Global Sharing by Academicians Zhong Nanshan and Li Lanjuan: A 20,000-Word Transcript on COVID-19 Prevention, Treatment, Clinical Management, and Therapeutic Experience
On the evening of April 2 (Beijing Time), the International Experience-Sharing Conference on COVID-19 Prevention and Control and the Launch Ceremony of the Healthy China International Public Health Management Training Program were held online. The event was jointly organized by multiple parties, including the Chinese Patient Assistance Alliance, the National Health Commission’s Telemedicine Management and Training Center, the Beijing Kangmeng Charity Foundation, the Beijing Life Oasis Public Service Center, and the China Primary Health Care Foundation.
This sharing session is open to a global audience, aiming to actively respond to the call from the World Health Organization (WHO) and the international community, promote the exchange of international experience, and facilitate discussions among experts from various countries on unresolved issues. Meanwhile, the “Healthy China International Public Health Management Training” program will be officially launched at the conference, introducing the training initiative to healthcare professionals and encouraging their active participation.
In the highly anticipated session on sharing experiences in COVID-19 prevention and control, Academician Zhong Nanshan, an academician of the Chinese Academy of Engineering and a professor at Guangzhou Medical University, shared insights into the research, diagnosis, and treatment of COVID-19. Another well-known hero in the fight against the epidemic, Academician Li Lanjuan, also an academician of the Chinese Academy of Engineering and a professor at Zhejiang University, shared her experience regarding cytokine storms and the treatment of severe COVID-19 cases. Meanwhile, multiple medical experts, including the two academicians, exchanged views on COVID-19 prevention and control strategies through a roundtable forum.
VCBeat has compiled the conference content, with a full transcript provided below.
As the conference commenced, Academician Chen Zhu, former Minister of Health and current Chairman of the Central Committee of the Chinese Peasants and Workers Democratic Party, sent a congratulatory letter. In his message, he extended sincere gratitude to all parties involved in organizing the training program and expressed high regard for the medical professionals from various countries participating in the training and exchanges. To date, the Chinese government, along with institutions such as the Red Cross Society of China—which serves as the government’s assistant in humanitarian affairs—has provided anti-pandemic assistance to 89 countries and four international organizations to the best of its ability.
Dr. Gauden Galea, the World Health Organization’s Representative in China, shared an external perspective on the various efforts made by China during this public health emergency. He noted that while the “China model” may sound monolithic, it actually encompasses a wide range of detailed prevention and control measures, employing a combination of diverse tools and approaches. Dr. Galea believes that other countries and regions can learn from this Chinese model and conduct more in-depth analysis, sharing, and understanding of it.
Professor Lu Qingjun, Director of the National Health Commission’s Telemedicine Management and Training Center and co-organizer of this event, expressed his hope that, through the Healthy China International Public Health Management Course, experience in epidemic prevention and control would be distilled into a theoretical framework, integrating infectious disease prevention and treatment with public health management. This approach aims to enhance healthcare professionals’ understanding of public health, strengthen the integration of clinical medicine and public health, emphasize both theoretical learning and practical application, and help elevate China’s disease prevention and public health management to a new level.
Here we have an expert committee formed during the outbreak of COVID-19, including Professor Li Lanjuan, Professor Gao Fu, and myself, among other experts. At that time, we announced to the media that there was human-to-human transmission of COVID-19.
At that time, the government faced two choices in dealing with highly infectious diseases: should we suppress it or mitigate it? If we chose to suppress it, it would certainly have a significant impact on the economy. However, due to its high transmissibility and a very large basic reproduction number (R0), we had another option: mitigation. The question then becomes: Would measures taken to delay and reduce its high transmissibility be effective?
Faced with two options, the Chinese government chose suppression, taking proactive measures to intervene.
So, what stringent containment measures did we implement? The first was the lockdown of Wuhan. At that time, it was decided that people should neither travel to Wuhan nor leave the city, which became a key principle at the time.
Second, ensure information transparency. We provide real-time updates on the number of confirmed and suspected cases, with data publicly disclosed daily for every city across China.
Third, activate the joint prevention and control mechanism. In brief, this entails early prevention, early detection, early diagnosis, and early isolation. Early diagnosis should be conducted in hospitals rather than at the Centers for Disease Control and Prevention (CDC). Additionally, real-time quantitative PCR testing should be performed, with nucleic acid testing mandated for all close contacts, including asymptomatic individuals.
On January 23, Wuhan went into lockdown, after which we began implementing a series of measures. It took two weeks from January 23 to reach the peak, and another two weeks to decline back to the original level. Overall, it took four weeks to bring the spread of the epidemic under control.
This is the curve of new cases in China, representing statistically confirmed cases. Four weeks have passed, and case numbers outside China are still on the rise. As can be seen, our data declined over a two-week period, suggesting that these stringent containment measures are effective.
We also engaged in a debate at the time: Is wearing masks effective? Can it prevent infection? Wearing a mask only prevents patients from transmitting the virus to others, which is why people in some countries feel that mask-wearers are subject to discrimination. This is because wearing a mask seems to imply that one is a patient, but this is not actually the case. More importantly, wearing a mask is intended to protect oneself from infection when coming into contact with patients.
Some opponents argue that wearing masks is ineffective and cannot prevent viruses from penetrating the mask, with the exception of medical-grade N95 respirators used in surgical settings. The majority of Chinese people, however, support mask-wearing, believing it should be mandated. This practice can effectively prevent droplet transmission. Since droplet spread has been identified as the primary route of viral transmission, wearing masks can interrupt this key pathway, which is crucial for virus prevention and control.
Just now, Dr. Gao Li began by discussing the overall policy, which essentially has two core components: first, maintaining social distance, and second, wearing masks.
Here is a case involving a man who flew from Shanghai to Germany for a business trip and conference, then returned to China, after which he began to exhibit symptoms. Two to three days later, he was diagnosed with COVID-19. Meanwhile, two other individuals traveling with him were also infected; they were initially asymptomatic but were subsequently confirmed to be infected following their joint travel.
This serves as evidence of human-to-human transmission; furthermore, it demonstrates that asymptomatic individuals can also transmit the virus. This underscores the need to pay closer attention to asymptomatic carriers, as they may potentially spread the virus to healthy populations.
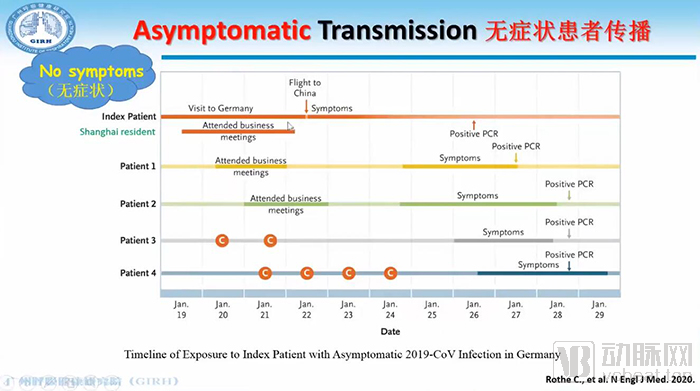
Image sourced from a screenshot of the conference’s live video stream
I am uncertain about its transmissibility, but I can offer some clues. Two groups require close attention: those who have had close contact with infected individuals, and those from key epidemic areas.
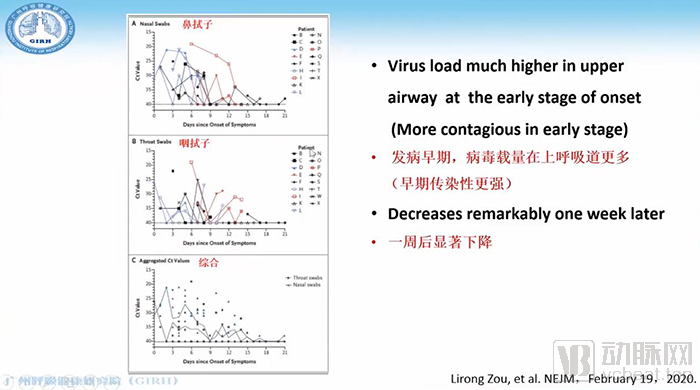
Image sourced from a screenshot of the conference’s live video stream.
Statistical data from nasal and pharyngeal swabs indicate that viral load is extremely high in the early stages of disease onset. The earlier the stage, the higher the viral load in the upper respiratory tract; after one week, the viral load in the respiratory tract declines significantly. Therefore, we believe that asymptomatic individuals still maintain a high viral load in the upper respiratory tract, indicating strong infectivity.
We have tried several treatment methods and conducted several controlled studies. The first was lopinavir/ritonavir, also known as Kaletra; the second was chloroquine; the third was tocilizumab, an IL-6 receptor antibody; the fourth was Lianhua Qingwen capsules, a traditional Chinese medicine; the fifth was inhalation of hydrogen-oxygen mixed gas to further improve blood oxygen levels. The last was remdesivir.
