to reports, out of an abundance of caution, hospital authorities opted to first conduct gene sequencing to identify the pathogen before filing official reports. Given that this was a novel virus, the time required for genomic sequencing was understandable and justifiable.
However, let us hypothesize: if big data and artificial intelligence had been available to capture these early subtle clues in real time, might the outcome have unfolded differently?
Of course, some may question why the National Direct Reporting Network for Infectious Diseases and Public Health Emergencies (hereinafter referred to as the CDC Direct Reporting Network), which was launched in 2004 at a substantial cost of RMB 730 million, failed to serve its early warning function.
According to VCBeat and public media reports, the CDC’s direct reporting private network has not been entirely ineffective; however, its data sources rely exclusively on self-reported submissions. Due to various factors, the network cannot be directly connected to hospitals’ internal systems. Without access to such data, the system is naturally unable to function effectively.
On February 3, the National Health Commission issued the “Notice on Strengthening Informatics Support for the Prevention and Control of Novel Coronavirus Pneumonia.” In accordance with the notice, local health commissions continuously improved data collection methods, with most hospitals adopting direct online reporting, thereby gradually leveraging the role of dedicated networks.
For big data, authentic data sources are of paramount importance. During the course of this epidemic, it has become clearly evident that conclusions drawn from inaccurate data deviate significantly from reality. How can we obtain authentic and reliable data from the frontline of medical institutions? The primary systems—Electronic Medical Record (EMR) systems, Laboratory Information Systems (LIS), Picture Archiving and Communication Systems (PACS), and Hospital Information Systems (HIS)—provide us with reliable data sources.
Electronic Medical Records (EMR) serve as the primary source of data and constitute a core system in the national initiative to upgrade hospital informatization. From 2018 to 2019, the State Council and the National Health Commission issued a total of nine policies that explicitly outlined mandatory requirements for electronic medical records. In 2019, more than 7,000 hospitals across China applied for the national EMR grading evaluation.
Leveraging big data and artificial intelligence to analyze electronic medical records (EMRs) for disease control and prevention is not only feasible but also a current hot topic. The Disease Surveillance and Early Warning System built by Beijing Dashu Yida Technology Co., Ltd. for the Nanjing Center for Disease Control and Prevention directly connects with local hospitals' EMRs.
This disease control monitoring and early warning system utilizes the most advanced big data and artificial intelligence technologies from Beijing Dashu Yida Technology Co., Ltd. It builds models based on medical knowledge graphs and directly extracts electronic medical records (EMRs) for semantic structuring. Artificial intelligence then matches these structured data against a knowledge base to determine whether the EMRs contain keywords related to infectious diseases such as COVID-19. Once identified by the AI as suspected or highly suspected cases, the information is automatically reported to the disease control authorities, thereby preventing hospitals from omitting or delaying reports due to unforeseen circumstances.
The system is directly integrated with and connected to hospital EMR systems, serving as a reporting, data aggregation, and early warning analysis platform for provincial and municipal Centers for Disease Control and Prevention (CDCs). It offers granular data capabilities, covering not only the 40 statutorily notifiable infectious diseases but also allowing regions to supplement locally prevalent infectious diseases as recognized by local authorities.
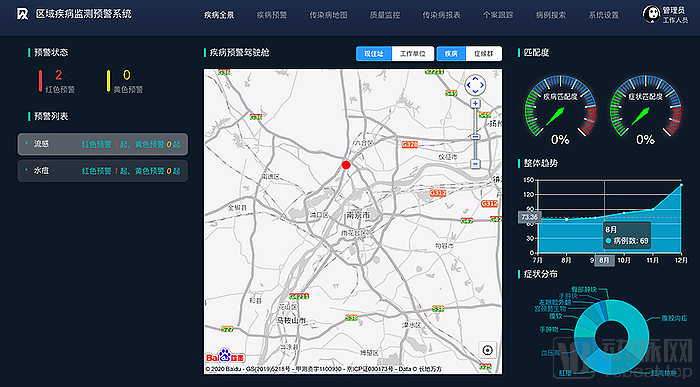
Dashu Yida Regional Disease Surveillance and Early Warning System (All displays are for demonstration purposes only and do not represent any actual significance)
Meanwhile, the system learns from historical disease control data and integrates big data such as regional population density and mobility rates to predict the transmission speed and geographic distribution of suspected infectious disease cases, thereby providing reference data for disease control decision-making.
Overall, to implement epidemic prevention and control measures in a solid and thorough manner, it is essential to leverage AI and big data technologies. This requires not only integrating vertical domain data across the “ministry-province-city-district/county” hierarchy within the industry but also breaking down cross-sectoral “information silos” horizontally. From the top-level design stage, real-time interoperability of structured information and coordinated joint prevention and response mechanisms must be established.
The system built by Beijing Dashu Yida Technology Co., Ltd. for Jiangsu Province was originally prepared for the spring influenza peak, but unexpectedly played a significant role during the more severe COVID-19 outbreak. Statistics show that if Wuhan, the epicenter of the outbreak, is taken as the origin and a circle with a radius of approximately two hours along high-speed rail lines is drawn, it becomes clear that disease control capabilities vary across regions. Relatively speaking, Jiangsu Province achieved much better control of the COVID-19 epidemic compared to its neighboring areas.
