Accelerating NMPA Class III Certification: How AI Imaging Leveraged Pandemic Response Value to Fast-Track Regulatory Approval
Amid the Widespread Epidemic, Plans Come First.
As early as February 10, the Secretariat of the National Artificial Intelligence Standardization General Group (China Electronics Standardization Institute) compiled the first batch of 34 AI products and solutions to aid epidemic prevention and control. These solutions broadly covered five sectors: intelligent recognition, intelligent interaction, intelligent healthcare, intelligent mobility, and remote services.
Among these, the intelligent healthcare sector accounted for the largest number of projects, with a total of 13. Leading companies are involved in every segment, ranging from imaging diagnostics to drug R&D. Meanwhile, intelligent healthcare is the sector closest to the front lines of epidemic prevention and control: AI-powered imaging diagnostics help alleviate the burden on physicians, while AI-driven drug discovery efforts test viral targets to facilitate drug repurposing.
Unlike usual, a common issue persists whether it involves repurposing existing drugs or employing AI-based imaging diagnostic software for COVID-19: although relevant authorities take the lead, there is a lack of clear approval procedures.
Not until March 5 did the regulatory framework for software related to novel coronavirus pneumonia finally arrive. The National Medical Products Administration (NMPA) stated that, in response to the COVID-19 outbreak, and in accordance with the principles of scientific review and the requirements for ensuring product safety, efficacy, and quality controllability, the NMPA and the Center for Medical Device Evaluation issued the “Key Points for the Review of CT Imaging-Assisted Triage and Assessment Software for Pneumonia (Trial)” (hereinafter referred to as the “Key Points”). With this development, medical AI-assisted diagnostic software has finally been brought onto the right track in terms of safety validation.
“Key Points” outlines the approval process for AI software during the pandemic across seven aspects: scope of application, basic requirements, risk management, software research, clinical studies, labeling, and considerations for software updates. Through an analysis of the document, VCBeat has identified the following four keywords.
Keyword 1: Class III Medical Device Certificate
The first part of the document initially clarifies the scope of review, stating: “According to the current Medical Device Classification Catalogue, this product is classified under code 21-04-02 and falls within Class III for regulatory purposes.”
It is worth noting that, based on the AI approval landscape in 2020, only Keya Medical’s FFRCT and Lepu Medical’s ECG analysis software obtained Class III medical device certifications for AI-based devices. In CT imaging applications such as those for the lungs and liver, no company has yet completed the full regulatory approval process through standard procedures. As of March 2020, some AI medical imaging companies stated that they had completed clinical trials and were on track to obtain Class III certifications in 2020.
Thus, this policy may signal a further acceleration of the approval process for Class III AI medical device registrations. From another perspective, it also indicates that the industry has, to some extent, recognized the role played by AI-assisted diagnostic software during the pandemic.
Keyword 2: Functional Requirements
The text states: “Software functions must include, at a minimum, anomaly detection, quantitative analysis (e.g., lesion volume proportion, CT value distribution), data comparison (both manual and automated), and report generation. Among these, anomaly detection serves to provide triage alerts for suspected patients, while quantitative analysis and data comparison are used for disease assessment in confirmed cases.”
Generally, the primary responsibilities of AI in hospitals are to improve physician efficiency and enhance diagnostic accuracy. However, in this passage, the Center for Medical Device Evaluation explicitly mentions functions such as “quantitative analysis” and “report generation.” This implies that AI software must not only provide highly accurate judgments but also present corresponding supporting evidence, thereby possessing capabilities for data analysis and processing.
Meanwhile, as the approval of Class III medical devices requires demonstrations of “non-inferiority” and “superiority,” the current COVID-19 pandemic undoubtedly presents AI companies with an excellent opportunity to design clinical trials. If deep learning can meet these product requirements by performing quantitative analyses that are difficult for traditional analytical software to achieve, and if clinical trial designs are centered on “AI triage” and “full-data learning,” the approval process for AI products is likely to be accelerated.
