China's National Healthcare Security Administration Releases Latest Medical Insurance Data: Expenditure Surpasses RMB 3 Trillion in 2025, Signaling Deepened Reform Directions
Recently, the National Healthcare Security Administration released the "Statistical Bulletin on the Development of Medical Security Undertakings in 2019." According to the data disclosed in the bulletin, in 2019, the total number of participants in basic medical insurance across all categories reached 1.35436 billion, with the coverage rate remaining stable at over 95%.The total revenue and total expenditure of the basic medical insurance fund for the year were RMB 2,333.487 billion and RMB 1,994.573 billion, respectively, with a cumulative balance of RMB 2,691.211 billion at the end of the year.
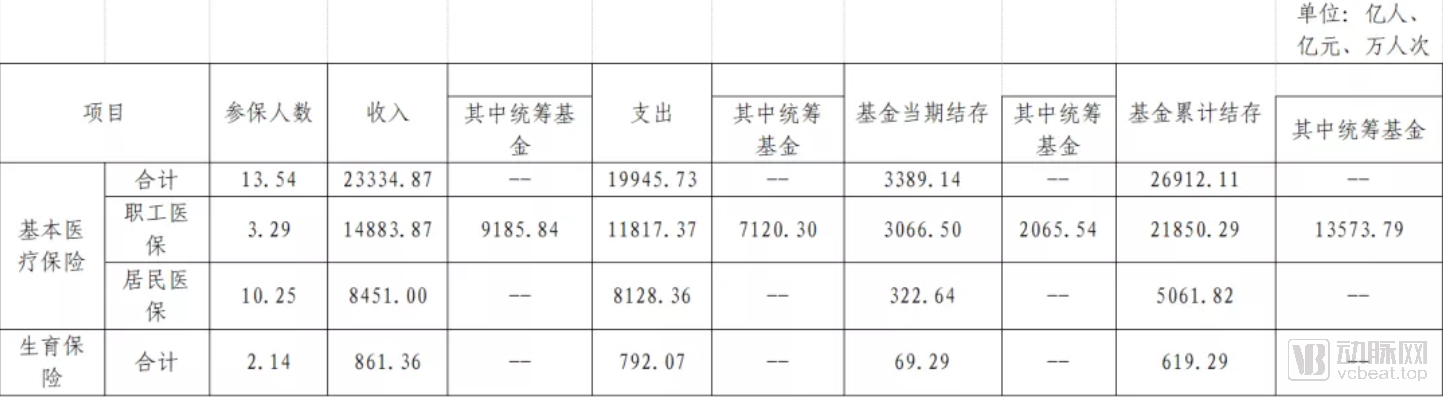
(2019 Key Indicators from the National Healthcare Security Flash Report)
In the 2019 edition of the National Reimbursement Drug List, there were a total of 2,709 Western medicines and Chinese proprietary medicines, including 1,370 Western medicines and 1,339 Chinese proprietary medicines. In addition, 892 types of Chinese herbal decoction pieces with national standards were also included.
InPharmaceutical ProcurementAs of the end of 2019, the preliminary statistics showed that the total value of online procurement orders placed through provincial-level centralized drug procurement platforms across all 31 provinces (autonomous regions and municipalities) in China amounted to RMB 991.3 billion. Of this, orders for Western medicines (chemical drugs and biological products) totaled RMB 811.5 billion, while orders for proprietary Chinese medicines totaled RMB 179.8 billion. The value of orders for drugs covered by the Basic Medical Insurance scheme reached RMB 832.7 billion, accounting for 84% of the total.
By the end of 2019, the 25 selected drugs in the pilot regions for the “4+7” centralized volume-based drug procurement had achieved an average of 183% of their agreed-upon procurement volumes, with the procurement volume of selected drugs accounting for 78% of the total procurement volume for drugs with the same generic names. Following the nationwide expansion of the pilot program, all 25 generic drug varieties were successfully included in the expanded procurement, resulting in an average price reduction of 59%, which represented a further 25% decrease compared to the prices in the “4+7” pilot program.