Changsha Shuangshu Technology, which specializes in intelligent surveillance of infectious diseases, aims to address the overarching challenges in infectious disease monitoring by resolving the pain points physicians face with current infectious disease reporting cards. Under the first-contact physician responsibility system, any physician who initially diagnoses a patient with a confirmed or suspected infectious disease, or identifies a pathogen carrier, is required to complete an Infectious Disease Report Card and maintain records for future reference.
Infectious disease surveillance imposes stringent requirements on the data quality of infectious disease report cards, with timeliness, completeness, and accuracy of reporting serving as key indicators. While this is a positive development, it has objectively led to numerous challenges for physicians during the actual process of completing infectious disease reports.
First is timeliness. Current regulations mandate that Class A infectious diseases must be reported within 2 hours, while Class B and Class C infectious diseases must be reported within 24 hours. However, completing the infectious disease report card requires considerable time for physicians. During periods of high patient volume, omissions are prone to occur, resulting in failure to report in a timely manner. This leads to delayed and underreported cases of infectious diseases.
Secondly, there is the issue of completeness and accuracy in infectious disease reporting data. Currently, most hospital registration systems lack complete patient information such as addresses and phone numbers, failing to meet the requirements for data completeness on infectious disease report cards. Physicians are forced to inquire about and enter this information on-site, a process that takes 3–5 minutes or even longer, causing significant inconvenience.
Whether physicians have sufficient awareness of infectious disease outbreaks also affects infectious disease surveillance. The infectious disease reporting forms on the direct reporting network for disease control and prevention include an option for “pneumonia of unknown etiology,” which could, in practice, correspond to early-stage COVID-19 cases with unclear diagnoses. In reality, however, physicians rarely select this option for reporting, as doing so entails completing a series of subsequent registration forms and investigations, imposing an additional burden on them. Alternatively, even if they are aware of this option, they may hesitate to report due to the lack of a definitive diagnosis or find themselves unable to submit reports under the existing system’s rules.
Currently, hospital infectious disease monitoring and reporting systems lack intelligence, clinical intervention protocols for physicians are insufficiently effective, and screening for delayed or missed reports by hospital infectious disease control departments is time-consuming and labor-intensive. These objective factors prevent infectious disease monitoring from completely eliminating delayed or missed reporting, representing key pain points in the field. Through extensive practical experience, Changsha Shuangshu Technology believes that these pain points can be addressed using big data.
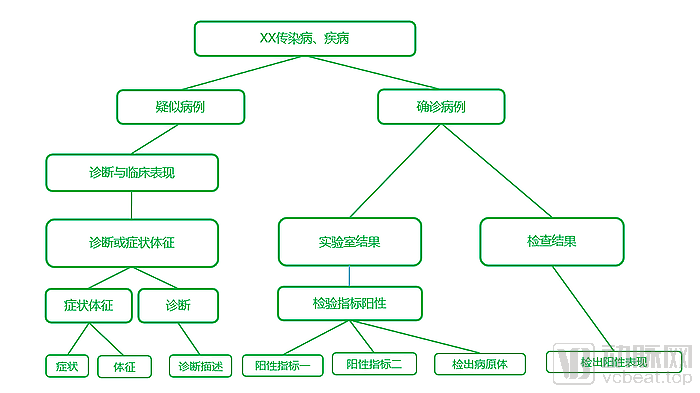
Operational Logic of Shuangshu Technology's Intelligent Infectious Disease Surveillance Solution
In Shuangshu Technology’s intelligent surveillance solution for infectious diseases, clinical data from four major systems—EMR, LIS, EMR, and PACS—are first aggregated. Then, leveraging Shuangshu’s expert knowledge base on infectious diseases and semantic analysis technologies, infectious disease-related features are extracted and labeled from the clinical data. Subsequently, an infectious disease analysis model is employed to analyze and compare these features, thereby enabling the identification of infectious diseases.
Upon identification of an infectious disease case, the system instantly or with a delayed push sends an alert to the specific physician’s workstation frontend and can forcibly lock the system, requiring the physician to complete the mandatory infectious disease report.
In practice, doctors did express some initial reservations due to unfamiliarity with the operation. However, during the process of filling out report cards, Dashu leveraged big data and artificial intelligence technologies to implement a series of optimization measures, including high-precision identification of infectious diseases, automatic prompts for pending report information, auto-filling of patient data, intelligent parsing and recognition of address information down to the street level, and automatic deduplication of duplicate reports. These enhancements significantly improved efficiency. Ultimately, doctors accepted and endorsed the system.
This intelligent infectious disease surveillance solution also shifts the control point forward, moving the validation logic from the direct reporting network for disease control entirely to the stage where physicians complete infectious disease reports. Reports cannot be submitted if they fail validation, thereby effectively addressing issues of completeness and accuracy in report cards.
After physicians complete the infectious disease report cards, those with complete and accurate data are reviewed by the hospital’s infectious disease reporting personnel before being submitted to the CDC’s direct reporting network, thereby also addressing the issue of timeliness.

