Innovative Health Tech Firms like WeDoctor, Yunhu Yijian, and Jianjian Home Doctor Seize the Spring of Public Health Screening
As the COVID-19 pandemic served as a wake-up call for national and public health, it has become imperative to reflect on how to strengthen China’s public health service system. As a key component of this system, the National Basic Public Health Services serve as the first line of defense in enhancing emergency response capabilities for public health incidents and safeguarding residents’ health.
The National Health Commission’s relevant regulatory documents explicitly state that the funding required for the Basic Public Health Services Program is primarily borne by the government, with urban and rural residents directly benefiting.
Basic public health services are primarily delivered by primary healthcare institutions and constitute the foremost of the three core responsibilities of family doctors at the grassroots level. However, due to the overall weak capacity, staffing shortages, and inadequate equipment in these primary healthcare institutions, this people-centered initiative—a key measure under the “Healthy China” strategy—has not been fully implemented, becoming a significant pain point for health authorities at all levels. Consequently, enhancing the services provided by grassroots family doctors from the three dimensions of operational efficiency, service standardization, and residents’ sense of gain has become the most urgent priority for health commissions and healthcare service providers alike.
Leveraging multi-dimensional data and focusing on the core component of basic public health services—public health examinations—we analyze three major pain points in this sector. By evaluating representative products and project performance in the market, we identify the most effective current solutions and assess both present and future market opportunities.
Since 2009, the National Basic Public Health Services Program has been implemented, with special funds jointly allocated by the central and local governments. The program provides free basic public health services to all residents, focusing on key populations such as children, pregnant and postpartum women, the elderly, and patients with chronic diseases. Currently, the number of service items has increased from the initial 10 to 31.

National Basic Public Health Service Program. Source: Official Website of the National Health Commission; Chart by VCBeat.
In the figure above, items marked in red are newly added or have undergone significant changes from the previous version. It can be seen that with the development of China’s healthcare sector, the number of basic public health service items has increased year by year, and the coverage of key populations has gradually expanded.
For example, in the health management of the elderly in 2009, only fasting blood glucose was required to be checked once a year as part of auxiliary examinations, while more costly tests such as complete blood count, urinalysis, and B-mode ultrasound were only required to be conducted in areas with adequate resources.
In subsequent updates, auxiliary examinations were gradually expanded. The latest version includes complete blood count, urinalysis, liver function tests (serum aspartate aminotransferase, serum alanine aminotransferase, and total bilirubin), renal function tests (serum creatinine and blood urea nitrogen), fasting blood glucose, lipid profile (total cholesterol, triglycerides, low-density lipoprotein cholesterol, and high-density lipoprotein cholesterol), electrocardiogram, and abdominal ultrasound (liver, gallbladder, pancreas, and spleen). These items are required to be performed once annually nationwide.
In fact, in addition to providing basic public health services, primary care family doctors are also responsible for delivering services across three major domains: basic medical care, health management, and public health. Within the scope of basic public health services, cumbersome administrative tasks constitute a significant proportion of the workload. Moreover, funding disbursement is largely contingent upon the achievement rate of corresponding performance indicators. Consequently, primary care family doctors and institutional managers are forced to devote excessive energy to meeting these metrics, which is the primary reason behind the phenomenon of “prioritizing public health over medical care.”
Therefore, to free primary healthcare institutions and family doctors from the burdensome tasks of public health services, it is essential to identify key links and improve efficiency and speed. Upon further examination of the National Basic Public Health Service Specifications, it becomes evident that “public health physical examinations” permeate nearly all public health programs, including resident health records, population health management, and disease prevention and control. In practice, these examinations also constitute the most task-intensive, time-consuming, and laborious component.
