Six Emerging Opportunities for Domestic Medical IT Suppliers in the Post-Pandemic Era
After nearly two months of intense efforts, the COVID-19 epidemic in China has finally been brought under effective control. The makeshift hospitals that have ceased operations and closed their doors stand as the most profound medals for these healthcare workers who marched against the tide, much like the pressure marks left on their faces by protective equipment. If we were to take stock of the deep impressions left on ordinary people by this epidemic, apart from short videos featuring newly crowned “kitchen kings,” it would likely be the epidemic maps and daily updates that became part of our daily routine.
On January 20, DXY launched its “Epidemic Map” product, which has since garnered billions of views. Subsequently, real-time epidemic updates rapidly became a standard feature across major internet platforms, with Tencent WeChat, Alibaba Alipay, JD Health, Chunyu Doctor, and others rolling out their own epidemic data products.
Compared with the single information sources such as television and newspapers during the 2003 SARS outbreak, people can now access information through more diverse mobile channels, thanks to the construction and public availability of regional health information platforms in recent years. For example, ZHEJIANG MEDIINFO I.T.CO.,LTD, a medical IT enterprise headquartered in Hangzhou, Zhejiang Province, promptly launched a COVID-19 reporting and monitoring system for the Jiangxi Provincial Health Commission at the onset of the pandemic. The company provided epidemic data to the Jiangxi Provincial Epidemic Prevention and Control Command Center, supported the entire process of epidemic trend monitoring and analysis, and played a positive role in containing the outbreak across the province.
Furthermore, VCBeat’s research has found that the majority of provincial, sub-provincial, and prefecture-level governments across China have promptly made available on their open data platforms data that is accessible, complete, fine-grained, timely, machine-readable, and structured. While the number and structure of datasets vary across platforms, these data sets, which meet basic development standards, have laid the groundwork for a series of big data-driven intelligent applications during the pandemic, such as the Health Code first launched in Hangzhou.
In fact, every public health emergency since the turn of the new millennium has driven leapfrog development in the informatization of population health.
For example, in the aftermath of the 2003 SARS outbreak, China launched its first wave of regional health informatization initiatives. In 2004, the former Ministry of Health initiated the development of the Standards for Classification of Public Health Information and Basic Data Sets in China and the Standards for Basic Hospital Data Sets, marking the inception of regional health informatization construction in China.
Furthermore, following the 2009 H1N1 pandemic, the Ministry of Finance and the National Development and Reform Commission consecutively launched multiple health informatics projects funded by central fiscal transfers in 2010. These initiatives mandated pilot programs at the provincial level to establish provincial regional health informatics platforms, as well as repositories for personal health records and electronic medical records, thereby laying the foundation for the development of a three-tier platform system encompassing national, provincial, and municipal levels. To date, China has essentially achieved comprehensive coverage of its regional health informatics systems, marking a transition from non-existence to widespread implementation.
By September 2013, the National Health and Family Planning Commission and the State Administration of Traditional Chinese Medicine jointly issued the “Guiding Opinions on Accelerating the Development of Population Health Informatics” (hereinafter referred to as the “Guiding Opinions”), which formally proposed the top-level design for guiding healthcare informatization construction in the subsequent years, namely the “46312 Project.”。
Specifically, the "Guiding Opinions" require that, while ensuring the continuity of existing health informatization and population and family planning informatization efforts, a comprehensive population health informatization project be systematically developed. This project is based on three major databases—comprehensive population information, electronic health records, and electronic medical records; focuses on six key business applications—public health, family planning, medical services, medical security, drug management, and comprehensive management; relies on four-tier population health information platforms at the national, provincial, municipal, and county levels as hubs; uses resident health cards as the carrier; is supported by information standards and security systems; and emphasizes interoperability, data sharing, and business collaboration as its core elements.