Dual-Number Infectious Disease Surveillance Platform (All displays are for demonstration purposes only and do not represent any actual significance)
Building on the solution for physicians’ infectious disease reporting cards, Shuangshu Technology further implemented a one-click direct reporting function from hospital intranets to the CDC’s dedicated direct reporting network. In May 2017, Xiangya Hospital of Central South University utilized this system to achieve one-click direct reporting of infectious disease cards from its hospital intranet, completing the process in under three seconds. At that time, this was among the very few cases capable of enabling direct reporting from hospital intranets.
Currently, in addition to Xiangya Hospital of Central South University in Hunan Province, both the Children's Hospital of Chongqing Medical University and the Affiliated Hospital of Zunyi Medical University in Guizhou have adopted the one-click direct reporting solution via their internal networks.
According to statistics, the dual-data infectious disease surveillance system leveraging big data and artificial intelligence can achieve an effectiveness rate of over 95% in eliminating delayed and missed reports; it significantly reduces the average time physicians spend on completing infectious disease report cards from the previous 5–8 minutes to under 40 seconds; and the time required for direct reporting via the CDC’s dedicated network has also been shortened from 2–3 minutes to just a few seconds.
In fact, Zhongnan Hospital of Wuhan University also adopted Shuangshu’s infectious disease monitoring solution last year, demonstrating advantages in the efficiency of subsequent epidemic reporting. However, regarding early warning for sudden outbreaks of unknown infectious diseases, Shuangshu Technology believes that data analysis results from a single hospital are still relatively insufficient in terms of persuasiveness.
Relatively speaking, Shuangshu Technology believes that the integrated regional early warning and monitoring system for infectious disease outbreaks represents the optimal solution for addressing major regional infectious diseases. Currently, Shuangshu Technology has completed the research and development of this integrated regional early warning and monitoring system and is accelerating its deployment in other provinces and municipalities, aiming to explore new models for advancing China’s overall informatization of infectious disease control.
Do Not Overlook Rapid In-Hospital Data Collection; Big Data Operations Require Visualization
As the disease control reporting process has been streamlined, submitting disease control information has become much simpler. However, most hospitals struggle to gain a comprehensive overview of critical operational metrics, including the number of patients currently under care, the distribution of confirmed and suspected cases, staff-to-department ratios, shift schedules, and the status of personal protective equipment (PPE) supplies. Consequently, the outdated practice of printing Excel spreadsheets for manual data entry and statistical compilation has resurfaced.
Inefficient data workflows have imposed significant burdens and risks on frontline healthcare workers, while also preventing administrators from gaining a comprehensive overview. Department heads and hospital directors are unable to deploy resources rapidly, which has even disrupted routine staffing schedules. The approach taken by Dr. Zhang Wenhong, Director at Huashan Hospital in Shanghai, of having Communist Party members take the lead, was widely applauded; however, one underlying reason for this measure was likely that emergency conditions compromised ideal deployment protocols.
In reality, the vast majority of hospitals rely on vendor-provided services and lack the in-house capability to rapidly develop data acquisition and processing solutions. When confronted with unexpected situations that cannot be handled by these systems, health information technology infrastructure becomes merely ornamental. Under such circumstances, the resort to manual paper forms becomes understandable.
According to feedback obtained by FanRuan from hospitals, there were numerous data bottlenecks within hospitals during the pandemic, primarily categorized into three areas: micro-systems for data entry, automated reporting, and management-oriented data applications.
Micro-form reporting systems emerged as one of the most critical needs for hospitals during the pandemic. Although hospital information systems are already highly complex, their functionalities are primarily designed around routine hospital operations, with little additional data collection aimed at operational analytics. This gap has made it difficult to capture data required for ad-hoc requests. When vendor engineers are unable to provide timely on-site support due to unforeseen circumstances (such as a pandemic), hospitals are essentially left without recourse.
The primary purpose of the micro-system is to capture and store in a database certain data that hospitals might otherwise collect via Excel, as well as ad hoc or emergency data, for use in urgent situations—such as the temporary management of protective supplies during an epidemic.
The second requirement is automated reporting, aimed at freeing hospitals from complex and cumbersome reporting tasks. Meanwhile, automated reporting can be quickly adjusted and modified to align with each hospital’s specific circumstances. During the pandemic, automated reporting played a significant role in reducing the operational burden on hospitals.
Third is management-oriented data application. By collecting data from hospital EMR, HIS, and LIS systems and combining it with data collected through reporting micro-systems, it becomes convenient to provide hospital administrators with insights into the current operational status of the hospital and key areas for strategic focus.
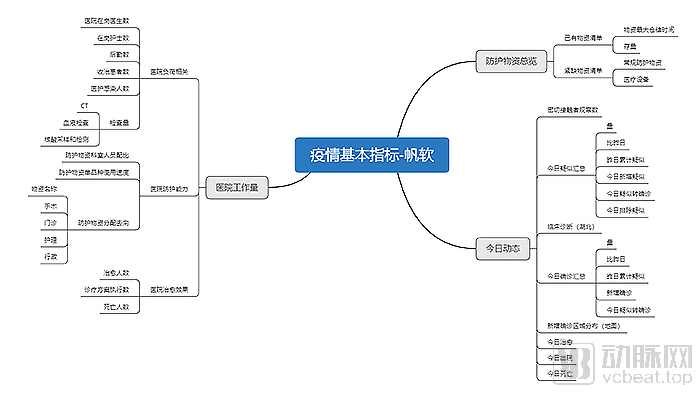
In this regard, Fanruan has summarized its long-term practical experience to provide hospitals with various templates for data entry micro-systems and automated reports. These include templates for multiple hospital operational metrics such as material handling, health status reporting, and remote work statistics. The solution enables the reporting of dozens of indicators across three key areas: hospital workload, overview of protective supplies, and epidemic dynamics, thereby addressing the urgent needs of hospitals.