In terms of health insurance payment methodsIn China, 97.5% of medical insurance pooling areas have implemented global budget controls for healthcare payments, and 86.3% have adopted diagnosis-related group (DRG) payment systems. Thirty cities have been included in the national pilot program for CHS-DRG payment. More than 60% of pooling areas have implemented per-diem payment for long-term and chronic disease inpatient services, while exploring capitation-based payment models integrated with chronic disease management for primary care services.
On the Direct Settlement of Cross-Provincial Medical Expenses for Out-of-Area PatientsAs of the end of 2019, there were 27,608 medical institutions participating in the direct settlement of cross-provincial healthcare expenses. The coverage of primary care institutions continued to expand, with 24,720 designated medical institutions at Level II and below. Throughout the year, direct settlements for cross-provincial healthcare services were conducted for 2.72 million visits, involving total medical costs of RMB 64.82 billion, of which RMB 38.32 billion was paid by the insurance fund. The average cost per hospitalization was RMB 24,000, with an average fund payment of RMB 14,000 per stay. All 41 cities in the Yangtze River Delta region have achieved full coverage of direct settlement for outpatient expenses incurred across provincial boundaries, while five southwestern provinces (Yunnan, Guizhou, Sichuan, Chongqing, and Tibet) have launched direct settlement for cross-provincial outpatient expenses.
On the Supervision of Medical Insurance Funds, a total of 264,000 medical institutions were investigated and penalized for violations of laws, regulations, and contractual agreements throughout the year; local authorities processed 33,100 insured individuals involved in illegal or irregular activities; and a total of RMB 11.556 billion in funds was recovered during the year.
In just 22 months since its establishment, the National Healthcare Security Administration has delivered a truly impressive track record.
As healthcare reform enters uncharted waters, and as the traditional medical system converges with new technologies and concepts, the National Healthcare Security Administration acts as a helmsman who perceives both immediate realities and distant horizons. By carefully balancing the old and the new, it steadily steers the vast ship of China’s healthcare reform toward the shores of a Healthy China through a series of deliberate policy initiatives.
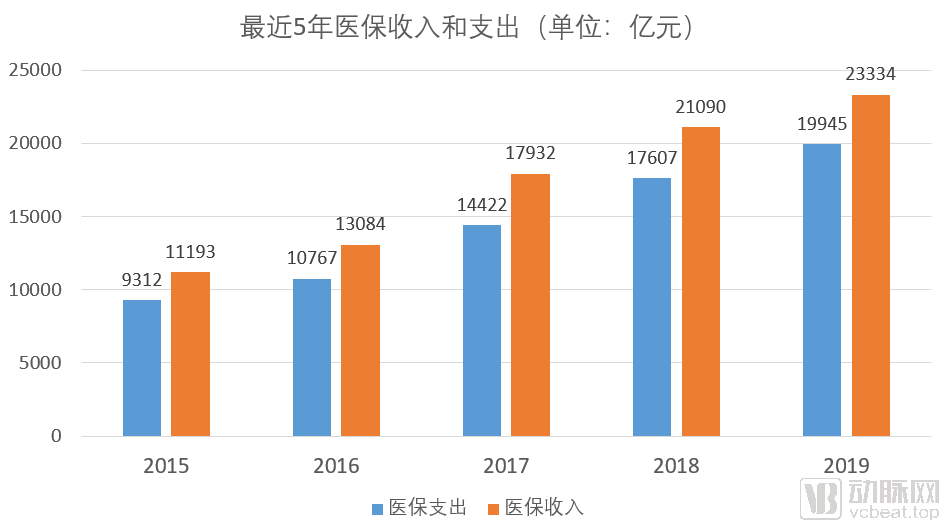
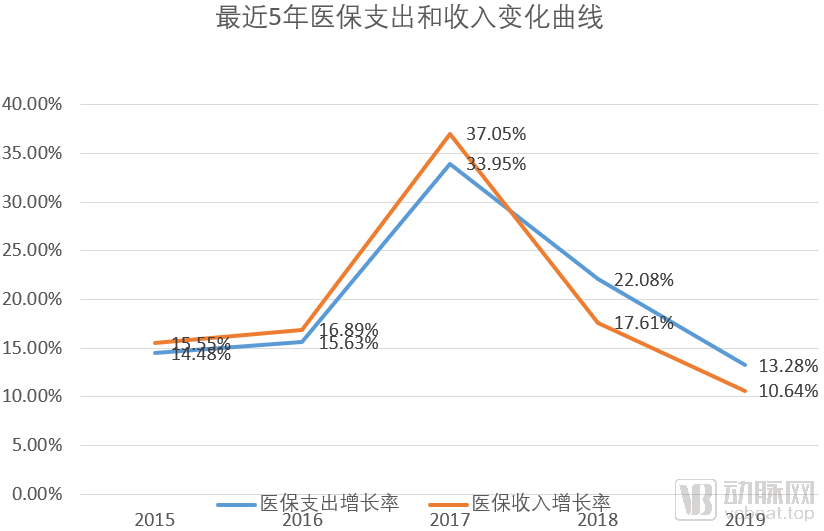
In recent years, with the rise in medical costs, health insurance has faced significant pressure. As can be seen from the figure,Although the growth in absolute terms of medical insurance expenditures is lower than that of medical insurance surpluses, the former’s growth rate exceeds the latter’s. If this trend continues, the medical insurance fund will face the risk of deficits, thereby breaking the “Expenditure Determined by Revenue, Ensuring Surplus, and Maintaining Risk Resilience to Avoid Deficits” and other principles.
Healthcare insurance is vital to the national economy and people's livelihood, so its importance goes without saying. Thus, against the backdrop of the major institutional reform of the State Council, the National Healthcare Security Administration was established.On May 31, 2018, the National Healthcare Security Administration was officially established amid widespread attention. The management functions previously dispersed across four departments were consolidated under the National Healthcare Security Administration, marking a significant shift in the healthcare industry.“Super Buyer”Was born.