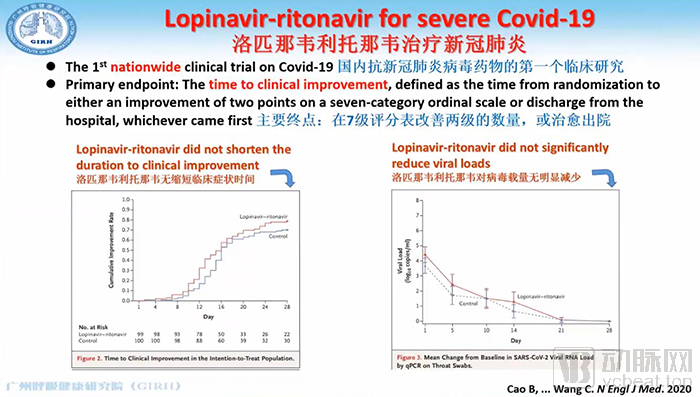
Image sourced from a screenshot of the conference's live video stream.
Here, I will present a clinical study conducted by Professor Cao Bin to evaluate the efficacy of Kaletra in treating COVID-19. As can be seen, Kaletra did not demonstrate significant benefits in terms of improvement on a 7-point ordinal scale; its effects on reducing viral load or shortening the duration of clinical symptoms were modest. Our conclusion is that Kaletra is not the most effective treatment option.
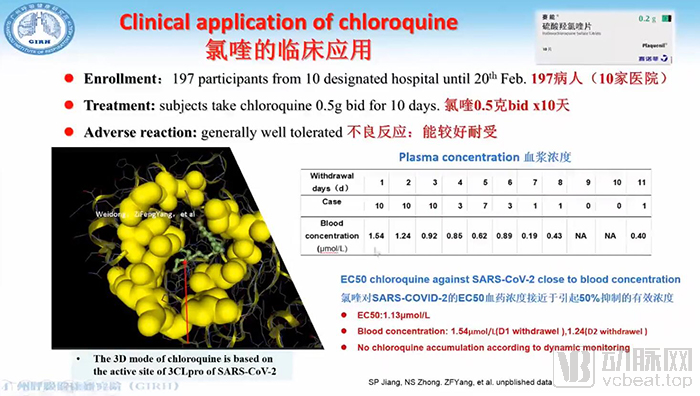
Image sourced from a screenshot of the conference's live video stream.
Second, we examine the clinical trials of chloroquine. Based on in vitro studies, we hypothesized that chloroquine might exert its therapeutic effect by targeting the 3CL protease of SARS-CoV-2. A total of 197 patients from 10 hospitals participated in the clinical trial. After administering chloroquine at a dose of 500 mg twice daily for 10 days, the blood concentration reached 1.54 μmol/L, which is very close to the EC50 value (1.13 μmol/L) observed in in vitro experiments. Therefore, we believe it should be effective.
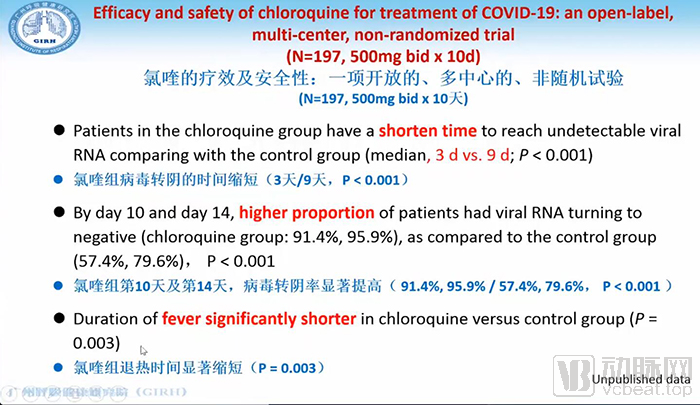
Image sourced from a screenshot of the conference’s live video stream.
In the treatment group, which received chloroquine, the time to viral clearance was 3 days, significantly shorter than the 9 days observed in the control group. The rates of viral clearance on day 10 and day 14 were also higher in the treatment group, at 91.4% and 95.9%, respectively, compared to 57.4% and 79.6% in the control group. The time to fever resolution was also significantly shorter in the chloroquine group than in the control group. Chloroquine demonstrated a much faster rate of viral clearance. Clinical trials indicate that chloroquine has a relatively significant therapeutic effect.
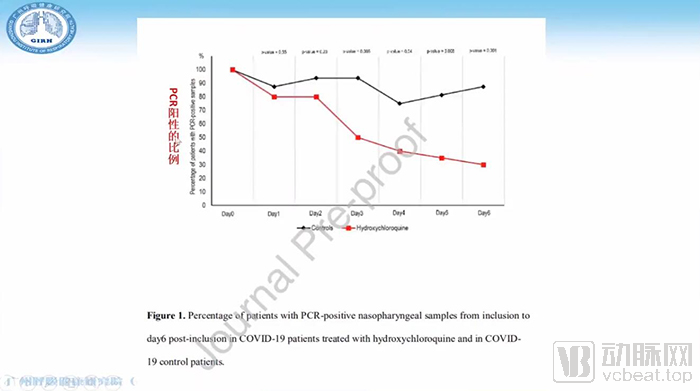
Image sourced from a screenshot of the conference’s live video stream.
Another clinical trial evaluated the combination of hydroxychloroquine and azithromycin for the treatment of COVID-19. The study included only 20 cases, representing a relatively small sample size. Patients received 600 mg of hydroxychloroquine daily, underwent daily nasopharyngeal swab testing for viral detection at the hospital, and were administered azithromycin as appropriate based on their clinical condition. The results demonstrated a significant effect, with notable changes in viral load compared to the control group.
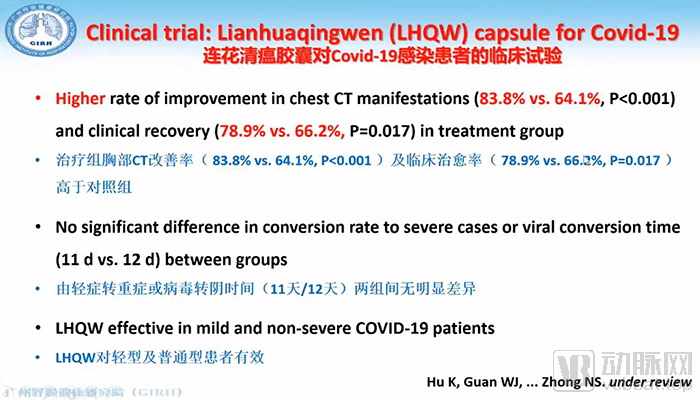
Image sourced from a screenshot of the conference's live video stream.
Another option is the traditional Chinese medicine Lianhua Qingwen capsules. Here, I will share some data with you: a total of 284 patients were enrolled, with the control group and treatment group allocated in a 1:1 ratio. The overall treatment efficacy rate was higher in the treatment group (91.5%) than in the control group (82.4%). Meanwhile, symptom improvement occurred more rapidly in the treatment group, taking 7 days compared to 10 days in the control group, demonstrating a notable difference in outcomes. The improvement rate on chest CT scans was 78.9% in the treatment group, significantly better than the 66.2% observed in the control group. However, there was no significant difference between the two groups in terms of progression from mild to severe cases or the time required for viral clearance. Therefore, Lianhua Qingwen capsules are more effective for patients with mild and moderate conditions.
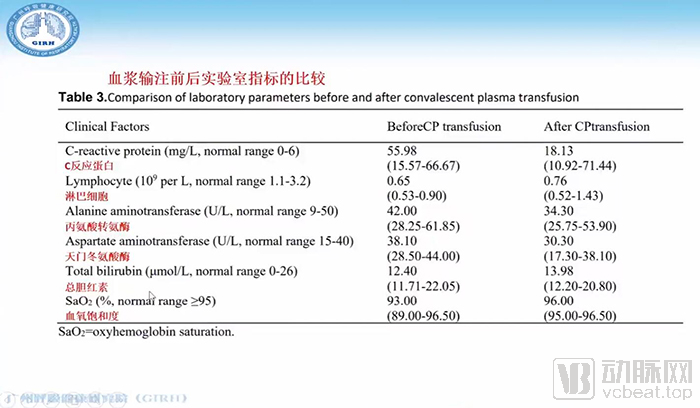
Image sourced from a screenshot of the conference’s live video stream.