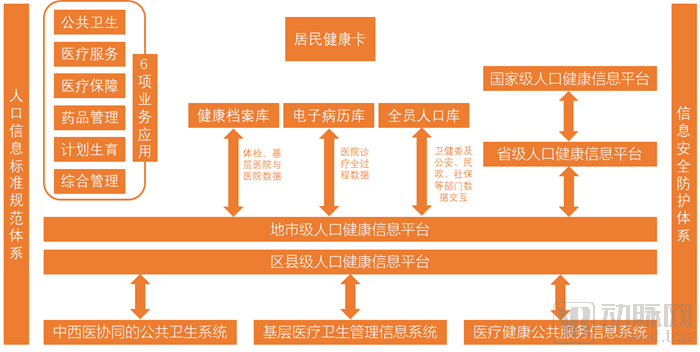
Population Health Information NetworkSource: VCBeat, compiled from public information
The “13th Five-Year Plan” for National Population Health Informatization Development, released in 2017, set the tone for the development goals of population health information platforms: unified authority and interoperability.
During this period, a large number of healthcare IT vendors that undertook the construction of most foundational databases and linkage platforms emerged one after another, giving rise to a healthcare IT market valued at hundreds of billions.
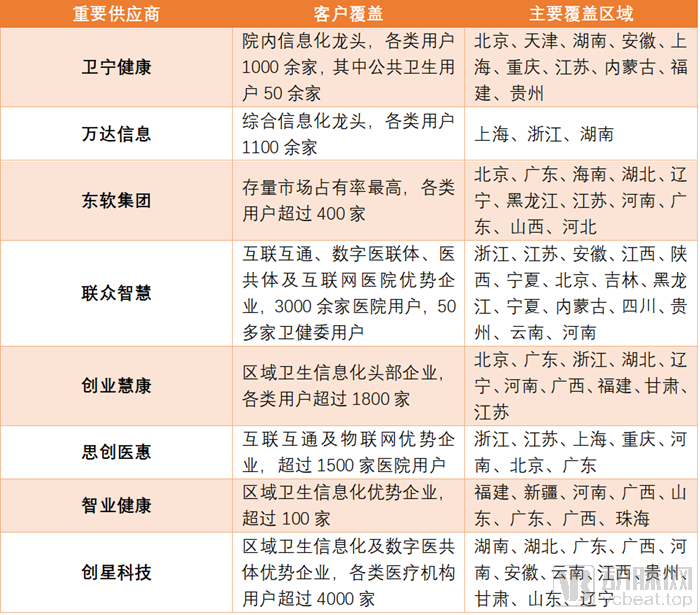
Major Domestic Medical IT VendorsData Source: Compiled by VCBeat from public sources including research reports and official websites
Based on past experience, the COVID-19 outbreak in early 2020 is highly likely to serve as a catalyst for deepening healthcare reform, thereby creating new growth opportunities for medical IT companies that are transitioning from a period of rapid, unregulated expansion to a more stable phase of development.
1. Internet Hospital
The implementation of internet healthcare applications may become the first direction in which the COVID-19 pandemic boosts medical IT enterprises' new infrastructure development.
During the pandemic, hospitals became high-risk areas for cross-infection due to the highly contagious nature of the COVID-19 virus. Patients with minor ailments, such as the common cold, adopted online consultations and home delivery of medications for diagnosis and treatment, thereby reducing exposure associated with hospital visits and lowering the risk of infection. On the other hand, the surge in patient numbers overwhelmed major hospitals in many regions, including Wuhan. The use of internet-based healthcare services by patients with mild symptoms also effectively alleviated the pressure on hospital outpatient services.
Since January this year, the construction of internet hospitals by hospital institutions has reached a climax, with physical hospitals of all levels across China launching online consultation services. During the epidemic, ZHEJIANG MEDIINFO I.T.CO.,LTD joined forces with Ping An Good Doctor to launch internet hospital services in dozens of physical hospitals across nine provinces, including Zhejiang, Jiangsu, and Shaanxi.
Typically, internet healthcare unbundles the previously integrated hospital-based disease treatment into several digitizable components. The three typical components are online consultation, e-prescribing, and medication review and delivery, which constitute the primary battleground for consumer-facing enterprises, including early entrants in the internet healthcare sector and more recent internet traffic platforms.