The National Healthcare Security Administration (NHSA) is positioned as the primary purchaser of medical services, thereby enabling it to play a decisive role in shaping the development of the healthcare service system and allocating health resources. In terms of organizational structure, the NHSA comprises six departments and one office under its leadership, which consists of one director and three deputy directors. Hu Jinglin, former Vice Minister of Finance, was appointed as the inaugural Director of the NHSA.
Shortly after its establishment, the National Healthcare Security Administration addressed issues of significant public concern by issuing its first major policy: the “Notice on Launching Provincial-Level Special Centralized Procurement of Anti-Cancer Drugs.”
With this as the opening, the National Healthcare Security Administration (NHSA) launched a series of reforms with far-reaching implications for the industry, focusing on key areas such as healthcare security fund management, adjustments to the national reimbursement drug list, and drug pricing. By systematically reviewing and analyzing all policies disclosed on the NHSA’s official website, VCBeat has identified five major sectors with significant policy impact from an industry perspective, namely:Internet healthcare, adjustment of the National Reimbursement Drug List (NRDL), centralized drug procurement, informatization of medical insurance, and Diagnosis-Related Groups (DRGs).
1. Internet Healthcare
Historically, the industry widely believed that the lack of integration with medical insurance payment systems would pose a significant barrier to the development of the internet healthcare sector.
On August 30, 2019, the National Healthcare Security Administration issued the “Guiding Opinions on Improving Price Formation and Medical Insurance Reimbursement Policies for ‘Internet+’ Medical Services,” breaking the ice and removing barriers to industry development.
The current guidance on medical insurance policies proposes that online and offline medical services should be subject to equitable pricing and reimbursement policies. For "Internet+" medical services provided by designated medical institutions, if the service content is identical to that of offline medical services covered by medical insurance and the fees charged align with those of corresponding public medical institutions, such services shall be included in the scope of medical insurance coverage and reimbursed accordingly upon completion of the requisite filing procedures.
During the COVID-19 pandemic, the National Healthcare Security Administration (NHSA), in conjunction with the National Health Commission (NHC), issued the "Guiding Opinions on Promoting 'Internet+' Healthcare Services During the Prevention and Control of COVID-19" on March 2, 2020. The document explicitly states that online follow-up services for common and chronic diseases provided by qualified internet-based medical institutions to insured individuals may be included in the scope of reimbursement from the basic medical insurance fund in accordance with local regulations. Internet-based medical institutions may issue electronic prescriptions online for insured individuals, who can then obtain medications through various flexible offline channels while enjoying medical insurance coverage. The healthcare security authorities have strengthened collaboration with internet-based medical institutions and other relevant parties to enable direct online settlement of the portions of consultation and medication fees covered by medical insurance. As a result, insured individuals are only required to pay the out-of-pocket portion, similar to using their insurance cards for medication purchases at physical hospitals.