When it comes to the application of big data, the promotion of most applications is inseparable from data visualization. In addition to conventional bar charts, line charts, and pie charts, epidemic maps have always been the most attention-grabbing component. This trend is not a recent phenomenon; as early as 1854, John Snow, a British anesthesiologist and epidemiologist, conducted research on the cholera outbreak in the Soho district of Westminster in western London, which is considered a pioneering study in the field of epidemiology.
At the time, knowledge about cholera was limited, and it was even believed to be airborne. John Snow recorded the number of deaths per household and marked them on a map. His analysis revealed that most cases were clustered around the Broad Street water pump. Combined with other evidence, Snow concluded that the outbreak was linked to contamination of the pump’s water supply. He subsequently had the pump handle removed, which helped bring the epidemic under control. This event led to the recognition that cholera is waterborne.
Although medical capabilities at the time were inadequate to cope with cholera, the use of data visualization enabled effective control of the epidemic. By correctly choosing maps over other types of charts, Snow made statistical analysis immediately clear and accessible. This exemplifies the power of data visualization.
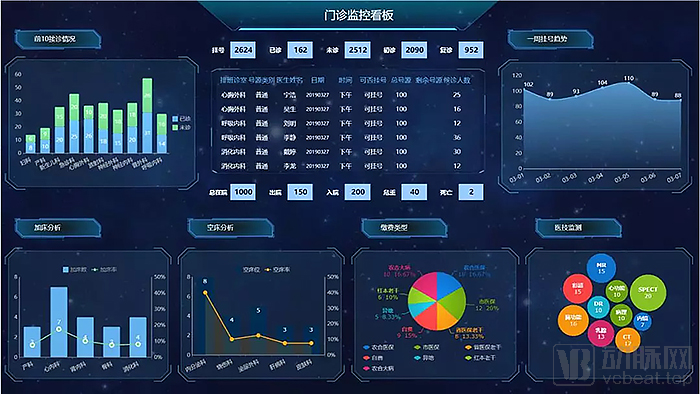
FanRuan's Outpatient Monitoring Dashboard (Image provided by FanRuan; for display purposes only and does not represent any actual significance)
Fanruan’s expertise in data visualization has also been leveraged in epidemic prevention and control. Its data reporting and visualization tools integrate data obtained from hospital information systems with data captured by micro-reporting systems, generating visualized dashboard displays. This enables hospital administrators to make timely and accurate decisions when confronted with complex data.
The emergency supplies management system, urgently launched by Beijing Dongruan Wanghai Technology Co., Ltd. on February 4, not only facilitated the matching of scarce supplies for 140 hospitals within less than 20 days but also conducted a statistical analysis of the overall supply status of hospitals across China through big data and data visualization.
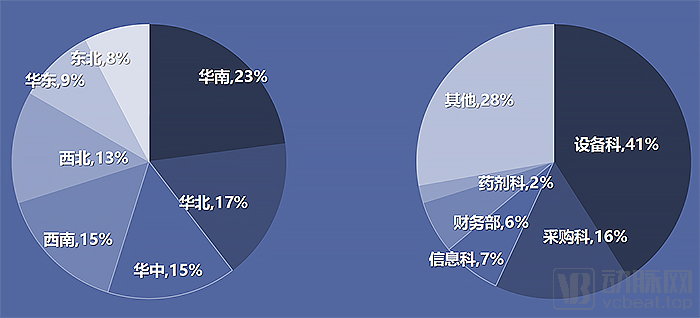
Registration Status of the Wanghai Kangxin Emergency Supplies Management System (as of February 23, 2020; image sourced from the Wanghai Kangxin HIA Data Platform)
Visual charts in the report released by the Wanghai Kangxin HIA Data Service Platform clearly reveal that the shortage of hospital supplies was not confined to Central China but was widespread across the country, as medical teams were dispatched from various regions to support Hubei Province.
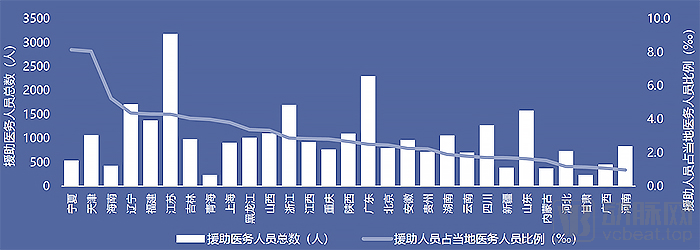
Overview of Medical Personnel Dispatched from Various Provinces and Cities to Aid Wuhan During the Epidemic (as of February 15, 2020; image source: Wanghai Kangxin HIA Data Platform)
The personnel deployment map also illustrates the support provided by medical systems across China to Hubei Province. Taking data as of February 15 as an example, Jiangsu Province dispatched a cumulative total of 3,182 medical personnel, the highest number at that time; however, this figure represented approximately 4% of its total medical workforce, demonstrating the province’s substantial medical resources. In contrast, the Ningxia Hui Autonomous Region dispatched a cumulative total of 536 medical personnel, accounting for 8.62% of its local medical workforce—the highest proportion at that time. Such visualized data plays a decisive role in enabling administrators to coordinate resources and make informed decisions.