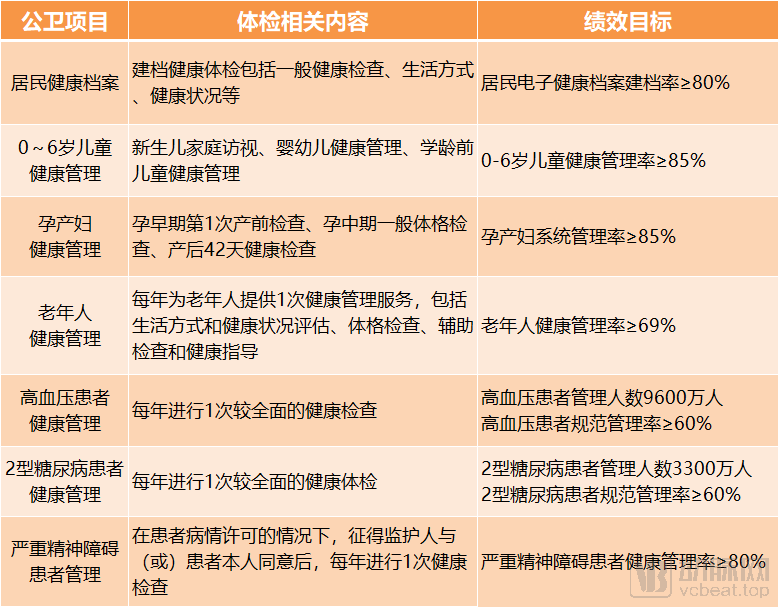
Examination-Related Content and Performance Indicators in the 2019 Basic Public Health Services Program; Source: Official Website of the National Health Commission; Graphic by VCBeat
The above outlines the physical examination components specified in the 2019 National Basic Public Health Service Guidelines issued by the National Health Commission. Health examinations for key populations, such as the elderly and patients with chronic diseases, are conducted annually, adhering to strict quantitative indicators and standardized operational procedures. Therefore, leveraging the “public health physical examination” segment through targeted service solutions to enhance efficiency, standardize management, and improve service experience will be pivotal to advancing the overall quality of basic public health services.
Although public health checkups are provided to residents free of charge, the implementation of this public welfare service has not been smooth. The main challenges include:
First, residents’ enthusiasm for participation is low. Conventional health education efforts no longer meet their needs, resulting in limited awareness of and trust in basic public health programs, with frequent instances of misunderstanding and non-compliance. Even when residents actively participate, their sense of benefit remains low if primary healthcare institutions fail to provide timely feedback on results.
Secondly, there is an abundance of forms, yet the level of informatization in primary healthcare institutions remains low. Many reports still require manual completion, aggregation, and uploading, or suffer from poor data interoperability, resulting in untimely updates of health records.
Finally, there is a shortage of personnel in basic public health services, yet the workload is heavy and the tasks are detailed. These workers must also cope with assignments or inspections arranged by superior agencies at various levels, making it difficult to balance quality and quantity in their work.
In fact, these are not only pain points in public health examinations but also reflect the broader challenges facing basic public health services. Consequently, this has led to misreporting, underreporting, and even fabrication of data, which not only damages the reputation of national public welfare programs and primary healthcare institutions but also hinders the implementation of a series of new national healthcare reform policies, such as Healthy China and tiered diagnosis and treatment.
Multiple Companies Enter Public Health Checkups or Primary Care Testing, with Significant Differences in Strategy and Approach
Currently, multiple companies have launched solutions targeting public health physical examinations or primary care laboratory testing, with varying areas of focus. Overall, the following categories can be identified:
One example of a strategic focus on the layout of internet-based healthcare systems is the WeDoctor Cloud Mobile Clinic, which constitutes a key component of WeDoctor’s four-tier digital healthcare network spanning cities, districts/counties, townships, and villages.
Another approach focuses on cold-chain logistics. Due to the stringent requirements for cold-chain transport of laboratory specimens and the dispersed nature of primary healthcare institutions, companies represented by Yunhu Yijian utilize cold-chain logistics vehicles to transport specimens, thereby linking primary healthcare facilities with third-party clinical laboratories.
Another type is the medical examination vehicle produced by traditional automakers, represented by companies such as Yutong and Dongfeng, which focuses on manufacturing craftsmanship, materials, and other hardware-related aspects of the vehicle.
Having cultivated the public health examination sector for many years, Jianjian Family Doctor positions itself as the most dedicated provider of “public health service empowerment” solutions. Covering three key areas—hardware, software, and services—it empowers primary healthcare institutions through workflow digitalization, equipment intelligence, and service standardization, thereby adopting a differentiation strategy distinct from the aforementioned products.
In terms of hardware, Jianjian Family Doctor’s flagship product, the Public Health Examination Vehicle, utilizes specialized vehicles as its platform and is equipped with 14 types of examination-related and public health education devices. It can be flexibly deployed in various out-of-hospital examination scenarios, including communities, rural areas, and nursing homes.