Next, we examine the results of the clinical study involving the transfusion of 200 mL of convalescent plasma with a neutralizing antibody titer of 1:640, including the safety profile of the plasma transfusion. We subsequently compared laboratory parameters. Although no significant differences were observed in these laboratory data, a comparison of pre- and post-treatment values in patients receiving convalescent plasma therapy revealed a substantial increase in serum neutralizing antibody levels. Meanwhile, viral loads decreased significantly, with all patients testing negative. These findings clearly demonstrate the pronounced efficacy of convalescent plasma therapy.
There is also data from a few days ago: an open-label clinical study involving five critically ill patients. Donors provided convalescent plasma, in which the binding titer of specific IgG antibodies reached 1:1000 and the neutralizing titer exceeded 40. The plasma was administered via intravenous infusion at a dose of 40 mL per session. The results showed that the cycle threshold (Ct) values increased in all patients, indicating a decrease in viral load. Additionally, SOFA scores decreased, the oxygenation index improved, and body temperature declined. In other words, convalescent plasma therapy does demonstrate a certain level of efficacy.
Lastly, inhalation of hydrogen-oxygen gas mixtures can alleviate dyspnea. Patients with dyspnea who receive nebulization therapy with inhaled hydrogen-oxygen gas mixtures can experience reduced airway obstruction.
The case fatality rate among patients with severe COVID-19, particularly those in critical condition, is a matter of great significance. Globally, more than 45,000 deaths have been reported, which constitutes a grave challenge. To address this issue, as Academician Zhong has just mentioned, we traveled to Wuhan together on January 18, and I subsequently led a team back to Wuhan on February 1 to treat critically ill patients. The team returned only on the 31st and is currently still under quarantine.
Through two months of clinical observation, we have identified a critical time window during which COVID-19 patients progress to severe disease. Typically, after one week, patients experience a sudden deterioration in their condition, characterized by dyspnea, tachypnea (respiratory rate >30 breaths per minute), decreased oxygen saturation, and a reduced PaO2/FiO2 ratio. In severe cases, the condition can rapidly progress to critical illness, ultimately leading to death. Why does this abrupt change occur during the 7–14 day period? Cytokine storm is a crucial and key pathogenic mechanism, as it leads to multi-organ dysfunction.
There have been numerous reports on patients with severe illness during the SARS, H5N1, MERS-CoV, and H7N9 outbreaks. In SARS patients, levels of IL-2, IL-10, IL-12, TNF-α, and IL-6 were significantly elevated. H5N1 infection was also associated with marked increases in various cytokines. A cytokine storm was likewise observed in H7N9 cases. Therefore, does SARS-CoV-2 infection truly induce a cytokine storm? We conducted studies to address this question by measuring cytokine levels in patients with severe and critical illness, and our findings revealed significant elevations in numerous cytokines.
We observed that cytokine storms were already significantly elevated during the early to middle stages of the disease in patients, with a marked increase in cytokine levels occurring in the second week after onset. If the cytokine storm could be suppressed during this period, patients might not progress to critical illness.
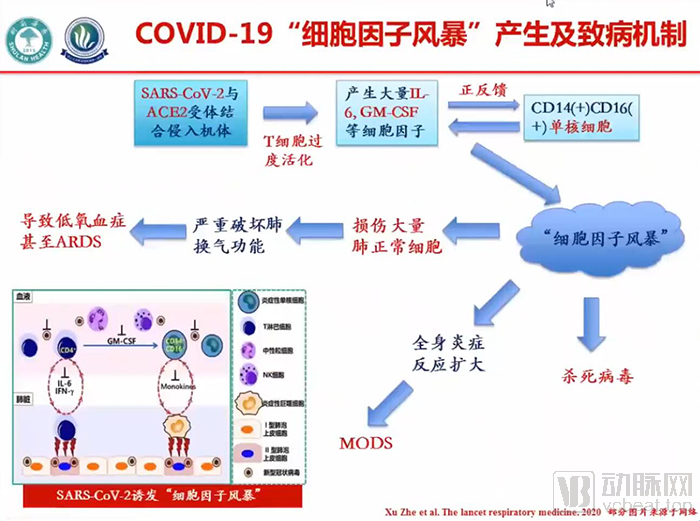
Image sourced from a screenshot of the conference’s live video stream
This is our understanding of the overall pathogenesis of cytokine storm. After binding to human ACE2 receptors, SARS-CoV-2 invades the body and causes excessive activation of T cells, leading to the massive production of cytokines such as IL-6 and GM-CSF. It can also establish a positive feedback loop with monocytes, further inducing substantial release of IL-6 and other cytokines, thereby triggering a cytokine storm.
Following the onset of a cytokine storm, which is initially intended to combat viral infection, excessive and massive inflammatory responses can damage normal lung tissue, impair pulmonary gas exchange, and lead to hypoxemia and Acute Respiratory Distress Syndrome (ARDS). Furthermore, systemic inflammatory responses can result in multiple organ failure. Therefore, the development of a cytokine storm represents one of the most critical pathogenic mechanisms underlying severe and critically ill patients.
Cytokine storms have been extensively studied, and as early as 2005, experts proposed therapeutic strategies targeting cytokine storms. These included recombinant receptor agonists, antagonists, and dimers targeting IL-1, IL-6, and IL-8; anti-TNFα monoclonal antibodies or soluble receptor agonists; and synthetic anti-TNFα agents. However, no clinical study results were available at that time.
Since the onset of the novel coronavirus pandemic, we have adopted many new approaches. As previously introduced by Academician Zhong, tocilizumab, as a component of immunotherapy, can effectively and continuously block the cytokine storm induced by IL-6. Currently, multicenter clinical trials on tocilizumab treatment are still underway.
Second, immunotherapy—specifically C5a monoclonal antibodies—is another approach. As is well known, C5a is a cytokine-like mediator involved in lung injury caused by highly pathogenic viral infections. By administering monoclonal antibodies against C5a, we may be able to block the cytokine storm. C5a-targeted therapies are being developed accordingly, and multi-center clinical trials of C5a monoclonal antibodies are currently underway, although results have not yet been fully released.
Historically, the common approach to suppressing cytokine storms has involved the judicious use of corticosteroids, which can provide a certain degree of suppression. Clinicians have accumulated extensive experience indicating that corticosteroids should not be administered in excessive doses or for prolonged periods. In particular, corticosteroids can inhibit immune responses, thereby delaying the clearance of SARS-CoV-2.
Xuebijing, a traditional Chinese medicine formulation composed of multiple herbal ingredients, can be used to inhibit systemic inflammatory response syndrome. Its key components include safflower, red peony root, Szechuan lovage rhizome, salvia miltiorrhiza, and angelica sinensis. This therapy has also been included in the seventh edition of the clinical diagnosis and treatment guidelines.
All medications have certain effects, but none can completely eliminate cytokines. We previously developed an artificial liver-based blood purification system, with research dating back to 1986. The artificial liver can effectively remove toxic substances such as bilirubin and endotoxins, as well as cytokines, during hepatic insufficiency. It demonstrates remarkable efficacy in managing hepatic insufficiency, significantly improving cure and recovery rates. This technology, known as "Removal of Inflammatory Mediators in Hepatic Insufficiency," has been promoted across hundreds of hospitals in 31 provinces and municipalities throughout China.
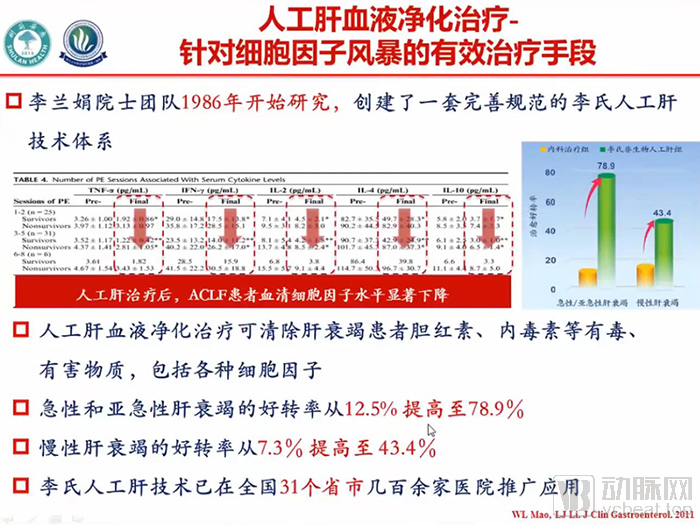
Image sourced from a screenshot of the conference’s live video stream.