Keyword 3: Data Requirements
For AI approval, this document provides numerous explicit requirements, which can be summarized as follows:
1. The training data shall, in principle, include no fewer than 2,000 CT images of COVID-19 cases; these images must be sourced from at least three medical institutions, including at least one institution located in an area severely affected by the epidemic; and they must encompass CT images from both the early and progressive stages of novel coronavirus pneumonia.
2. Provide the data distribution of CT images for novel coronavirus pneumonia by integrating factors such as population characteristics (e.g., sex, age), imaging stages (early, progressive, and severe phases), data source institutions, and CT equipment specifications (e.g., manufacturer, slice thickness).
3. Provide an analysis report on factors affecting algorithm performance, incorporating CT equipment, imaging-based staging, and similar clinical presentations.
Based on the above three points, obtaining Class III medical device certification through the “Key Points” remains challenging. As of March 6, there were a total of 80,714 confirmed cases (with 67,592 in Hubei Province), and many provinces and municipalities had not yet exceeded 2,000 confirmed cases. For non-first-tier AI companies, it is difficult to meet the “2,000 cases” threshold if their products have not been deployed in cities heavily affected by the epidemic, or if they have been deployed but lack sufficient validation and usage data.
Keyword 4: Clinical Trial Design
The "Key Points" indicate that companies may adopt a single-arm target value trial design, using inherent diagnostic accuracy metrics such as the sensitivity and specificity of triage alerts as primary evaluation endpoints. This approach differs from standard procedures.
Manufacturers shall provide a detailed description of the selection, construction methodology, and rationale for the gold standard. Available methods for constructing the gold standard include: (1) using clinically confirmed results as the gold standard, i.e., comprehensive diagnostic outcomes based on epidemiological history and clinical manifestations (including imaging features); and (2) establishing the gold standard through an expert image review panel.
Furthermore, the "Key Points" also propose sample size estimation metrics that need to be clarified under various scenarios. These provisions provide clear guidelines for enterprises in formulating clinical trial plans.
Overall, the COVID-19 pandemic has drawn greater attention to AI-assisted diagnostic technologies due to emerging clinical needs. However, whether products can secure timely approval under this regulatory framework will depend on close collaboration between enterprises and the Center for Medical Device Evaluation (CMDE) to advance the development of AI.
In addition to developments in domestic AI review and approval, overseas CE marking has also made progress.
In February 2020, AI products from companies such as Infervision and Zhiyuan Huitu successively obtained EU CE certification, enabling them to expand into the European market. Furthermore, insights from numerous review and approval meetings indicate that Chinese regulatory authorities also place significant emphasis on the U.S. FDA’s perspectives regarding AI-assisted diagnostic medical devices, aiming to identify aspects suitable for adaptation to China’s specific national context.
Slightly different from the approach in China, the FDA generally conducts review and regulation of different products based on risk, classifying them into Class I, II, and III. Generally speaking, imaging products fall under Class II, while invasive products are categorized as Class III. Depending on whether there are existing predicate devices for comparison and whether the specific risks are sufficiently understood and controllable, approvals for Class II devices are further divided into pathways such as De Novo, 510(k), and PMA.
With the continuous application of new technologies such as artificial intelligence (AI) and machine learning, the FDA’s review standards for Computer-Aided Detection/Diagnosis (CAD) software have evolved accordingly. From 1998 to 2017, regulatory oversight of CAD software remained relatively traditional, relying on the Premarket Approval (PMA) pathway. Between 2017 and 2020, as understanding of these applications deepened, the De Novo classification request pathway was adopted instead. The De Novo pathway not only permits marketing of the device in the U.S. market but also establishes a new regulatory classification, enabling subsequent substantially equivalent devices to submit premarket notifications via the 510(k) pathway under this newly established classification.
Based on the 2019 approval landscape, AI products from companies such as GE and Subtle Medical have all secured regulatory clearance through the 510(k) pathway. Subtle Medical’s two FDA-cleared products centered on image reconstruction—SubtlePET and SubtleMR—were both applied for and approved via the 510(k) route.