It is evident that policies are increasingly favoring the internet healthcare industry.
2. Adjustment of the National Reimbursement Drug List
The National Reimbursement Drug List (NRDL) controls 80% of the sales market in public hospitals. For pharmaceutical companies, failure to be included in the NRDL means losing the volume growth advantage driven by reimbursement coverage, thereby plunging them into fierce market competition. For consumers, the inclusion of more life-saving and emergency medications in the NRDL would help reduce out-of-pocket expenses.
On August 20, 2019, a notice issued by the National Healthcare Security Administration on printing and distributing the “National Basic Medical Insurance, Work-Related Injury Insurance, and Maternity Insurance Drug Catalog” triggered an earthquake in the industry. This catalog adjustment added 148 drug varieties to the routine access list and removed 150 varieties.
This major revision of the drug catalog marks the first comprehensive adjustment since the establishment of the National Healthcare Security Administration (NHSA) and represents a thorough review of the existing catalog entries since the inaugural version was released in 2000. It comes just two years after the previous major update to the national reimbursement drug list.
In light of this, the dynamic adjustment of the National Reimbursement Drug List (NRDL) is returning to a normalized routine. With the shortened adjustment cycle, the NRDL can facilitate more timely inclusion and exclusion of drugs, thereby revitalizing existing medical insurance resources, improving drug accessibility, and maximizing the efficacy of medical insurance funds.
The new National Reimbursement Drug List (NRDL) has been in effect since January 1, 2020.
3. Centralized Drug Procurement
The purpose of centralized drug procurement is to explore and improve the mechanism for centralized drug procurement and a market-driven price formation mechanism, reduce the public’s burden of medication costs, standardize drug distribution order, and enhance medication safety for the public.
Since the establishment of the National Healthcare Security Administration (NHSA), which consolidates the powers of payment, supervision, and pricing, its inaugural policy focused on centralized drug procurement. The subsequent rollout of multiple related policies underscores the NHSA’s strong commitment to controlling pharmaceutical costs.
In November 2018, the National Healthcare Security Administration, in conjunction with the National Health Commission, the National Medical Products Administration, and other relevant departments, studied and drafted a pilot program. Adhering to the principle of “state organization, alliance-based procurement, and platform-based operation,” the “4+7” pilot program was launched.
According to the latest data this year, following the nationwide expansion of the pilot program, procurement was successfully expanded for all 25 generic drug varieties. The expanded procurement prices decreased by an average of 59%, representing a further 25% reduction compared to the "4+7" pilot program.
Reducing drug prices is the first step toward truly separating prescribing from dispensing. The achievements of centralized drug procurement seem to herald the official onset of a new era in healthcare reform led by medical insurance.
4. Informatization of Medical Insurance
China’s medical insurance information system has long been plagued by three major issues: First, inconsistent standards and non-reciprocal data recognition have prevented the formation of big data at both national and regional levels, let alone enabling effective big data analytics. Second, fragmented systems hinder data sharing; nearly 400 pooling areas across China have developed their own information systems independently, which are scattered across different departments such as Human Resources and Social Security, Civil Affairs, and Health Commission, resulting in poor interoperability. Third, regional closure and prominent “data silo” phenomena persist, as each pooling area manages its medical insurance data in a closed manner. Each pooling area operates as an “information silo,” where external access is blocked and internal data cannot be shared outward, leading to isolated and self-contained operations.
Establishing a nationally unified healthcare security information system has become a top priority for the National Healthcare Security Administration.
At the 2018 National Healthcare Security Work Conference, the “One, Two, Three, Four” objectives for healthcare security informatization were proposed, and subsequent work began to advance steadily. In 2019, the “Dynamic Maintenance of Healthcare Security Business Coding Standards” was launched on a trial basis on the official website of the National Healthcare Security Administration, marking the formal implementation of the National Healthcare Security Information Platform. Among the 15 information business coding standards, four healthcare security information business codes—“Disease Diagnosis and Surgical Procedures,” “Pharmaceuticals,” “Medical Service Items,” and “Medical Consumables”—were also put into operation.