Unlike consumer-facing enterprises that rely heavily on online channels, medical IT companies concentrate their competitive resources offline. For medical IT firms serving business-to-business (B2B) clients, the primary entry point into internet hospital services is through “hospital informatization + regional informatization.” Currently, B2B clients in the healthcare informatization industry can be categorized into two groups: hospital informatization providers, which serve hospitals by offering products such as Hospital Information Systems (HIS), Healthcare Cost Management Systems (HCMS), Management Information Systems (MIS), Electronic Medical Records (EMR), Laboratory Information Systems (LIS), and Picture Archiving and Communication Systems (PACS); and regional health informatization providers, which primarily serve government clients by delivering solutions such as tiered diagnosis and treatment systems, medical insurance information systems, Regional Health Information Systems (RHIS), and Public Health Information Systems (PHIS). B2B clients typically settle payments on a project or order basis, with a certain degree of customization involved, specifically including HIS/Clinical Information System (CIS) construction for hospitals and the development of regional health information platforms.
Number of Hospitals by Grade in 2018

Data source: China Health and Family Planning Statistical Yearbook 2019
We anticipate that all secondary-level and above hospitals will have a demand for launching internet hospital services, meaning there are nearly 10,000 potential unmet projects for physical hospitals to establish internet hospitals. VCBeat has learned that Zhejiang Mediinfo I.T. Co., Ltd. established a subsidiary, Juyi Zhilian, in August 2019 specifically to conduct internet hospital business. According to the head of Juyi Zhilian, the company’s first-phase task is to connect the information channels of thousands of hospitals’ informatization user data to larger platforms, laying the foundation for the later development of diversified data application models.
2. Interconnectivity Rating
Interconnectivity serves as the foundation for the formation of big data and the subsequent development of diverse applications. In September 2017, the National Health Commission issued the “Standardized Maturity Assessment Scheme for Regional (Hospital) Health Information Interconnectivity (2017 Edition).” The assessment of hospital information interconnectivity classifies application ratings into seven levels, which are, in ascending order: Level 1, Level 2, Level 3, Level 4-B, Level 4-A, Level 5-B, and Level 5-A. The requirements for each level are cumulative and progressive; specifically, higher levels encompass all requirements of the lower levels.
The minimum threshold for Level 4 in the Hospital Information Interconnectivity Standardization Maturity Assessment is Level 4-B. The specific requirements for Level 4-B include the preliminary establishment of a hospital information platform based on electronic medical records (EMR), the creation of an EMR shared document repository based on the platform, the implementation of registration services compliant with standard requirements and basic interaction services with higher-level platforms by the platform, no fewer than 13 application functions, connectivity with no fewer than 15 business systems, and interconnection with no fewer than three external institutions.
In August 2018, the Bureau of Medical Administration and Hospital Supervision of the National Health Commission issued the “Notice on Further Promoting the Construction of Information Systems in Medical Institutions with Electronic Medical Records at the Core” (hereinafter referred to as the “Notice”). The Notice stipulated that by 2020, tertiary hospitals should achieve interconnectivity of information across all clinical diagnosis and treatment processes within the hospital, reaching Level 4 in the Standardized Maturity Assessment for Hospital Information Interconnectivity. According to statistics, as of the publication of the sixth batch of assessment results, a total of 214 tertiary hospitals nationwide had achieved Level 4 in the Standardized Maturity Assessment for Hospital Information Interconnectivity, representing a completion rate of less than 10%.