On February 7, 2020, Caption Health received FDA clearance to market its AI-powered echocardiography acquisition application, which the FDA classified as a new type of Computer-Assisted Device (CAD)—specifically, CADa/o (Computer-Aided Acquisition/Optimization). This marks another regulatory innovation by the FDA.
Therefore, the introduction of this policy can also be regarded as an innovative attempt by China’s regulatory system in the review and approval process. In the face of emergencies, specific measures may be needed to support the development of medical technology.
However, some argue that regardless of how the approval process evolves, “a certificate is ultimately just a piece of paper.” Whether an AI solution can survive in the market and gain acceptance among physicians hinges fundamentally on the intrinsic value of the artificial intelligence itself. Meanwhile, it is precisely because AI has demonstrated unexpected value during the pandemic that regulatory policies have been advancing accordingly.
According to Director Liu Shiyuan’s summary, the role of medical imaging AI during this epidemic can be categorized into four aspects:“First, detect lesions, and confirm and segment them; second, diagnose and differentiate lesions by measuring data such as their distribution, morphology, and density; third, assess lesion progression and outcomes through AI-based quantification and grading to determine whether the condition is deteriorating or improving; fourth, integrate clinical laboratory tests and leverage full-data learning to transition from qualitative to quantitative analysis, thereby developing precise algorithmic models and ultimately achieving personalized precision medicine.”
The first three functions can be regarded as the foundational roles of artificial intelligence in this epidemic prevention and control campaign. For many frontline doctors in Wuhan, the ability to interpret patients’ CT images with greater efficiency and diagnostic accuracy would undoubtedly help alleviate the backlog of imaging studies and reduce missed diagnoses. Meanwhile, AI applied to digital radiography (DR) can address the shortage of specialized radiologists in primary healthcare settings, where it is often difficult to evaluate suspicious findings. Furthermore, follow-up functionalities enable physicians to rapidly quantify changes in patients’ conditions, thereby facilitating subsequent clinical decision-making.
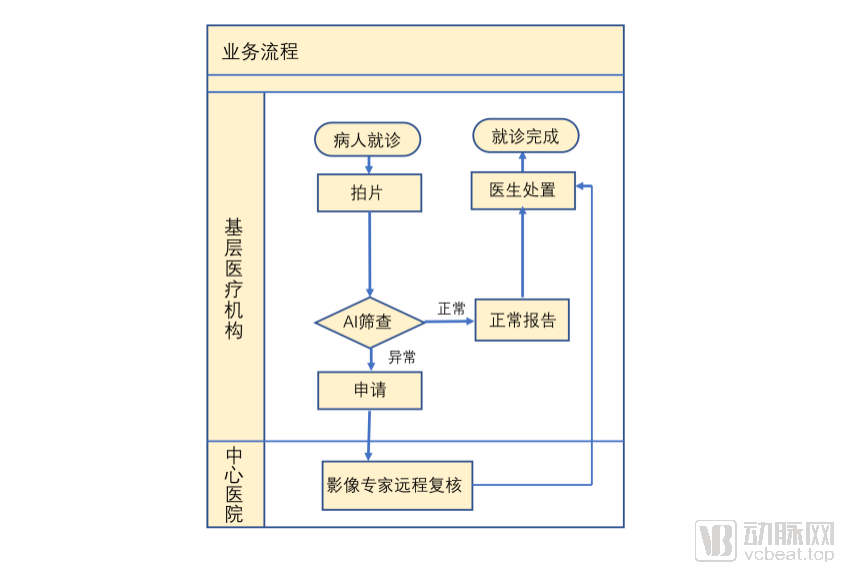
Nearly 30 AI companies developed “AI+CT” solutions for this epidemic. Each company played a role in “improving efficiency and reducing omissions,” yet their approaches varied. Taking Huiyi Huiying’s “triune” smart imaging solution as an example, the company enabled direct frontline deployment through remote installation of its integrated services: “AI-assisted screening, intelligent digital film, and intelligent remote consultation.” Leveraging deep learning algorithms, the solution can diagnose 500 CT images within 2–3 seconds, generate structured text-and-image reports with a single click, and store data in the cloud to create personalized health records for patients, facilitating self-access and follow-up care. Furthermore, intelligent remote consultation enhanced overall resource allocation capabilities for societal epidemic prevention and control. Additionally, Yitu Healthcare launched its AI+CT imaging auxiliary diagnosis product within just one week after the Spring Festival, and it was widely adopted across China, including in Wuhan.