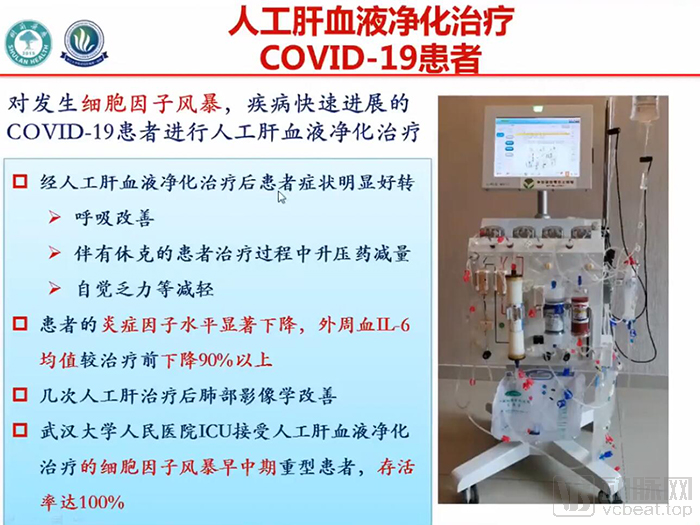
Image sourced from a screenshot of the conference’s live video stream.
This illustrates the fundamental principle of the artificial liver and the artificial liver machine. After separating blood cells from plasma, the plasma undergoes activated charcoal adsorption followed by filtration. This system effectively removes various inflammatory mediators from the patient’s blood, producing immediate therapeutic effects.
Artificial liver support systems are highly effective in treating cytokine storms associated with COVID-19. We have previously applied artificial liver support in managing H7N9-induced cytokine storms, which also proved to be highly effective.
This time, we applied the treatment to patients with severe and critical COVID-19-associated cytokine storms in Wuhan and Zhejiang Province. The artificial liver system can rapidly clear inflammatory mediators. Patients even experienced improved dyspnea halfway through the treatment course, allowing for a reduction in vasopressor dosage during shock management, along with significant alleviation of subjective symptoms such as fatigue. During treatment, levels of inflammatory mediators decreased markedly, with mean interleukin-6 (IL-6) levels dropping by approximately 90%.
After several sessions of artificial liver support therapy, pulmonary imaging showed significant improvement in inflammation. Notably, during treatment at Wuhan People’s Hospital, we found that early-to-mid stage application of artificial liver support achieved a 100% survival rate, successfully rescuing patients by suppressing cytokine storm.
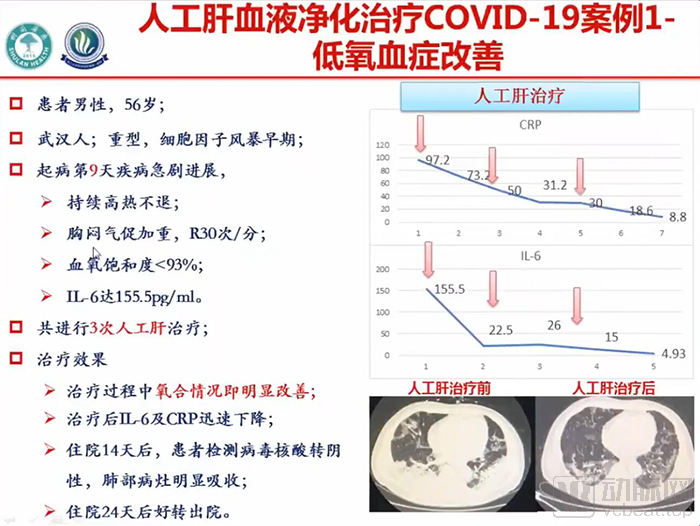
Image sourced from a screenshot of the conference's live video stream.
This 56-year-old male patient was diagnosed with severe COVID-19. He exhibited significantly elevated cytokine levels, with interleukin-6 (IL-6) reaching 155.5 pg/mL, which is 15 times the normal value. On day 9 of symptom onset, he experienced persistent high fever, chest tightness, and shortness of breath, with a respiratory rate of 30 breaths per minute and oxygen saturation below 93%. His IL-6 level had increased 15-fold. We administered three sessions of artificial liver support therapy. The patient’s oxygenation improved markedly, IL-6 and C-reactive protein (CRP) levels decreased significantly, and pulmonary inflammation was alleviated. After 24 days of hospitalization, he fully recovered and was discharged. As a healthcare professional himself, he also avoided more severe adverse outcomes.
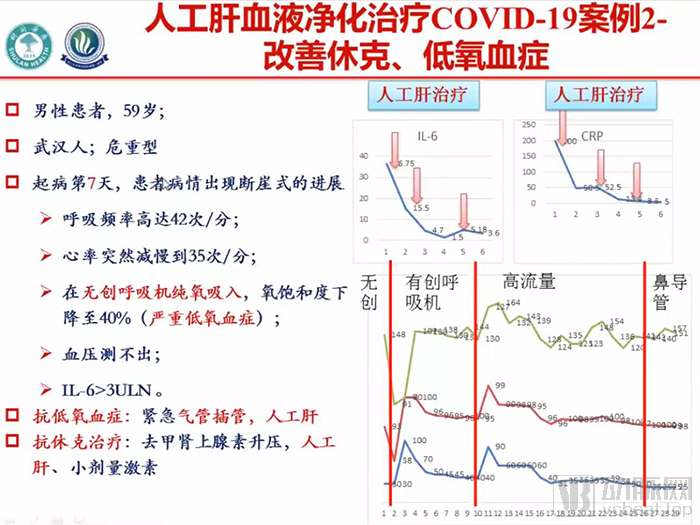
Image sourced from a screenshot of the conference's live video stream.
This is a 59-year-old patient with critical illness. On the 7th day of onset, the condition deteriorated precipitously: the respiratory rate suddenly surged to 42 breaths per minute, while the heart rate abruptly dropped to only 35 beats per minute. Despite receiving 100% oxygen via non-invasive ventilation, oxygen saturation fell to 40%. Blood pressure was unmeasurable, and IL-6 levels were more than three times the upper limit of normal.
In this emergency situation, on the one hand, we provided respiratory support using a ventilator; on the other hand, after several sessions of artificial liver therapy, his shock was gradually corrected. His cytokine levels decreased, blood pressure stabilized, and oxygen saturation improved.
Following the second session of artificial liver support, the patient’s oxygen saturation rose to 56%, and the endotracheal tube was extubated five days later. After three sessions of artificial liver treatment, the patient’s condition has largely stabilized, with improvement in pulmonary inflammation. The patient remains hospitalized and is aware that he was pulled back from a life-threatening situation.
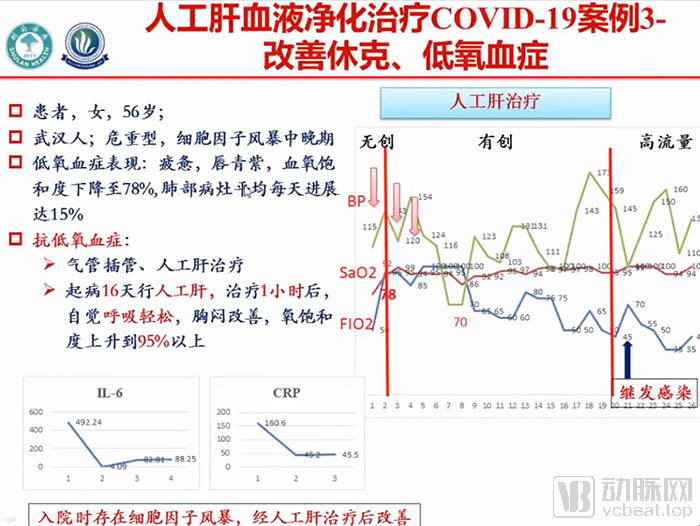
Image sourced from a screenshot of the conference's live video stream.
This is a 56-year-old female patient with critical illness. Artificial liver support was not administered in the early stage; we determined that she had progressed to the middle-to-late stage, exceeding 15 days of disease duration. Artificial liver therapy was initiated on day 16, and her condition, including dyspnea, showed some improvement. However, due to the delayed initiation of artificial liver support, she developed acute sepsis caused by Acinetobacter baumannii, leading to sudden dyspnea, coma, mydriasis, and absent pupillary light reflex.
In such a severe condition, we immediately administered several sessions of artificial liver support therapy, maintained the regulation of her gut microbiota, and provided stem cell therapy. After three sessions of artificial liver treatment, the patient gradually regained consciousness ten days later and was progressively weaned off the ventilator. She remains hospitalized at present. Upon our recent visit, she tearfully expressed her gratitude via mobile phone, deeply moving us; she has been given a second chance at life.