Completion Status of the 2019 Interconnectivity Rating Task

Source: Compiled by VCBeat from public information
Kan Jiaping, Senior Vice President of ZHEJIANG MEDIINFO I.T.CO.,LTD, told VCBeat that the Interconnectivity Maturity Assessment imposes extremely high requirements on the ability to integrate heterogeneous platforms. This necessitates substantial practical experience from healthcare IT enterprises, thereby creating an invisible barrier to entry. “The initial clients for our Interconnectivity Maturity Assessment services are typically long-standing partners with whom we have collaborated for many years,” Kan explained. “For instance, Hangzhou First People’s Hospital, which was among the first batch in China to achieve Level 4 Grade B maturity, was one of the earliest hospitals to adopt our HIS products.” In the aftermath of the pandemic, the importance of the Interconnectivity Maturity Assessment has grown. Furthermore, as the previously emphasized electronic medical record (EMR) initiatives enter their evaluation phase, the Interconnectivity Maturity Assessment is poised to once again become a key focus of hospital IT spending.
3. Cloud Migration of the Infrastructure Layer
For a long time, computational capacity has, to some extent, constrained the ability of healthcare big data to deliver more practical functionalities. Migrating underlying IT systems to the cloud offers advantages in terms of synergy and scalability. Since the 1960s, healthcare IT, as a vital component of the computer industry, has undergone four developmental stages: from mainframes to personal computers and minicomputers, then to internet data centers, and finally into the era of cloud computing. The evolution from computational power being monopolized by a few institutions to enterprises accessing computing resources on demand—transforming computing into a public utility akin to water and electricity—has driven exponential gains in productivity with each technological iteration. Therefore, migrating underlying infrastructure to the cloud is undoubtedly an inevitable trend for healthcare IT.
Future healthcare places high demands on communication and collaboration across hospitals, departments, and teams. Cloud-based underlying systems facilitate more convenient interconnectivity, promoting intra-hospital collaboration and real-time reporting of epidemic data between hospitals and administrative authorities. Furthermore, cloud architecture offers greater flexibility and scalability. During epidemic prevention and control periods, the surge in patient volume and workload within a short timeframe increases the demands on IT system capacity and generates needs for new functional modules. Under a cloud architecture, new workstations and processes can be configured more flexibly and rapidly, facilitating the swift formation of new teams and business lines, as well as the rapid establishment of cross-hospital medical consortia.
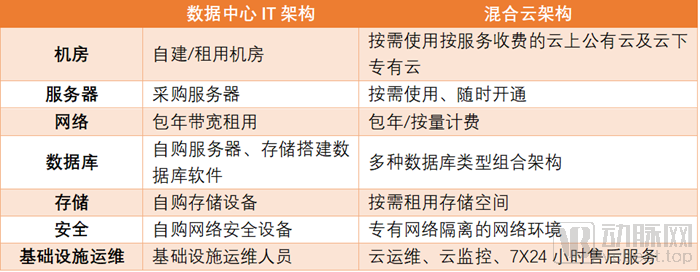
Comparison of Data Center IT Architecture and Hybrid Cloud ArchitectureSource: VCBeat, compiled from public information
In fact, migrating the underlying infrastructure of medical IT systems to the cloud has remained a consistently hot topic. For instance, Wonders Information, in joint construction with the Shanghai Municipal Health Commission, launched China’s first “Health Cloud.” During the pandemic, this platform rapidly deployed a multi-dimensional public service system for novel coronavirus pneumonia, encompassing resident-facing, staff-facing, physician-facing, and management-facing interfaces. It provided various online services, including a health dynamic monitoring system for individuals entering Shanghai, a real-time epidemic map, online consultations, psychological counseling, health knowledge quizzes, and appointment registration. Covering all 16 districts and 243 communities in Shanghai, this cloud platform has become a critical pillar supporting the development of “Internet + Healthcare.” It is reported that Wonders Information also provides platform-based, personalized health management cloud solutions to multiple provinces and cities, including Hunan, Taizhou (Zhejiang), Changping District (Beijing), Mianyang (Sichuan), Jiashan (Zhejiang), Tianjin, and Ningxia. For many other medical IT professionals, migrating underlying infrastructure to the cloud remains a highly attractive business opportunity.