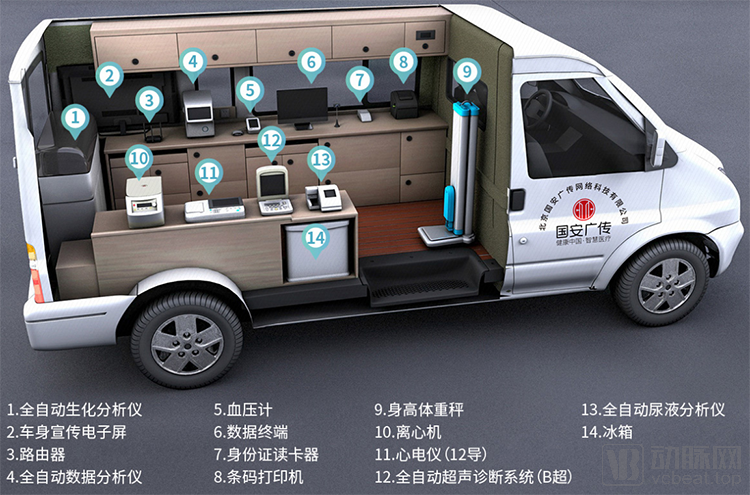
Internal Equipment of Jianjian Home Doctor Public Health Examination Vehicle
This public health examination vehicle can collect identity information and health data covering 7 major categories and 48 sub-items, including blood pressure, electrocardiogram (ECG), ultrasound, biochemistry, complete blood count (CBC), routine urinalysis, weight, and height.
On the software front, the self-developed “Jianjian Box,” “Jianjian Messenger,” and “Jianjian Data Robot,” powered by AI algorithms, big data learning, and speech recognition technologies and integrated with a health checkup management platform, not only deliver efficient and intelligent services but also significantly ensure the authenticity, validity, interoperability, and sharing of health data.
In terms of services, Jianjian Family Doctor can continue to provide outsourced operational services to primary healthcare institutions and family doctors once the software and hardware facilities are in place. It has also built a dedicated health examination operation scheduling platform that enables real-time, precise allocation of vehicles and personnel based on the needs of primary healthcare institutions. Additionally, it allows for synchronized access to residents' big health data, assisting competent authorities in real-time aggregation, analysis, and supervision.
A representative from Jianjian Family Doctor stated that, based on current operational data, a single mobile unit can serve an average of 15,000 to 20,000 patients annually.
China’s ¥42 Billion, County-Level ¥30 Million: How Does Jianjian Family Doctor Penetrate the Market?
So, how large is the public health examination market? Let’s take elderly health examinations as an example to illustrate.
According to data from the National Bureau of Statistics, in 2019, the proportion of the population aged 60 and above was 18.1%, while that of those aged 65 and above was 12.6%. Under regulations, individuals aged 65 and older are eligible for free public health examinations; however, many regions have expanded this policy to include those aged 60 and above, based on local circumstances.
Therefore, we adopt a conservative estimate that 15% of the elderly population in China participates in public health check-ups, meaning approximately 210 million people out of China’s total population of 1.4 billion are eligible. With local governments continuously increasing their support, the average subsidy for public health check-ups for the elderly has now reached over RMB 200 per person. This implies that the national market size is at least RMB 42 billion.
Public health checkup services are often procured at the level of district/county Health Commissions. Taking a district or county with a population of one million as an example, approximately 150,000 residents would be eligible for public health checkups, resulting in an annual budget of RMB 30 million.
The above figures represent only the subsidies for public health examinations among the elderly; corresponding subsidy funds are also available for other key populations, indicating that the overall market for public health examinations is even larger.
Jianjian Family Doctor Public Health Examination Services not only meet all the requirements for public health check-ups for the elderly but also cater to other key population groups. Currently, less than a year after its market launch, the public health examination vehicle has been rapidly deployed in 26 districts and counties across Hubei, Guangxi, Jiangsu, Anhui, Henan, and Jiangxi provinces. Local operational data have already demonstrated tangible results.
Taking the November 2019 report data from the Desheng Town Central Health Center in Yizhou, Guangxi as an example, the Jianjian Family Doctor Public Health Examination Program not only improved the work efficiency of local family doctors, significantly increasing the number of daily examinations and saving the labor of seven information staff members, but also reduced paper-related costs by RMB 150,000, thereby achieving genuine cost reduction and efficiency enhancement.