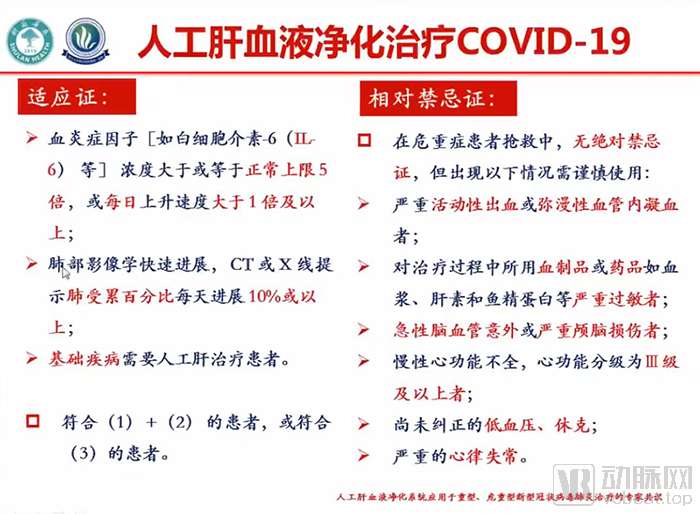
Image sourced from a screenshot of the conference’s live video stream.
The preceding sections have presented various case studies. The application of artificial liver blood purification is highly effective in the early stages of cytokine storm. The primary indications include patients with cytokine concentrations exceeding five times the upper limit of normal, or increasing by more than 100% per day, as well as those exhibiting daily progression of chest X-ray findings by more than 10%. We believe that such patients should receive treatment with artificial liver blood purification. This therapy can reduce the probability of disease progression to critical illness by 16%.
We have now issued a national expert consensus, which has also been incorporated into the national diagnosis and treatment guidelines.
Overall, we believe that cytokine storm is a key factor in the progression of COVID-19 to severe disease. Clinical trials of monoclonal antibodies, C5a antibodies, and stem cell therapies are underway and represent rapid and effective approaches.
Artificial liver blood purification can clear inflammatory mediators, block cytokine storms, and prevent the progression of severe cases to critical conditions, significantly improving the success rate of treatment for severe and critically ill patients.
Following Academician Zhong Nanshan and Academician Li Lanjuan’s presentations on the diagnosis and treatment of COVID-19, as well as their experiences in managing cytokine storm and critical care for severe cases, the conference proceeded to its second agenda item: a roundtable forum on the exchange of experience in COVID-19 prevention and control.
The first session of the roundtable forum was moderated by Mr. Wu Wenda, Vice President of Tencent Healthcare. Participants who joined the forum and delivered speeches included Academician Zhong Nanshan, Head of the High-Level Expert Group of the National Health Commission; Academician Li Lanjuan, Member of the High-Level Expert Group of the National Health Commission; Professor Liu Guoen from the National School of Development at Peking University; Mr. Luo Yongqing, Global Vice President and General Manager of China Region at Gilead Sciences; and Mr. Xin Lijun, CEO of JD Health.
Below is an abridged transcript of the roundtable discussion.
Academician Li Lanjuan
I believe this outbreak represents a newly emerging infectious disease. The primary challenge lies in how to bring the epidemic under control and prevent and curb its spread. Academician Zhong has just provided an excellent overview of this aspect. In my view, our most critical measures are to identify and control sources of infection, interrupt transmission routes, and protect susceptible populations. To identify sources of infection, testing is essential; following detection, cases should be isolated and treated.
The General Secretary put forward the principle of “testing all who should be tested and treating all who should be treated.” These eight characters are of paramount importance. In the early stages, when I arrived in Wuhan, there were significant difficulties in conducting large-scale testing and providing medical care. However, within just a few days, our country mobilized more than 40,000 medical personnel to Wuhan, and makeshift hospitals were gradually put into operation. Beds in all major hospitals were made available to treat critically ill patients, while makeshift hospitals were designated for those with mild symptoms, thereby rapidly resolving the issue. Consequently, once the source of infection was brought under control, the rate of new infections dropped substantially. This is the most critical point.
The second preventive measure, as mentioned by Academician Zhong, is to wear masks, reduce interpersonal contact, minimize transmission, and cut off the routes of spread.
Furthermore, regarding treatment, all patients should receive proper management of their disease. Academician Zhong previously introduced several antiviral medications, which I consider to be highly important. Antiviral therapy can shorten the course of the disease and prevent mild cases from progressing to severe illness.
Third, in the treatment of critically ill patients, we need to block the cytokine storm pathway to reduce the incidence of critical cases and the case fatality rate. The situation was quite dire when we first arrived in Wuhan; however, medical teams quickly arrived, and medical resources—including oxygen supplies, ventilators, and artificial liver support systems—became available, leading to a significant drop in the case fatality rate. As a result, the epidemic in Wuhan was basically brought under control within just two months.
Academician Zhong Nanshan
"In my view, given the current global situation and drawing on China’s recent experience, implementing citywide lockdowns in high-risk areas, along with promoting social distancing and mask-wearing, is undoubtedly the most effective approach to prevent further viral spread."
I am currently concerned that the disease is spreading rapidly in some countries, with 10,000 new cases reported in a single day—such surges can indeed be that severe. Consequently, the large number of patients places an enormous burden on healthcare systems. The shortage of hospital beds, medical facilities, and healthcare professionals creates a more detrimental vicious cycle.
Furthermore, cases have been reported in more than 200 countries and regions. If some major powers fail to contain the outbreak, it will bring disaster to the entire world; no country can remain unaffected. This is my greatest concern.
We are currently making every effort. Based on current data, remdesivir is effective. Although it is not a highly specific targeted therapy, it does shorten the duration of the disease. Additionally, chloroquine and hydroxychloroquine have both demonstrated favorable efficacy. I have recommended hydroxychloroquine to some patients in the United States, including friends of mine, and it has proven effective. Within a few days, their viral loads turned negative.
Liu Guoen, Boya Distinguished Professor at the National School of Development, Peking University
First, humanity currently faces the ongoing risk of the global spread and surge of the COVID-19 pandemic. As Academician Zhong just mentioned, today’s figures are approaching one million, with 938,000 confirmed cases and 47,272 deaths. Based on my calculations, the case fatality rate stands at 5%, reflecting today’s data.
Against this backdrop, on the one hand, we should follow the technical guidance provided by the experts just mentioned, particularly those who have recently been engaged in frontline epidemic prevention and control work. On the other hand, we must avoid causing them unnecessary disruption and refrain from triggering unwarranted, blind panic within this broader context. Such actions would not be conducive to our epidemic prevention and control efforts.
I raise this point to encourage everyone to consider how a systematic pathway analysis might enable us to better assess the overall situation in the face of the current epidemic. Why is this the case?
Let me share a set of figures with you, based on the weekly mortality curves published by the U.S. CDC in recent years and their comparison with the situation in 2020. I am presenting this information because China’s data are not as comprehensive, nor are they released to the public as promptly. In contrast, U.S. data are highly complete; therefore, I will use the United States as an example to illustrate my point.
From 2015 to 2019, including January 2020, weekly data over the past few years show that the average total number of deaths from all causes in the United States during the first week of January was 60,000. Over the previous five years (2015–2019), the average number of deaths continued to decline, reaching approximately 60,000 by around the 10th week.
The 2020 figures reveal a noteworthy issue that warrants our attention and reflection. The latest data from the 10th week of 2020 show that the total number of weekly deaths in the United States from all causes combined was approximately 47,000, which is exactly 13,000 fewer than the average for previous years. This is because the United States has recently begun to implement substantial control measures across major cities.
Why did the death toll actually decrease? It was because everyone stayed at home and avoided going out, which reduced deaths from other causes that occur under normal circumstances. For example, deaths due to COPD caused by air pollution, or fatalities from car accidents, among others.
In fact, under conventional conditions in the past, these causes were major killers across our broader societies. Taking China’s official 2017 statistics as an example, among the top six leading causes of death, stroke ranked first, ischemic heart disease second, lung cancer third, air pollution and respiratory-related chronic obstructive pulmonary disease (COPD) fourth, liver cancer fifth, and road traffic injuries sixth. This helps explain why staying at home during lockdowns could significantly reduce the substantial casualties caused by these factors.
From this perspective, while we are responding to the assault of the current major disease, we should also recognize that, under normal circumstances, humanity is constantly accompanied by significant threats of mortality.
With the pandemic brought under control, we are better positioned to reflect on these issues. On one hand, this helps reduce the unnecessary and unfounded fear we face in the current exceptional circumstances; on the other, it enables us to think more systematically about how to better safeguard public health.
This is my first point: adopting a systemic mindset to address the current situation may help us better prevent and control this epidemic.
Given my background in economics, the second point I wish to address is the impact of epidemic prevention and control measures on the economy. In general, I am reluctant to conduct such an assessment, as our current prevention and control efforts are still ongoing, making any evaluation at this stage scientifically premature. However, in response to widespread requests, I will attempt a preliminary assessment, which should be regarded as highly tentative.
Here is a set of figures: The Financial Times has conducted a highly systematic tracking of six major economic indicators for China. These six indicators include real estate sales volume, traffic conditions in major cities, coal consumption for power generation, container freight volume, nationwide box office revenue, and pollution levels in the ten largest cities. Collectively, these six indicators largely reflect the state of China’s economic performance, and they are aggregated to form a composite index.