Compared with CT, DR has certain limitations in terms of resolution and image clarity; however, these factors do not hinder radiologists from diagnosing COVID-19. Furthermore, due to its low cost (equipment priced under several hundred thousand yuan, and examination fees ranging from 60 to 80 yuan), many townships without CT scanners have still equipped themselves with a certain number of DR units. Such imaging equipment has also been widely utilized in epidemic areas.
Taking Jiufeng Medical’s AI-based intelligent screening system for viral pneumonia (including COVID-19) using chest X-rays as an example, the system can be deployed in primary healthcare settings either via mobile imaging vehicles or through remote deployment, or it can be installed within imaging centers of medical consortia and medical alliances. It leverages AI technology to efficiently process digital radiography (DR) images. By the end of February 2020, Jiufeng Medical had helped approximately 300 primary township health centers deploy its Jiufeng Intelligent Image Reading System, screening 15,000 individuals. Among these, about 15% (in areas outside Hubei Province) and 20% (in Hubei Province) of the chest X-rays were identified by AI as indicative of viral pneumonia. Following expert review, a total of 84 suspected cases of COVID-19 among primary-care patients were identified.
The aforementioned three functions are not only applicable to radiology departments during the COVID-19 pandemic but also help alleviate the workload of physicians at hospitals of all levels in routine practice, thereby demonstrating their “universal” applicability. Meanwhile, due to the unique circumstances of the pandemic, certain specialized roles of AI have become particularly prominent.
During the peak of the Wuhan epidemic, intensive care beds in the city were often in short supply, and makeshift hospitals used for isolating patients with mild to moderate symptoms were also overcrowded, leaving many patients waiting for beds outside of hospitals. Patients admitted to makeshift hospitals typically required physicians to assess the severity of their condition in advance, followed by re-evaluations at intervals of 3–5 days.
At this critical juncture, physicians must make precise assessments of patients within a very short timeframe and triage them to the hospitals best suited for their specific conditions. For patients who have already been admitted, doctors are also required to conduct regular follow-ups, monitoring changes in ground-glass opacities on imaging studies across different stages of the disease. Treatment plans must be promptly updated for patients whose symptoms worsen, while those showing improvement or recovery should be transferred accordingly. These challenges have created new demands for medical AI: to assist physicians in qualitatively characterizing patients’ conditions and determining the stage of disease progression based on quantitative analysis. Although this was not an intentional strategy by AI companies, such applications were widely adopted during the pandemic.
Secondly, generally speaking, physicians cannot directly differentiate the type of pneumonia a patient has based solely on CT findings. However, some companies are striving to use digital methods to quantify the radiological features of novel coronavirus pneumonia, thereby enabling direct determination of the pneumonia type. Currently, many physicians are leveraging AI and have published relevant papers through retrospective studies; yet, moving from research to robust validation, we may not obtain definitive answers before the epidemic ends.
Compared with the “universal” role, the aforementioned two roles have certain limitations; that is, AI played a corresponding role due to the occurrence of the COVID-19 pandemic, and its characteristic lies in the non-replicability of its functions.For example, if the novel coronavirus were not highly contagious, makeshift hospitals would not have emerged, and there would naturally be no need for triage; the same logic applies to scientific research. However, the approach of conducting analysis through data may harbor deeper value in AI.

AI Companies Developing Imaging-Related Applications During the Pandemic (Incomplete Statistics)
Regarding the question, “What is the potential value of AI?” a physician stated, “In general, radiologists tend to issue diagnoses of ‘space-occupying lesions’ rather than specifically diagnosing pneumonia. However, for patients, the term ‘space-occupying lesion’ is overly broad; they require more precise diagnostic conclusions, which are rarely provided by radiology departments at present. Currently, many AI applications are engaged in quantitative data analysis, but this is not where AI’s true strength lies—conventional data processing software can also collect and mine data. Therefore, for AI to realize its genuine value, it must leverage quantitative data to deliver qualitative diagnostic judgments.”