Big Data Reconstructs the Full Picture of Urban Epidemics and Public Sentiment, Improving Epidemic Prevention and Control Processes
By integrating small-scale medical data with diverse big data sources, numerous practical data applications for epidemic control can be developed, such as queries for co-travelers on flights and trains, searches for confirmed cases in nearby communities, and national epidemic distribution maps. These represent the most intuitive and widely concerned data during this outbreak, in which many medical big data enterprises have played a significant role.
During the pandemic, big data platforms for COVID-19 surveillance, large-screen monitoring systems for fever clinics, and management platforms for individuals under medical observation for SARS-CoV-2 were established across various regions to provide epidemic analysis reports to the public and government authorities.
The epidemic monitoring platform leverages big data technology to construct dynamic heat maps of epidemic trends at the city and regional levels, facilitating the reconstruction of the entire course of urban outbreaks and the optimization of epidemic prevention and control processes. By employing intelligent analysis and prediction, it provides intuitive support for government decision-making, emergency management, resource allocation, and the assessment and forecasting of major events. This empowers decision-makers to understand the development and trends of emergency incidents within their jurisdictions based on key data and dynamic changes, enabling rapid and informed decision-making.
Most monitoring platform dashboards dynamically display the latest information, including changes in confirmed cases, cumulative cases by type, forecasts of confirmed case numbers, comparative analysis of epidemic development trends, the effective reproduction number (Rt), Rt trends, and cure rates. In regions with well-developed regional healthcare platforms, multi-dimensional dynamic supervision of local medical institutions can also be implemented.
The Fever Clinic Monitoring Dashboard can interface with fever clinics within the region, enabling real-time monitoring of hospital fever clinic operations via a large-screen display. It also provides risk early warning capabilities with pop-up alerts to ensure the safety of medical personnel.
Of course, the epidemic prevention and control command platform should not only focus on direct information related to the epidemic; public opinion should also be a key area of attention. In the early stages of this outbreak, various types of information were disseminated in a mixed manner, making it difficult for people to distinguish truth from falsehood. Some of this was unintentional misinformation, while other content consisted of malicious rumors. These messages occupied significant communication channels, causing genuine requests for help to be buried under spam.
To promptly identify and debunk rumors, thereby promoting the dissemination of truth and positive energy, the Qingbo Big Data Platform launched the “Epidemic Rumor Crusher” during the pandemic. This tool provides comprehensive access to rumor-refutation information verified by media outlets, professional institutions, and experts. It aims to supply the public with reliable fact-checking information, alleviating public doubt and panic.

Beijing Qingbo Big data Technology Co., Ltd. assisted the “Leihuo Research” volunteers in compiling more than 50 public opinion materials. Since January 30, it has daily compiled the “Compilation of Epidemic Public Opinion ✝ Leihuo Clarification,” with content selected from the latest news related to the epidemic on that day. The basic version had publicly released 32 issues by March 2, aiming to provide references for government and corporate decision-makers, media and internet reporters, and researchers at home and abroad.
Moreover, more importantly, big data technology enables the detection and extraction of help-seeking signals from subtle clues. During the pandemic, Beijing Qingbo Big Data Technology Co., Ltd. leveraged big data to mine and aggregate public opinion data, conducting research on the patterns and dissemination mechanisms of online help-seeking behaviors related to novel coronavirus pneumonia (COVID-19) across social media platforms, including Weibo, WeChat, Douyin, Kuaishou, forums, and Tieba.
By performing data cleaning, semantic analysis, and feature extraction on online help requests, unstructured text information is transformed into structured data. Leveraging indicator model design and strategy optimization, these requests are automatically classified into three categories—urgent (life-threatening), important (significant), and routine—for aggregation and referral to the relevant departments. Staff members then proceed with subsequent steps, including information verification, implementation of assistance, and post-assistance follow-up.
As of the afternoon of March 2, Qingbo assisted the “Leihuo Rescue” volunteers in collecting a total of 3,157 requests for help, conducted follow-up visits with 2,572 individuals through various means, and facilitated medical treatment for 1,693 people.
According to statistics from Qingbo Big Data, the overall public opinion trend during the epidemic followed a tortuous path in line with epidemic prevention and control measures, peaking on January 28. As effective containment measures were subsequently implemented, public attention gradually declined. It is worth noting that in an era where the internet and mobile internet are highly developed, some local executive departments at the district and county levels lack sufficient internet awareness and have paid relatively insufficient attention to online pleas for help posted on various digital platforms, indicating significant room for improvement.