What we are seeing now is that, with January 2020 set as the baseline index of 100, where does this index currently stand? It hit its lowest point in late February to early March, when the epidemic was at its most severe, dropping below 60%. As the economy begins to recover gradually, the index has rebounded to slightly above 60%. In other words, based on the economic performance reflected by these six major indicators, the current level is approximately 60%.
If we base our estimates on this figure, assuming that the current level of work resumption is approximately 60%, and then conduct a macroeconomic assessment, what would be the approximate economic loss over the past three months, as measured by GDP?
Here is my calculation. In the first quarter of 2019, China’s GDP stood at RMB 21.3 trillion. Assuming the pandemic had not occurred and maintaining a normal growth rate of 6%, the GDP for the first quarter of 2020 would logically have reached RMB 22.6 trillion. However, the pandemic did occur. Based on the assessment of the six indicators mentioned earlier, if 60% of enterprises could resume operations at their original locations today, we could avoid losses amounting to RMB 13.6 trillion. What does this figure imply? The combined annual GDP of Beijing, Shanghai, Guangzhou, and Shenzhen last year was RMB 12.4 trillion. This means we would effectively recover an amount equivalent to the entire annual GDP of these four major cities.
Suppose we are unable to achieve a 60% operating rate and can only operate at 50%; even so, we could avoid losses of at least RMB 11.3 trillion. To put this in perspective, the combined GDP of Beijing, Shanghai, Guangzhou, and Tianjin is approximately RMB 11.1 trillion. Furthermore, when considering the adverse effects of the pandemic on our savings, investment, and capital markets, the long-term losses would be even greater. This is my preliminary estimate for your reference.
Third, our response to this epidemic must begin in China. The outbreak has now spread to major developed countries and regions, including the United States, Europe, Japan, South Korea, and Singapore. I wish to discuss this matter with you all, hoping to draw the high attention of the entire international community.
If you look at the latest epidemic map from yesterday, South Asia, Africa, and South America currently show only small clusters of red dots, with no large-scale outbreaks yet. However, this does not mean that major outbreaks similar to those in China, the United States, and Europe will not occur in the future.
The current resilience and economic affordability of the healthcare systems in these regions are not even a fraction of those in developed countries. Should an epidemic outbreak occur, it would likely result in significant mortality among the population in these areas.
Once they start moving around again, the impact on all of humanity will be immeasurable. Therefore, we still have time. I believe we must contemplate this issue regardless, because we live in a global village, and no one can escape it. This is critically important. Once an outbreak occurs, there will be nothing we can do. Do you think they can endure one or two months without resuming work? That is impossible. So, what should be done? This brings me to my third point.
I noted that yesterday, 20 leading economists worldwide, including numerous Nobel laureates, jointly signed a letter addressed to the World Bank and the World Health Organization, urging them to prioritize this issue. I am also raising this matter specifically here today. This is not merely their concern; if they fail to resolve it, other middle-income countries and developed nations will have to contend with this problem over the long term.
Mr. Luo Yongqing, Global Vice President of Gilead Sciences and General Manager of China Region
First, please allow me to extend the highest respect and heartfelt gratitude on behalf of Gilead Sciences to the vast number of healthcare professionals who have dedicated themselves to the fight against COVID-19!
Gilead Sciences has remained dedicated to the research and development of antiviral therapeutics. Over the past three decades, we have developed more than 20 iterations of medications for the treatment of hepatitis B, hepatitis C, and HIV/AIDS.
Remdesivir is an investigational antiviral drug that we began developing more than a decade ago. At the onset of the novel coronavirus pneumonia outbreak, we had already hypothesized that this drug might be effective against the virus. This assumption was based on our findings during the development of remdesivir, which demonstrated potent antiviral activity against SARS-CoV and MERS-CoV in both in vitro and animal models.
In early January, researchers identified the novel coronavirus. It shares significant structural similarities with the two viruses mentioned earlier. Since then, our entire team has been working around the clock, proactively engaging with researchers from the WHO, the United States, China, and Europe, in an effort to determine the safety and efficacy of remdesivir in treating COVID-19 through clinical trials.
There is significant interest in the clinical trials we are currently conducting, and I will provide an update here.
Currently, more than 10 countries and regions worldwide are participating in six international studies on the use of remdesivir for treating novel coronavirus pneumonia. These include two randomized, double-blind, controlled trials conducted in China to evaluate the safety and efficacy of remdesivir in COVID-19. Also included are two other studies: one initiated by the U.S. National Institute of Allergy and Infectious Diseases (NIAID), and another led by the World Health Organization (WHO) and conducted in France.
We have also launched two studies to evaluate the safety and efficacy of remdesivir. Currently, more than 70 institutions and hospitals worldwide are participating, with over 2,000 patients enrolled.
Currently, we are still conducting clinical trials and have not yet received formal approval. Nevertheless, as early as February, we began organizing our global supply chain with the aim of expanding production capacity. Due to the urgency of the pandemic, we made significant investments even before the publication of clinical data or regulatory approval. We hope that once the product is approved, we can deliver it to various parts of the world as quickly as possible, thereby providing support to governments, healthcare workers, and patients in improving disease outcomes.
Regarding the accessibility of remdesivir, we aim to expand production capacity after drug approval to ensure its affordability and accessibility. Since its inception, Gilead Sciences has adhered to a patient-first philosophy. This case is no exception; we will ensure its affordability and accessibility.
Xin Lijun, Vice President of JD.com and CEO of JD Health
I will now provide a report to all friends on the work carried out by JD.com and JD Health since the onset of the pandemic, as mentioned earlier.
Since the onset of the pandemic, the entire JD Group and JD Health have been fully mobilized at the earliest opportunity under the unified command and coordination of Mr. Richard Liu, founder of JD.com, implementing a series of effective measures in a focused and stepwise manner.
Since the onset of the pandemic, JD Health has fully leveraged JD.com’s overall intelligent supply chain advantages to maximize its capabilities in the circulation and supply of medical resources, including pharmaceuticals and medical devices. As China’s largest retail platform, we have implemented comprehensive measures across sourcing, warehousing and distribution, and platform oversight to ensure a stable supply and pricing of protective equipment such as face masks.
This is critically important. Products from our partner manufacturers can move directly from the factory production lines into warehouses and be delivered to consumers at the fastest possible speed. In January alone, JD Health procured more than 30 million units of various epidemic prevention supplies, including pulse oximeters, thermometers, and ventilators, to meet the nationwide demand for protective equipment against the pandemic. We also prioritized the donation and delivery of medical supplies to frontline hospitals such as Wuhan Union Hospital and Tongji Hospital to support their epidemic prevention and control efforts.
Since late January, people across China have actively responded to the call from the government and experts by implementing home-based prevention and control measures, with many regions imposing traffic restrictions. However, public demand for medical and health services has not ceased due to home isolation. Notably, experts have pointed out that COVID-19 closely resembles influenza in its early stages. Against this backdrop, JD Health has fully leveraged the advantages of its internet platform, mobilizing capabilities across all segments of its service supply chain to proactively provide online consultations, prescription renewals, and door-to-door medication delivery.
Starting January 26, JD Health launched the “Prevention and Control of Novel Coronavirus Pneumonia” free online consultation platform, taking the lead in the internet sector by expanding its free consultation services to cover all diseases across all medical specialties. Meanwhile, we have invited academicians such as Han Demin and numerous experts, together with more than 30,000 full-time and part-time physicians, to provide online services and offer free professional consultations to users nationwide. From the onset of the epidemic until yesterday (April 1), JD Health’s online consultation platform had served nearly 8 million user visits, with daily consultations exceeding 120,000, significantly alleviating users’ needs for medical consultations and psychological counseling during periods of reduced outdoor activity.
While supporting epidemic prevention and control efforts, JD Health has also paid close attention to patients with chronic diseases, as this group is required to self-isolate at home and faces difficulties in going out during this period. We have launched the "Chronic Disease Care Program," enabling patients with chronic conditions to undergo follow-up consultations and obtain prescriptions through our online consultation platform.
Meanwhile, we have partnered with more than 70 Chinese and international pharmaceutical companies, including Gilead Sciences, where Mr. Luo is affiliated, to jointly ensure the medication supply for patients with chronic diseases. Medications can be delivered directly to users via JD Logistics, enabling convenient and timely online follow-up consultations and prescription purchases from the comfort of home.
What is particularly noteworthy is that the team includes 38 physicians who served on the front lines of epidemic treatment in Hubei Province, along with more than 30 experts in Traditional Chinese Medicine (TCM). We have provided numerous solutions, including TCM therapies such as Lianhua Qingwen Capsules mentioned by Academician Zhong, and used this platform to share anti-epidemic experiences and protective knowledge with overseas communities.