From the current perspective, fully allowing artificial intelligence to make decisions without referencing doctors' opinions violates AI ethics. However, by developing AI-based imaging auxiliary diagnostic algorithms for pneumonia, companies are indirectly addressing the issue of direct decision-making by enhancing physicians' diagnostic capabilities.
Taking United Imaging Intelligence’s research in this area as an example, its AI-assisted analysis system can segment the lungs into distinct pulmonary segments, delineate lesions within them, and calculate the infection ratio for each segmental lesion area, thereby providing reference data for diagnosing infections. Due to the rigorous standards of clinical diagnosis, these achievements may not immediately assist physicians in practical diagnostic settings in the short term; however, they do offer valuable insights for understanding the novel coronavirus.
Extending from the perspective of differentiating pneumonia types, some enterprises are attempting to combine imaging data with data from other departments to establish comprehensive AI models, providing physicians with more holistic reference information.
For example, Ande Medical Intelligence holds that it is difficult to differentiate various types of pneumonia solely based on radiological images, whereas etiological diagnosis serves as the gold standard for definitive diagnosis. Therefore, while studying CT imaging, Ande Medical Intelligence attempted to construct AI training datasets anchored by the gold standards of etiological diagnoses and positive nucleic acid test results for various pneumonias, thereby enabling the classification of pneumonia into bacterial, fungal, COVID-19, or other viral types.
GE Healthcare has chosen to integrate radiogenomics, artificial intelligence, and image processing technologies. On March 5, GE Healthcare launched the “Smart Win COVID-19 LK 2.0” AI platform, which aims to enable earlier lesion detection and more precise quantitative analysis of pulmonary nodules, lung inflammation, and impaired lung function. On one hand, the platform provides AI-assisted diagnostic capabilities to help physicians process medical images; on the other hand, it supports research into the early identification of COVID-19 in CT scans.
Zhao Zhoushe, Vice Dean of the Precision Medicine Institute at GE Healthcare China, stated: “We first preprocess all data uploaded to the platform, standardizing images from any scanner model to a uniform slice thickness of 1 mm. Subsequently, we apply algorithms to these standardized images to segment and annotate the lungs, trachea, and bronchi. At this stage, we can identify lesions; using appropriate models, we are able to determine whether a patient has COVID-19 and provide a probabilistic assessment.”
Specifically, the LK2.0 AI platform provides three types of personalized processing based on the stage of COVID-19 lesion development.
For early-stage asymptomatic patients and subtle COVID-19 lesions that are difficult to detect, GE Healthcare has expanded the scope of its AI analysis to include the trachea and bronchi, facilitating the early identification of lesions in cases with no significant morphological changes in the lungs.
For complex lesions in the middle and late stages of COVID-19, the LK platform enables rapid, intelligent segmentation of lung lobes, precise localization of lesions, and quantitative scoring. By integrating AI-driven deep learning modeling, it further assesses disease progression, reflects lesion volume and distribution, analyzes diffuse lesions, and predicts disease trajectory.