Public Opinion Big Data by Qingbo Big Data (Image source: Qingbo Big Data; displayed for illustrative purposes only and does not represent any actual significance)
Therefore, Qingbo Big Data plans to continuously update the online help-seeking detection and mining system developed for the pandemic in the future, making it more universal and open to the public. It aims to provide technical support within its capacity for governments and society to respond to various disaster events. In addition to facilitating resource allocation by decision-makers, it also helps those seeking assistance to find nearby available resources for self-rescue.
Big Data + AI Empowers Pre-Consultation Screening, Bringing Peace of Mind to Patients and Healthcare Providers
This outbreak occurred during the winter season, a peak period for infectious diseases, and its early symptoms closely resembled those of influenza. This placed the much larger population of common flu patients in a dilemma: whereas they would previously have simply visited a hospital for a basic examination, they now hesitated to seek in-person care for fear of contracting COVID-19, yet worried about leaving potential cases unattended. In response to this need, many internet healthcare companies have launched remote outpatient services, pre-consultation screenings, and online self-diagnosis and triage systems.
Prior to the 2019 outbreak, Beijing Dashu Yida Technology Co., Ltd. developed the “Health Pass” APP for the Health Commission of Jiangsu Province. In addition to providing routine online remote consultations and triage services for medical inquiries, the company urgently launched an AI-based self-assessment feature during the pandemic, which was upgraded to specifically address the symptoms of COVID-19. This functionality played a significant role in Hubei Province, the epicenter of the outbreak.
As part of the national initiative to support Hubei Province, Jiangsu Province dispatched 732 physicians to aid Huangshi City. A remote online system was also deployed to facilitate telemedicine consultations for Huangshi residents, featuring a self-diagnosis module for common diseases powered by big data and artificial intelligence.
The online self-diagnosis and triage module provides a set of questions for initial symptom screening, converting them into micro-case records for each patient to assist remote physicians in conducting pre-consultation assessments. Before doctors in the corresponding departments open patients’ text-and-image or video consultations, artificial intelligence has already structured the dialogue, incorporating previously entered personal information—such as the patient’s age, height, weight, history of hypertension, and pregnancy status—and aggregating all this information directly.
Doctors can directly access patients' micro medical records during consultations, enabling them to ask more targeted follow-up questions based on their clinical judgment, which significantly improves the efficiency of the diagnostic process.
Meanwhile, by integrating various data platforms, once residents are identified as suspected or highly suspected cases by initial AI screening, the disease control departments will capture these data for analysis and sampling. By observing whether highly suspected cases are scattered across different locations or clustered in specific regions, analytical warnings and judgments can be made, effectively strengthening epidemic prevention and control measures in affected areas.
The internet hospital platform developed by Beijing Dashu Yida Technology Co., Ltd. for the Jiangsu Provincial Health Commission has successfully integrated with 68 internet hospitals and nearly 20 healthcare platforms in Jiangsu Province. As of February 12, the system had received hundreds of thousands of clicks for self-testing from residents and suspected patients. Daily API calls ranged from several hundred to several thousand, with a peak of over 7,000 calls in a single day.

Meanwhile, Beijing Dashu Yida Technology Co., Ltd. has also collaborated with partners to develop robots powered by 5G and artificial intelligence. These robots can conduct initial screening of febrile patients through questioning, perform vital sign measurements such as body temperature, blood pressure, and blood oxygen saturation, follow up with targeted questions based on the findings, and then triage the patients. In cases where there is a high suspicion of COVID-19, the hospital is notified for further management.
This intelligent robot underwent trial operations for nearly one month at two hospitals in Wuhan and Shanghai, respectively. At its peak, it performed over 360 initial screenings in a single day, significantly alleviating hospital pressure during the outbreak and reducing the risk of infection among healthcare workers.
Leveraging Big Data Thinking to Help Primary-Level Institutions Achieve Safe and Efficient Personnel Management
In addition to data from the healthcare system, data from outside the healthcare system—particularly frontline data from primary care communities—also played a significant role in epidemic prevention and control screening efforts.
However, the initial operational efficiency of grassroots screening was low. Many regions relied on paper-based reporting followed by manual entry into digital systems, which consumed considerable time and energy while yielding suboptimal results. This phenomenon of “fighting the epidemic through paperwork” indirectly exposed critical weaknesses in epidemic prevention and control, characterized by low efficiency and a lack of appropriate technical support. The issue of conflicting data from multiple sources was once particularly severe.
Over time, and under the guidance of central authorities, big data thinking and technologies have begun to be applied at the grassroots level.
As early as late January, Siming District in Xiamen City initiated epidemic prevention and control measures. Given the district’s limited administrative area and large population of non-local residents, the post-holiday return-to-work surge was anticipated to impose significant pressure on containment efforts. In response to the urgent need for coordinated joint prevention and control during public travel, the district government required a key-population health management platform that could be developed and rapidly deployed online within a short timeframe, thereby further enhancing the efficiency of grassroots community epidemic prevention and control work.
ZOENET HEALTH (hereinafter referred to as “ZOENET Health”) leveraged internet and cloud computing technologies to rapidly develop and launch the Huoshaoyun Health Management Platform. This is also Fujian Province’s first health management platform dedicated to key population groups.
By leveraging this platform, residents within the jurisdiction and returning individuals can submit personal health declarations, complete online information registration, and record their body temperature, thereby enhancing the efficiency of data collection for key populations under management. Enterprises in the area can register corporate information and record and track employee health data online, enabling timely awareness of employee status and assisting local government authorities in epidemic prevention and control efforts.