As of April 1, the platform had collected more than 130,000 overseas medical consultation inquiries in total. Among these, over 8,100 were in English, and the number of visits exceeded 5.85 million.
After two months of nationwide epidemic prevention and control efforts, it is evident that the value of internet healthcare has gained increasing recognition from both the public and the government. We hope that countries with the necessary conditions will draw on the “China experience,” fully leveraging the advantages of “contactless services” offered by internet platforms during epidemic containment and prevention, to help address people’s healthcare and related needs while they remain at home for protective measures.
Mr. Cao Kefan, Image Ambassador of the China Primary Health Care Foundation
First, I believe the most critical role of the media throughout the epidemic prevention and control process is to provide the general public with timely and accurate information. Given the widespread use of the internet and self-media, people are often exposed to varying pieces of information on social media platforms such as WeChat Moments. The public genuinely seeks the most accurate information. As Academician Zhong noted, we release daily updates on confirmed cases and new infections through mainstream media channels, enabling ordinary citizens to stay informed about the progression of the epidemic across China, particularly in Wuhan.
Second, mainstream media outlets such as China Central Television (CCTV) and Dragon TV have continuously invited frontline experts, including Academicians Zhong Nanshan and Li Lanjuan, to provide updates on epidemic prevention and control, thereby guiding the public to stay promptly informed about relevant measures in their daily lives.
Third, public welfare organizations such as the China Primary Health Care Foundation can leverage the abundance of medical resources available during the pandemic. For instance, events like today’s gathering bring together numerous medical experts to share their clinical experiences and research findings.
As Academician Zhong just explained, China was able to achieve phased success in epidemic prevention and control within such a short period primarily due to two key factors: First, a decisive choice was made to adopt suppression—a stringent measure—rather than mitigation, despite its significant economic impact. Second, maintaining social distancing and wearing masks proved to be critical measures in reducing the risk of transmission. Third, he shared certain clinical approaches used to rapidly achieve viral clearance in patients with mild or ordinary cases, thereby preventing their progression to severe or critical conditions.
I believe that both the media and public welfare organizations have delivered excellent results during the pandemic. In the future, our media outlets and public welfare organizations can draw on this epidemic prevention and control effort to provide greater guidance for their work going forward.
Following the presentations by Chinese experts, the roundtable discussion moved into its international exchange session. This segment was moderated by Ms. Fang Jun, founder and director of the Health China International Public Health Management Training Program. Professor Soonman Kwon, Dean of the School of Public Health at Seoul National University; Dr. Naveen Rao, Senior Vice President of the Rockefeller Foundation; and Dr. Welte Tobias, advisor to the German government on the COVID-19 pandemic, participated in the roundtable and delivered remarks in turn.
Below is the transcript of the roundtable discussion.
Dr. Tobias Welte, Advisor to the German Government on the COVID-19 Pandemic
The situation in Europe differs from that in the United States, with Southern Europe potentially facing more severe conditions than Northern Europe. Southern European countries such as Italy and Spain have experienced trajectories somewhat similar to Wuhan’s, characterized by a rapid surge in cases at the onset of the outbreak, a substantial increase in patient numbers, and an overwhelmed healthcare system due to insufficient ICU capacity. Consequently, these countries are currently grappling with significant challenges.
Nordic countries had certain advantages, as the outbreak occurred 3–4 weeks later than in Southern Europe, allowing them more time to prepare. Some Northern and Central European countries, such as Germany, Austria, and Switzerland, also had significantly richer medical resources compared to their Southern European counterparts. Therefore, preparedness was more adequate in these regions. They also implemented certain lockdown measures, drawing reference from China’s experience. As a result, the case fatality rate in Northern and Central Europe was much lower than that in Southern Europe.
Currently, most European countries have implemented various forms of lockdown measures and adopted the preventive strategies mentioned earlier by our Chinese colleagues. Social contact has been significantly reduced, with schools and kindergartens closed. Many individuals are also self-isolating at home. As a result, the rate of new case increases is now declining. Although we have not yet reached the peak or the plateau phase, the doubling time for cases has extended from three days to ten days. I hope this trend will continue.
On April 20, three weeks later, Germany will partially lift its lockdown measures, though this remains contingent on developments in the coming days.
Regarding treatment, we are not particularly optimistic—certainly not as optimistic as Chinese PhDs. Chloroquine may not be highly effective, whereas remdesivir appears to be more promising. We have already initiated several research projects. Randomized, double-blind, controlled trials are now underway across various European countries, and the clinical trials mentioned earlier have been launched throughout Europe.
Dr. Naveen Rao, Senior Vice President of the Rockefeller Foundation
The number of cases in the United States is rising, with 216,000 confirmed cases and over 5,000 deaths. The figure in New York is also relatively high, with 1,921 deaths. Currently, we are observing a daily growth rate of 32%. In terms of case fatality, approximately 250–300 people die each day. Thus, the growth rate remains high, at around 31%, indicating a very steep upward trend.
We have also implemented many measures similar to those just mentioned, such as social distancing and lockdowns. However, you know that these measures are very stringent, effectively confining everyone. Some individuals may not be at high risk, while others belong to susceptible populations. We are now considering how to adopt a dual-pronged approach moving forward, which may involve conducting acute-phase testing for patients with acute conditions and implementing antibody testing to determine who has developed immunity and who has been infected, thereby enabling these individuals to return to work as soon as possible. Should vaccines become available in the future, we will also be better positioned to identify which individuals would benefit from them.
We know that pandemics cause deaths in three ways. The first is direct mortality from the virus itself. The second results from healthcare systems being overwhelmed, leading to deaths such as those of children, maternal deaths during childbirth, or fatalities from other conditions. For instance, during the 2014–2015 Ebola outbreak, local healthcare systems were overstretched, and more people died from malaria than from Ebola directly. The third category comprises deaths caused by economic problems, essentially poverty-related mortality. This impact is particularly severe for vulnerable populations and the poor. Thus, pandemics primarily claim lives through these three mechanisms.
We are currently focused on the virus's lethality; next, we must ensure that patients do not die due to an overwhelmed healthcare system.
Third, we must ensure that vulnerable and impoverished populations do not fall into the worst possible circumstances due to economic constraints. We need to employ various methods for treatment through Ebola-style prevention and control measures, such as increased social distancing, early detection, and early isolation. Given the high likelihood of recurrence in the following year, epidemic prevention and control should be approached similarly to influenza management. Therefore, we need to achieve 60%–70% herd immunity, handling the situation in a manner analogous to influenza control.
We know that the peak of the outbreak has not yet arrived. April will be a particularly critical month for us, but we will strive to do our utmost. We also sincerely appreciate everyone’s concern and support!
Professor Kwon Soon-man, Dean of the Graduate School of Public Health at Seoul National University
South Korea has managed to control the situation well, primarily due to three key factors that proved effective at a very early stage.
First, act early. We should not fear overreaction, as it is always better than underreaction. In late January, when we had fewer than 10 confirmed cases, the government already instructed us to take action and prepare test kits. Accordingly, we produced the relevant kits in compliance with governmental directives. The government granted production approvals at a very early stage, initiated production work promptly, and also mandated large-scale testing.
At that time, we were not actually certain whether this approach was correct, as it involved a large number of people. The confirmed case count surged abruptly due to mass testing. Of course, one of the primary drivers of this surge in confirmed cases was activities associated with the Cheonji Church.
It is precisely because of large-scale testing that many people have been able to quickly access hospital treatment. The government has also provided a clear prioritization plan: patients with severe conditions require hospitalization, while those with mild cases are directed to use hotels and other facilities for home isolation or home-based treatment, with medical staff assigned to provide relevant care.
Large-scale testing enables us to effectively identify and isolate cases, ensuring that patients with severe illness receive timely and effective treatment.
Initially, during the testing process, we encountered situations where patients undergoing testing caused contamination of the entire testing site. In such cases, the contaminated areas had to be fully quarantined. For instance, some drive-through rapid testing sites identified confirmed cases, necessitating their closure and implementation of corresponding quarantine measures.
Third, I would like to discuss contact tracing. South Korea did not implement any citywide lockdown measures; all businesses remained open, and airports continued to operate. Of course, starting yesterday, we have also required all inbound travelers to undergo a 14-day quarantine. Prior to this, our approach was relatively open. We did not impose a lockdown, but we adopted a highly aggressive strategy in contact tracing, which has proven to be very effective.
We can intervene with patients after case detection by examining their mobile phones, GPS data, and movement trajectories, and even reviewing various surveillance footage to trace their whereabouts. This would likely be unfeasible in Western countries.