In accordance with the Guiding Opinions on Standardization Work in Medical Security, by 2020, on the basis of constructing a nationally unified medical security information system, the implementation and application of 15 information business coding standards, including those for disease diagnosis and surgical procedures, were gradually achieved. During the 14th Five-Year Plan period, a national list of medical security standards was established, and the research, formulation, pilot testing, and improvement of selected medical security standards were initiated.
According to VCBeat’s recent analysis of winning bid data for healthcare informatization projects, the market size for healthcare informatization in China was approximately RMB 58.2 billion in 2019 and is poised for substantial growth in the future.
5.DRGs
DRG-based payment is an advanced health insurance reimbursement method currently adopted by countries such as the United States, Germany, and France. It involves a comprehensive analysis of patients’ clinical conditions to assign them to specific diagnostic groups for bundled treatment, thereby standardizing care pathways and ensuring cost controllability.
From a historical perspective, starting in 2017, the National Health Commission launched pilot reforms for DRG-based payment and charging in Sanming City (Fujian Province), Shenzhen City (Guangdong Province), Karamay City (Xinjiang Uygur Autonomous Region), and three medical institutions in Fujian Province. In January 2018, Sanming City, Fujian Province, went live with its DRG payment and charging system.
Subsequently, in line with the three-step approach of “top-level design, simulation testing, and actual payment,” the National Healthcare Security Administration issued key policy documents, including the Notice on Applying for the National Pilot Program for Diagnosis-Related Group (DRG)-Based Payment and the Notice on Issuing the List of Cities Selected for the National Pilot Program for DRG-Based Payment, thereby launching DRG-based payment pilots in 30 cities across China.
In 2020, DRG-based payment was simulated in 30 pilot cities across China, with actual implementation scheduled to commence in 2021.
On March 5, 2020, the “Opinions on Deepening the Reform of the Medical Security System” (hereinafter referred to as the “Opinions”), issued by the Central Committee of the Communist Party of China and the State Council, sparked significant repercussions across the industry upon its release. It was hailed by many industry insiders as a programmatic document that would set the tone for China’s healthcare reform over the next decade.
Although the “Opinions” initiate reforms by deepening medical insurance reform, they extensively cover many aspects of the healthcare industry ecosystem and are bound to exert a profound impact on the sector. The “Opinions” propose an overall reform framework of “1+4+2”:
The “1” refers to the goal of striving to fully establish by 2030 a multi-tiered medical security system, with basic medical insurance as the mainstay, medical assistance as the safety net, and supplementary medical insurance, commercial health insurance, charitable donations, and mutual medical aid developing in concert. The “4” denotes the improvement of four mechanisms: benefit coverage, funding and operation, medical insurance payment, and fund supervision. The “2” signifies the enhancement of two supports: pharmaceutical and medical service supply, and medical security services.
From the overarching objectives of this programmatic document, it is evident that the National Healthcare Security Administration’s (NHSA) role as a “super purchaser” will gradually recede. While fulfilling its historical mission as a “super purchaser,” the NHSA is, in fact, spearheading the establishment of a multi-tiered healthcare security system. Judging by current industry development trends, China’s healthcare payers are shifting toward market-oriented commercial insurance and innovative payment entities such as online mutual aid platforms.
2019,The market size of health insurance is RMB 706.6 billion., based on the projected growth rate of over 30% compound annual growth rate (CAGR) in the market over the past five years, the market size of health insurance is expected to approach or even exceed one trillion this year. It can be seen that commercial insurance will play a leading role in the future multi-tiered medical security system, similar to that of public health insurance.
Moreover,The development of commercial health insurance presents an even greater opportunity for the healthcare industry: as new medical payment methods are established and widely adopted within the sector, a novel model of medical services tailored to these payment mechanisms will also be established and popularized.
This is atMarshall McLuhan, Neil Postman, Kevin Kelly, Clayton Christensenan insight mentioned in the works of philosophers.