4. Digital Tiered Diagnosis and Treatment
From pilot programs to nationwide rollout, urban medical consortiums and county-level medical communities have become key vehicles for the tiered diagnosis and treatment system. In May 2019, the National Health Commission issued the “Notice on Launching Pilot Programs for the Construction of Urban Medical Consortiums” (Guo Wei Yi Han [2019] No. 125) and formulated the “Work Plan for Pilot Programs on the Construction of Urban Medical Consortiums.” As required by the Plan, medical communities implement unified management of pharmaceuticals and consumables, featuring a unified formulary, centralized procurement and distribution, and consolidated payment for goods. They also establish mutual recognition of medical imaging examination results. Counties are encouraged to establish open and shared centers for medical imaging, electrocardiography, pathological diagnosis, and clinical laboratory testing, thereby promoting grassroots-level examinations, upper-level diagnoses, and regional mutual recognition. Diagnostic and treatment resources are shared within medical communities. Furthermore, coordinated use of beds, appointment slots, and equipment is strengthened both within and between medical communities to further integrate the service chain and achieve resource sharing.
In essence, the mutual recognition of medical information and resource sharing within Medical Consortiums are underpinned by the interconnectivity and efficient transmission of information and data, thereby driving incremental demand. In September 2019, the National Health Commission and the National Administration of Traditional Chinese Medicine jointly issued the List of Pilot Provinces and Counties for the Construction of Close-knit County-level Medical and Health Consortia, designating Shanxi Province and Zhejiang Province as pilot provinces, and 567 counties (cities and districts), including Xicheng District in Beijing, as pilot counties for the construction of close-knit county-level medical consortia.

“List of Pilot Provinces and Counties for the Construction of Close-Knit County-Level Medical and Health Consortia”Data Source: Public Documents
According to industry insiders, the digital medical community project is a long-term investment and construction endeavor. The first phase of construction typically takes around 12 months, with order values ranging from hundreds of thousands to several million yuan, depending on the scope of planning. Currently, the development of digital medical communities in China is still in its early stages. Only a few county-level medical community digitalization projects, which were planned earlier, have begun to be implemented. For instance, the first phase of the Jiashan County Digital Medical Community project in Zhejiang Province, undertaken by ZHEJIANG MEDIINFO I.T.CO.,LTD, was officially launched in January 2020.
5. Cross-Regional Settlement of Medical Insurance
Currently, cross-regional settlement of medical insurance has become the norm due to widespread access to healthcare services. In the future, the development of a digitalized system for cross-regional medical insurance settlement will become a prevailing trend.
As of the end of December 2019, the number of medical institutions providing direct settlement for cross-provincial non-local medical care reached 27,608, including 24,720 designated medical institutions at Level II and below, representing an increase of 12,197 and 11,917 institutions, respectively, compared with 2018. The cumulative number of settled visits amounted to 4.246 million, doubling the figure from 2018.
In fact, with the establishment of the National Healthcare Security Administration and its provincial and municipal counterparts, along with the advancement of healthcare security reforms, both the connotation and extension of medical insurance have undergone significant changes. The nationwide unified medical insurance IT system serves as the foundation for cross-regional settlement of medical insurance claims. In the first half of 2019, the National Healthcare Security Administration launched tenders for 14 information system projects grouped into nine packages, marking the commencement of the new medical insurance information system construction.
In July of the same year, clear national standards for the construction of a unified healthcare insurance IT system were officially released. Following the end of the pandemic, the development of a unified healthcare insurance IT infrastructure, along with subsequent systems for cross-regional settlement, cost containment, and regulatory oversight, is expected to accelerate. Furthermore, once the central healthcare insurance authority’s systems are fully established, they will need to connect with designated medical institutions, clinics, and pharmacies to provide services. Healthcare IT companies can also offer refined management solutions and cloud-based MIS (Management Information Systems) for pharmacies, as well as regulatory compliance and rapid claims processing services for commercial insurance providers, thereby creating new growth opportunities.