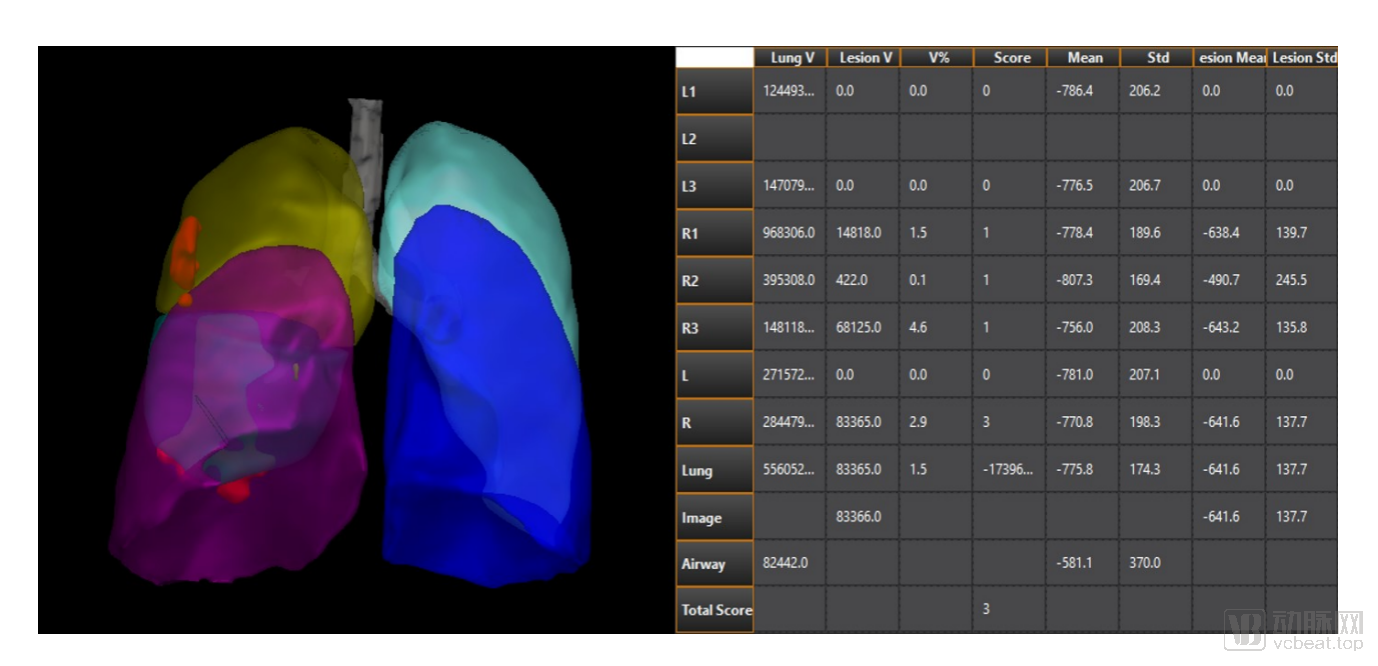
Segmentation of Complex Lesions in the Mid-to-Late Stages of COVID-19: 3D Visualization of Lesions (Red Areas) and Quantitative and Scoring Analysis
In response to the surge in COVID-19 patient data, the LK platform can standardize data from different models of CT scanners and perform rapid batch image interpretation.
However, segmentation, localization, and scoring are only one of the methods for assessing pneumonia. Xu Haibo, Director of the Department of Radiology at Zhongnan Hospital of Wuhan University, stated, “There are numerous imaging data parameters associated with COVID-19, many of which have not yet been fully integrated. This is one of the key areas we will focus on in our future collaboration with GE Healthcare. Currently, segmentation and annotation technologies are highly mature; they can help prevent missed lesions due to physician fatigue and generate templates for structured reports, reaching a level suitable for clinical deployment. Nevertheless, achieving highly intelligent and precise diagnosis still requires extensive reference matching and prolonged clinical validation.”
Overall, the relationship between the regulatory review and approval of imaging AI and its value can be described as mutually reinforcing. The expansion of AI’s value has accelerated the pace and heightened the necessity of regulatory review and approval, while such regulatory processes have procedurally paved the way for the development of imaging AI.
Although the outbreak of the COVID-19 pandemic temporarily delayed the review and approval processes for certain artificial intelligence products in the short term, it also demonstrated new value to the public.
So, can Class III certification for AI medical devices be granted under the “Key Points”? Based on the approval trends over the past two years, VCBeat believes that this will still depend on the enterprises themselves. If companies are sufficiently proactive, we expect to see AI firms obtain Class III certificates for CT lung-related products through the “Key Points” within the next three months.
But regardless of whether certification was obtained, AI demonstrated its inherent value during the pandemic. What can AI do in the future? Doctors now have new expectations...