During the registration process, the platform allows a single account to register information for family members and select their jurisdictional affiliation, facilitating subsequent home visits by community personnel for follow-up. Meanwhile, upon learning of local epidemic-related clues, residents can report potential epidemic risks or violations in their vicinity—such as suspicious population movements, public gatherings, and the production or sale of counterfeit goods—to offline community health centers and sub-district offices. This assists in the timely identification of epidemic hazards and the curbing of violations such as price gouging, thereby enabling effective centralized management by the community.
To prevent underreporting, omissions, and oversights by grassroots staff, the health platform requires access to mobile device geolocation data during data entry, with on-site personnel required to take and retain photographic records. Meanwhile, adopting a big-data mindset at the data collection end, the platform strictly utilizes provincially unified forms for information submission to enhance data standardization, thereby supporting regional big-data platforms.
The platform is currently integrating online consultation services for fever clinics from local internet hospitals to reduce the risk of cross-infection during in-person visits.
When primary care physicians and community workers conduct offline screening and follow-up visits, they can use this platform to simultaneously collect information on tracked individuals and record body temperature, while providing real-time online tracking of vital signs. This liberates grassroots personnel from manual form-filling, effectively reducing their workload and enhancing the efficiency of epidemic prevention and control.
Meanwhile, the platform also provides back-end management functions, enabling government administrators at all levels and enterprises to perform personnel registration, data queries, and statistical analysis within the back-end system according to their respective access permissions.
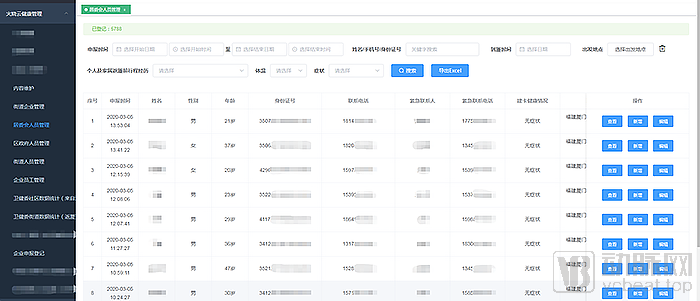
ZOENET HEALTH Huoshaoyun Health Management Platform (All displays are for demonstration purposes only and do not represent any actual significance)
Currently, the health management platform in Siming District has registered a total of 220,000 individuals, including 60,000 employees from 4,500 enterprises. By leveraging this platform, 6,000 individuals have been placed under priority management, which effectively alleviates the workload of grassroots personnel, enhances prevention and control efficiency, and thereby reduces local epidemic prevention risks.
Furthermore, the platform can provide individualized health management for students within the education system to address the surge in school resumption. Meanwhile, the platform is updating its features to enable subsequent functional iterations, such as automatic form filling via ID card scanning and facial recognition.
Wuhan, the epicenter of the outbreak, also implemented a similar close-contact management platform. As the epidemic’s ground zero, the city’s disease control efforts faced immense pressure, creating an urgent need to enhance operational efficiency through technological solutions. Like most other regions, Wuhan initially identified individuals who had close contact with confirmed patients (hereinafter referred to as “close contacts”) using primitive paper-based questionnaires, which were subsequently entered into computer systems.
This model is not only highly inefficient and error-prone but also suffers from prolonged data turnaround times. In Wuhan, every second wasted could potentially mean the risk of a clustered outbreak. To address this thorny issue, the Eru Research Team, which specializes in epidemiological investigation, customized an Electronic Data Capture (EDC) system for epidemiological surveys for the Wuhan Center for Disease Control and Prevention, and rapidly launched it within one week.

This system enables the management of local close contacts in Wuhan. Upon receiving the consolidated list of close contacts from the big data platform, the system imports the list into the close contact management system, stores it by district, and distributes relevant information according to community grid assignments. Frontline epidemiological investigators from the close contact teams can directly use the system on their mobile devices to conduct inquiries during door-to-door screenings.
Once the data is entered, it can be promptly uploaded to the Centers for Disease Control and Prevention (CDC), generating graphical interfaces and reports. This allows CDC personnel to view updated data in real time and conduct more intuitive and convenient analysis. The system has significantly improved the efficiency of circulating close-contact information at local CDCs and greatly reduced the reporting burden on grassroots community workers.
The actual workflow for reporting close contacts proceeds from community grid administrators to sub-district health service centers, then to district-level, municipal-level, and finally provincial-level Centers for Disease Control and Prevention (CDC). Personnel at each level require different reports and functionalities. To meet this need, the Eyou team rapidly developed customized reporting and data export features based on the existing system, generating reports strictly in accordance with data access permissions at each level, thereby maximizing reporting efficiency across all tiers of organizations.
Guided by big data thinking, the close contact tracking system incorporates a three-tier data filtering mechanism. First, standardized front-end data entry filters out unreasonable data at the source. Second, the Ewell team leverages its existing Ewell AI-powered data management system, which dynamically learns from the current data scope to automatically flag suspicious entries for correction. Finally, manual review is integrated, allowing for data sampling and approval to ensure the quality of extracted data, thereby supporting applications on the big data platform.