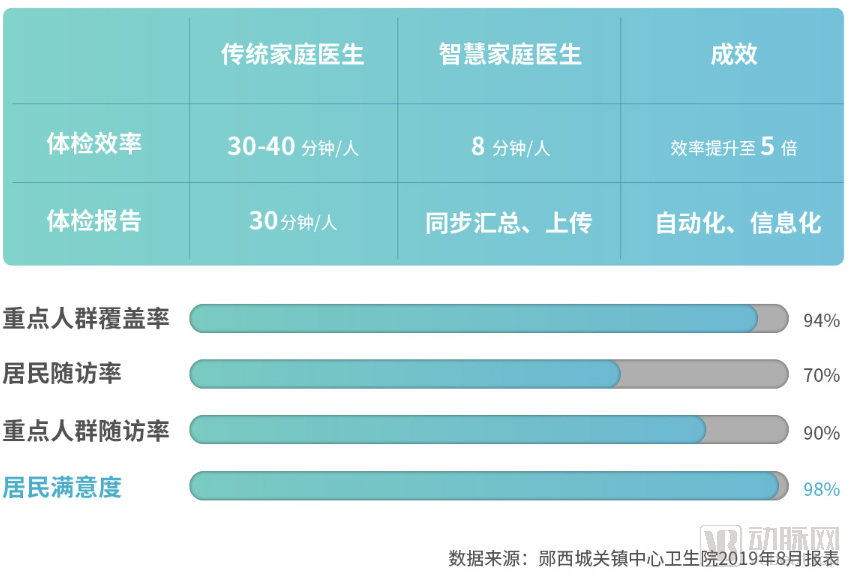
Meanwhile, the increased speed did not compromise service quality. For example, at the Chengguan Town Central Health Center in Yunxi County, Hubei Province, the implementation of Jianjian Family Doctor Public Health Examination Projects has not only significantly improved examination efficiency but also maintained high levels of coverage for key populations, resident follow-up rates, and follow-up rates for key populations, with resident satisfaction reaching as high as 98%.
Amid the economic downturn caused by the pandemic this year, Jianjian Family Doctor’s public health examination services have instead benefited from favorable momentum. Within just one month, new rounds of equipment procurement and project construction were launched in Yizhou, Guangxi, and Xinghua, Jiangsu, covering a total of 65 community health centers.
Why Has Jianjian Family Doctor Rapidly Penetrated the Market? In Summary, It Mainly Addresses Three Major Pain Points in Public Health Checkups.
First, enhance the informatization level of medical institutions to avoid redundant manual form-filling. With Jianjian Box, there is no longer a need for manual entry of either out-of-hospital checkup data or existing in-hospital checkup device data.
Second, the service radius has been expanded, with physical examinations and health education conducted simultaneously. To address issues of low resident initiative or limited mobility, public health examination vehicles can be deployed directly into communities, rural areas, nursing homes, and other locations. The electronic display screens installed on these vehicles enable simultaneous health education and promotion of basic public health services. More importantly, examination reports that comply with the "National Basic Public Health Service Specifications" can be generated on-site with a single click. This creates a more complete service loop, enhancing resident satisfaction and sense of benefit, thereby fostering greater enthusiasm for future participation.
Third, it reduces costs and improves efficiency for family doctors and primary healthcare institutions. The aforementioned cases intuitively demonstrate that the efficiency of public health examinations conducted by family doctors can be significantly enhanced.
Furthermore, due to the high mobility of vehicles, services can be rapidly launched in practice by simply integrating with local public health or resident health information platforms.
Since the launch of the National Basic Public Health Services Program, resident health records have evolved from nonexistence to existence, from paper-based to electronic formats, and from one-way data collection to gradual openness to individuals. This indicates that basic public health services have achieved phased progress. However, there is still a long way to go before resident health records are deeply integrated with medical services and health management, truly becoming a solid foundational infrastructure for national health.
Therefore, during this process, the scope of basic public health services is gradually expanding and population coverage is steadily increasing, which also means that the workload of family doctors will continue to grow.