Five years ago, South Korea became a hard-hit area for MERS. At that time, many people died due to inadequate contact tracing. This time, thanks to our aggressive yet effective tracing efforts, we have been able to contain the spread of the epidemic very effectively. Therefore, I believe that on one hand, we can choose to impose a citywide lockdown; on the other hand, we can choose not to lock down, but we must incur significant costs to conduct thorough contact tracing.
The government also sent messages to all citizens, detailing locations visited by confirmed cases. Individuals who had contact with these confirmed cases or had visited the disclosed locations were required to take appropriate measures. While this proactive tracing method did have some impact on us, it represented a viable option. Such measures can only be truly effective with the consensus and cooperation of the entire society. Lockdowns have their advantages, but they come at a significant economic cost.
I believe Japan and South Korea share certain similarities. We have conducted relevant public awareness campaigns urging people to wear masks, wash their hands frequently, and maintain social distancing. In South Korea, if you walk down the street or are in a public space without wearing a mask, many people will point at you and remind you to put one on. It is precisely this sense of civic duty and shared social responsibility that has enabled government policies on social distancing to be truly effective.
Dr. Tobias Welte, German Government Advisor on the COVID-19 Pandemic
Implementing close contact tracing in most European countries, including Germany, is difficult to carry out. On one hand, it contravenes existing practices in various countries; on the other, many people are concerned that it infringes upon individual freedoms. Of course, how the situation evolves will also depend on the duration of the pandemic.
If the current city lockdown measures continue for another 6–8 weeks, the public will be unable to cope; it is imperative to ensure a return to normalcy within the next two months. Thereafter, discussions must commence on which approaches are most effective in restoring everyday life to its pre-pandemic state. At that point, real-time tracking may be considered and potentially accepted by the public. This outcome will depend on how the case numbers evolve over the next two weeks.
Dr. Naveen Rao, Senior Vice President of the Rockefeller Foundation
The situation in the United States is very similar. Overall, there is widespread reluctance to adopt highly aggressive contact tracing measures, as they raise concerns regarding privacy and data security. Public awareness of these issues is strong, and opposition is inevitable.
We are also aware of the contact tracing measures implemented for close contacts of confirmed cases in South Korea and Singapore. We fully recognize that these approaches have been highly effective. However, we understand that it would be quite difficult to gain public acceptance in the United States for comprehensive tracking of all credit card records. It remains unclear whether Americans are currently willing to embrace such aggressive contact-tracing measures.
Academician Zhong Nanshan
I fully understand, and the points just made by the Korean professor are also very valid. Having learned valuable lessons from the MERS outbreak, during which more than 30 healthcare workers were infected, they have a clear understanding of how to respond when an epidemic occurs. This is particularly crucial given that the severity of the current novel coronavirus far exceeds that of MERS. Therefore, their approach to large-scale, close-contact tracing has been exemplary.
Circumstances vary from country to country. China is now capable of conducting large-scale screening, and we must also carry out large-scale screening.
Another point is that we have identified some patients who have tested negative for the virus and are asymptomatic, yet may still transmit the virus further. It is crucial to track these individuals. Therefore, I strongly agree with Mr. Rao from the United States regarding his observation of the significant surge in patient numbers in recent days.
Now, the United States has also begun large-scale screening. I understand that the methods are highly advanced, with screening results available in approximately 15 to 50 minutes. In China, it takes about one and a half hours to obtain screening results. It is excellent that you have such machines capable of high-throughput, rapid viral nucleic acid testing, delivering results within 15–20 minutes. This will also enable you to quickly identify infected patients.
I would like to raise a point regarding how to isolate these individuals. We need to monitor symptomatic individuals, but what about those who are asymptomatic? In fact, they are highly contagious, which poses a significant challenge. This is a major issue in the context of human-to-human transmission. I believe we need to take further measures to focus on confirmed patients who test positive for nucleic acid. It is crucial to implement measures to prevent them from causing further spread.
In particular, we believe it is crucial to prevent the spread to several states in the southern United States, and measures must be taken to avert this scenario. Otherwise, while the United States possesses advanced technological capabilities to identify cases through sophisticated methods, decisive actions—such as isolation and increased social distancing—must be implemented upon detection. These measures need to keep pace, which is what I am considering.
Remdesivir has demonstrated some efficacy, as evidenced by our research studies. However, prevention is of paramount importance. I am somewhat concerned about the situation unfolding in the United States, given that challenges facing the U.S. have global implications. With daily case counts reaching 10,000, the federal government must implement more robust measures.
Dr. Tobias Welte, Advisor to the German Government on the COVID-19 Pandemic
The key point is to improve communication. If I were to highlight three things, they would be communication, communication, and more communication. Today’s meeting was excellent, providing us with an opportunity to exchange experiences and share our data.
We have encountered a wide variety of challenges, necessitating collaborative efforts in research and development as well as exchanges and cooperation in clinical trials. The COVID-19 pandemic should foster greater global unity, enabling us to jointly advance R&D initiatives and implement diverse measures in concert. This represents the most significant silver lining emerging from this disaster.
Dr. Naveen Rao, Senior Vice President of the Rockefeller Foundation
How can personal protective measures and supply chains ensure the cross-border flow of relevant goods, thereby enabling countries to collaborate more effectively rather than acting in isolation and managing their own affairs separately?
Second, we need global data. It is not enough to merely analyze global data as is currently done; we must also understand the underlying significance of the data and conduct appropriate stratification. The situation in Africa remains relatively favorable at present; however, should an outbreak occur there, it would become a critical priority for global collaboration.
Therefore, thirdly, we must provide rational assistance to Africa.
Professor Kwon Soon-man, Dean of the School of Public Health, Seoul National University, South Korea
I agree with my two colleagues that communication is extremely important. Given the critical role of collaboration, we hope to see joint efforts among nations in disease prevention and control as well as drug development. We also encourage policymakers to engage in dialogue to identify which policies are effective. This is also of great importance.
Academician Zhong Nanshan
I fully agree with everyone’s views. Collaboration is crucial, and communication must remain seamless. Therefore, we are maintaining close communication with our colleagues in Europe and the United States to exchange insights on prevention and control efforts, including the differences between COVID-19 and influenza. We are also conducting clinical trials, and the results will be released soon. We need to identify which drugs are truly effective and which have at least partial efficacy. We are currently working extremely hard, hoping to make progress in our endeavors.
Vaccines are also a key focus of our collaboration. We have already commenced Phase I clinical trials. It remains uncertain which country will be the first to develop a vaccine. In any case, we welcome advancements and progress made by any nation in this field, as such achievements would benefit the entire globe and all of humanity. Therefore, cooperation is the central message I wish to convey.
At the conclusion of the conference, Mr. Cao Xirong, Chairman of the China Primary Health Care Foundation, delivered closing remarks. He stated that whether drawing on countries’ experiences in pandemic control, leveraging the latest research on diagnosis and treatment, or strengthening joint prevention and control measures and international cooperation during the outbreak, such efforts are crucial to curbing the global spread of the epidemic. He expressed confidence that these vital insights and experiences would provide significant guidance for China’s ongoing consolidation of its pandemic control achievements and for assisting many countries around the world in overcoming the epidemic.
As the organizer of the Health China International Public Health Management Training Program, the China Primary Health Care Foundation has been committed to advancing China’s healthcare and medical services since its establishment in 1996. Leveraging its organizational strengths as a public fundraising foundation and social welfare platform, it has extensively mobilized and pooled charitable resources from across society to support primary health care initiatives.
During the fight against the COVID-19 pandemic, the China Primary Health Care Foundation actively raised and coordinated resources, providing critical support in the form of scarce supplies to affected regions. As of March 27, the Foundation had donated over RMB 22.92 million in cash, along with medical supplies including face masks, protective suits, and various medical materials—such as large-scale medical equipment—valued at RMB 746.67 million.
In active response to the World Health Organization’s call for enhanced experience sharing among nations, Chairman Cao Xirong announced the launch of the “Healthy China International Public Health Management Training” program, tailored specifically for frontline clinical personnel. By promptly summarizing lessons learned from the fight against the COVID-19 pandemic and guiding the study of theoretical frameworks in international public health management, this initiative aims to enhance the public health awareness and competencies of healthcare administrators and medical professionals, thereby fostering the development of societal public health management systems.
The training course adopts an online bilingual instruction format, with content comprising four modules: “Overview of Public Health and Prevention and Control of Healthcare-Associated Infections,” “Latest Applications of New Technologies in the Prevention and Control of Major Epidemics,” “Medical Humanities and Doctor-Patient Relationships,” and “The Responsibilities of Chinese Healthcare Professionals and New Media Communication Management in the Context of Globalization.” The program consists of two classes per week, totaling 16 classes and four discussion sessions, all of which will be offered free of charge to healthcare professionals worldwide.