To date, the Yique EDC Close Contact Management Platform has covered all administrative districts and centralized quarantine sites in Wuhan. More than 700 CDC and community service personnel have used the platform, which has cumulatively managed data for over 80,000 close contacts. Meanwhile, local CDC authorities are applying to integrate with the resident identity system to achieve one-time data synchronization at the point of entry. This integration will link all relevant data—including close contact records, epidemiological investigation details, residential information, and social relationships—thereby maximizing the value of the data.
Big Data Development: Do Not Let the Original Intent of Breaking Down "Information Silos" Turn Into Creating More "Information Silos"
The fact is that, amid the vigorous development of health informatization in recent years, the progress of public health informatization has significantly lagged behind. The dedicated network for direct reporting by disease control and prevention agencies remains largely limited to the reporting of various infectious diseases. Access permissions are basically retained at the national level, preventing provincial, municipal, and county authorities from utilizing the data to generate timely and effective analytical insights.
Meanwhile, the information systems for disease surveillance, vaccination, and health emergency management handled by CDCs at all levels have not yet been interconnected.
Despite widespread investments in establishing big data platforms, the National Basic Health Information System and the information systems of disease control and prevention institutions are currently moving in opposite directions. These systems are being developed separately in terms of basic data collection, entry, standard application, and administrative management, failing to establish a unified and efficient public health information platform. As a result, much of the data cannot be effectively utilized.
Frankly speaking, various departments and regions are operating in silos. Without top-level coordinated design and promotion, the original intention of eliminating “information silos” may, in the future, inadvertently create even more “information silos.”
To address this potential issue, industry experts agree that it is necessary to establish unified planning and standardized frameworks for big data infrastructure. This will enable effective interoperability among different platforms and prevent the creation of additional “information silos.” Meanwhile, greater attention should be paid to the effective operationalization of data, ensuring that applications are implemented in specific business scenarios. Otherwise, the big data collected through considerable effort may become large yet useless, thereby negating its intended value.
Final Thoughts
We must clearly recognize that, despite the notable achievements in the fight against the epidemic and the booming application of “Internet Plus” and big data, shortcomings have been exposed, highlighting an urgent need to enhance the informatization level of China’s disease control and prevention system.
In the article “Reflections and Recommendations on the Modernization of the Disease Prevention and Control System,” multiple experts from the Expert Group on Novel Coronavirus Pneumonia Prevention and Control of the Chinese Preventive Medicine Association jointly pointed out that public health big data and information systems are an important component of the modernization of the disease prevention and control system, as well as a key means and foundation for enhancing public health service capabilities.
In the future, we should build upon the national infrastructure for public health informatization, leverage the reform and improvement of the public health service system, and deeply integrate medical services with foundational public health information. By employing technologies such as blockchain, big data, artificial intelligence, cloud computing, and the Internet of Things (IoT), and closely focusing on the “Precision Multi-Dimensional Big Data Real-Time Collection System,” the “AI Deep Learning System for Disease Surveillance and Epidemiological Patterns,” the “Big Data and Cloud Computing Intelligent Early Warning and Prediction System,” and the “Unified Resource Management and Allocation System for Emergency Support,” we will play a critical supporting role in routine surveillance, epidemic early warning and response, trend forecasting and assessment, source tracing of infectious agents, resource allocation, and prevention and control treatment.
Relying on the National Population Health Information Platform, and based on electronic medical records, health archives, and the national population database, supported by information security, standard specifications, and operation and maintenance assurance systems, we will improve and perfect a nationwide network system for epidemic reporting, monitoring, early warning, and public health emergencies. We will build a public health cloud platform and disease control business application systems to realize a series of platform-based business applications, including dynamic disease monitoring, early warning, and response; full-process management of childhood vaccination; monitoring and evaluation of health hazard factors; occupational health; maternal and child health care; and comprehensive supervision services.
By leveraging the public health cloud platform, we will establish public-facing public health information services, enabling citizens to truly experience the convenience brought by informatization, thereby enhancing the timeliness, accessibility, and equity of public health services and improving public satisfaction.
We extend our gratitude to the following guests for accepting our interviews and providing relevant information (listed in no particular order): Zheng Wei, FanRuan Data Application Research Institute; Li Shiyong, Founder and General Manager of Changsha Shuangshu Technology Co., Ltd.; Miao Miao, Chief Operating Officer of Beijing Dashu Yida Technology Co., Ltd.; Zhao Guang, CEO of Ewin Research; Zhuang Chengbin, Development Director at ZOENET HEALTH; Yu Tong, Director of Branding and Marketing at Beijing Dongruan Wanghai Technology Co., Ltd.; and Liu Chunyang, Assistant to the President of Beijing Qingbo Big data Technology Co., Ltd.
References:
Caixin: Timeline of the Novel Coronavirus Pneumonia Outbreak in Wuhan
Finance: Who Was the First COVID-19 Patient Identified Through Genetic Testing?
Finance: The Direct Online Reporting System for Infectious Diseases Cost 730 Million Yuan to Build. Why Did It Fail for 28 Days?
Chinese Journal of Epidemiology: Reflections and Recommendations on the Modernization of the Disease Prevention and Control System