Public Health Information Platform
By the time the “13th Five-Year” National Plan for Population Health Informatization Development (hereinafter referred to as the “13th Five-Year Plan”) was released in 2017, databases for population information, electronic health records, and electronic medical records had been preliminarily established. Twenty-seven provinces (autonomous regions and municipalities) across China had set up provincial-level population health information platforms, which, along with 44 hospitals directly under the administration of the National Health Commission, were connected to the national platform.
In April 2008, the National Automated Early Warning System for Infectious Diseases was launched across all 31 provinces (including municipalities directly under the Central Government and autonomous regions) in China, thereby establishing an automated early warning and response mechanism. Underpinning this system is the well-known National Notifiable Disease Reporting System (NNDRS), which serves as the core subsystem of the National Information Management System for Infectious Disease Reporting. In medical institutions covered by the NNDRS, physicians can complete infectious disease report cards and submit real-time, online, and direct reports of cases involving 39 notifiable infectious diseases identified during their practice. According to the 13th Five-Year Plan, the coverage rate of the NNDRS among medical institutions was targeted to reach 95% by 2020.
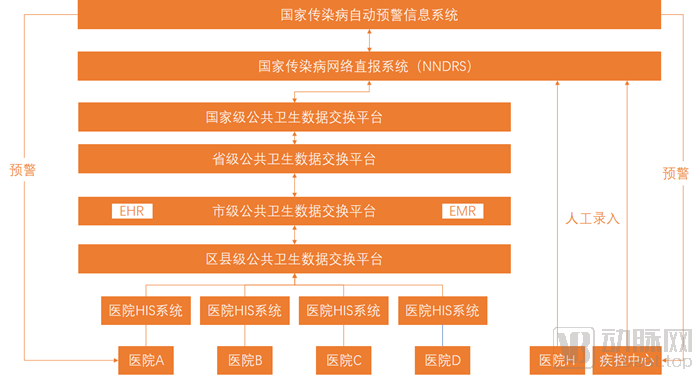
Epidemic Information Transmission Network | Data Source: VCBeat, compiled from public information
During the epidemic, case data directly reported by medical institutions to the NNDRS system were transmitted to the four-tier (national, provincial, municipal, and district/county-level) public health data exchange platform, forming an important source of publicly available epidemic data.
However, since the infectious disease report card represents a judgment based on known ICD-10 diagnostic codes, novel infectious diseases require a prolonged reporting and verification process involving repeated checks and confirmations. This was the reason why the COVID-19 outbreak was not captured in a timely manner by the National Notifiable Disease Reporting System (NNDRS), leading to the failure of the automated early warning information system. It was not until January 24 that the Chinese Center for Disease Control and Prevention urgently launched a new detection function for pneumonia caused by the novel coronavirus within the NNDRS, thereby exposing functional deficiencies in the public health informatics platform.
Accordingly, we believe that public health informatics platforms, centered on Level-4 regional informatization platforms and the three major population health databases, still have rigid demands for medical IT services. This enables public health informatics platforms to possess greater flexibility and scalability during sudden outbreaks. During the pandemic, ZHEJIANG MEDIINFO I.T.CO.,LTD leveraged its prior achievements in regional informatization to build a COVID-19 data monitoring platform for the Health Commission of Jiangxi Province. The company fully utilized existing electronic data in various formats for cleaning, importation, and collection, presenting the data intuitively through the most appropriate and straightforward visualization methods. Additionally, by incorporating external auxiliary decision-making data, the platform made significant contributions to epidemic control across Jiangxi Province.
In late March, medical teams from across China that had been dispatched to Hubei began to withdraw one after another. The sentiment of “we’ll meet again” behind this departure signifies that the nationwide campaign against the COVID-19 pandemic is successfully driving the virus into retreat. While it may still be premature to discuss how a sudden public health emergency will shape the future, it is never too early to make preparations.
In practice, from the perspectives of both business development and practical application, the aforementioned six major directions are not isolated from one another; their interactions will propel the informatization of population health to a higher level. We believe that for healthcare IT enterprises that have seized the first-mover advantage in smart healthcare, how to integrate existing resources to capitalize on emerging opportunities is a critical issue requiring careful consideration.