In fact, the state has been continuously increasing fiscal investment. We have compiled the changes in the per capita subsidy standard for basic public health services since 2009:
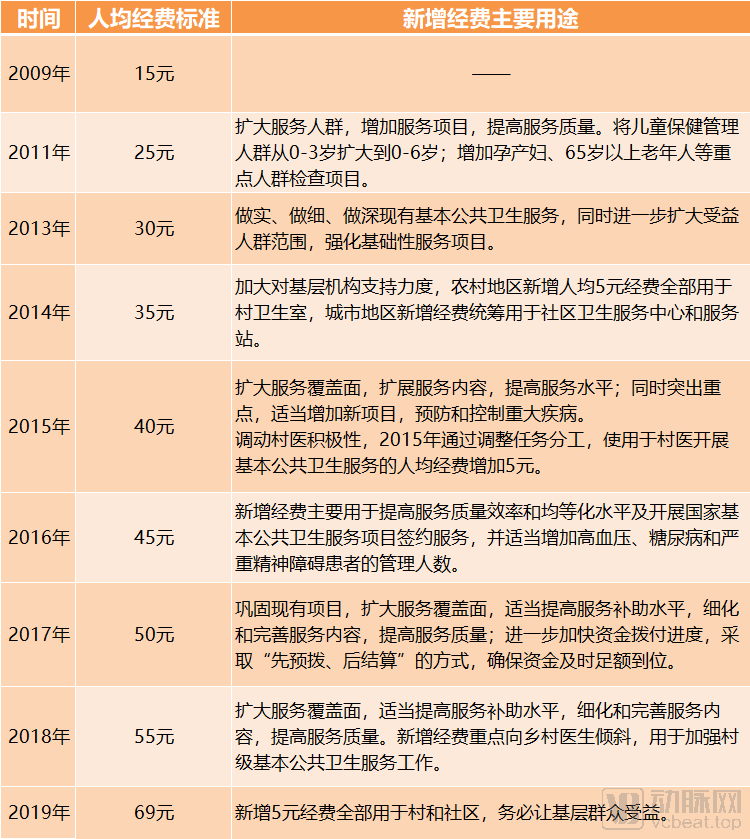
Changes in the Per Capita Subsidy Standard for Basic Public Health Services, Source: Official Website of the National Health Commission, Chart by VCBeat
As can be seen from the figure above, the per capita subsidy for public health funding has generally increased by RMB 5 annually. Of the RMB 14 increase added in 2019, RMB 5 was allocated to the original 12 basic public health services, while RMB 9 was directed toward the newly added 19 services. By 2019, based on the total population of 1.39 billion from the previous year, fiscal investment exceeded RMB 95 billion.
Adults aged 65 and older are one of the key populations for basic public health services. Data from the National Bureau of Statistics shows that between 2010 and 2019, the number of people aged 65 and above in China increased by 57.09 million, with their proportion of the total population rising from 8.9% to 12.6%. As birth rates decline, population aging is expected to intensify in the future. This trend indicates that the number of elderly individuals receiving basic public health services will continue to grow, consequently necessitating increased fiscal investment.
Furthermore, an analysis of the primary allocation of the additional costs shown in the figure above reveals that, beyond expanding coverage and enhancing service quality, resources are increasingly being directed toward community and rural settings.
The above historical data offers insights into the growth potential of the public health examination market. In the short term, 2020 is a critical year for ensuring the success of the poverty alleviation campaign, making it particularly important to strengthen the construction of public health service systems in impoverished areas. In the long term, the state will continue to optimize the structure of healthcare resource investment and enhance grassroots prevention and control capabilities in rural and community settings.
Although public health checkups constitute a highly specialized niche, they do not exist in isolation; rather, they have their own unique industry chain.

Public Health Checkup Industry Chain, Chart by VCBeat
Specifically, resources from the automotive, medical device, healthcare informatics, intelligent hardware, and telecommunications sectors can be integrated to jointly serve primary healthcare institutions.
“The expansion of basic public health service programs has increased the workload and pressure on family doctors, underscoring a stronger demand for digitalization at the primary care level,” said a representative from Jianjian Family Doctor. The representative noted that subsidies for public health services will continue to rise, with basic public health services being fully decentralized to primary healthcare institutions. “This further strengthens our confidence and determination to deepen our engagement at the grassroots level.”
The representative stated that Jianjian Family Doctor will continue to delve deeply into grassroots family doctor work scenarios, particularly addressing the practical pain points of basic public health services. Adopting a design model centered on “digitalization of workflows, intelligent devices, and standardized services,” and leveraging AI algorithms based on the TensorFlow machine learning framework and an AI speech recognition brain platform, the company aims to build a robust empowerment system for China’s National Basic Public Health Services, with public health check-ups at its core.