Policy-Driven Transformation in China's $100B+ Diabetes Management Market Amid 110 Million Patients
According to data released by the International Diabetes Federation (IDF), in 2018, China had approximately 110 million diagnosed diabetes patients, accounting for 8.2% of its total population, making it the country with the largest number of diabetes patients worldwide.
How to manage these diabetic patients has become one of the government’s key priorities for public welfare. From the perspective of policy evolution trends, diabetes management centers on increasing the rate of standardized patient care, rising from 30% in 2010 to 70% by 2025. A series of supporting policies, including health education, clinical guidance, payment mechanisms, and regulatory oversight, are implemented to support the achievement of this goal.
Specifically, what are the main content and methods of science popularization? What is the guiding direction for development? What does the specific payment system look like? And what are the key aspects of regulation?
In response, we have launched a special feature on diabetes management policies as a companion piece to the "Digital Diabetes Management Report." The full report can be accessed for free by scanning the mini-program code below.

According to statistics from the VCBeat Knowledge Base, in 2007, the former Ministry of Health issued the "Notice on Launching Publicity Activities for the 2007 'United Nations Diabetes Day'," officially ushering in the era of diabetes management. By the end of 2019, the central and provincial governments had jointly released 91 related policies.
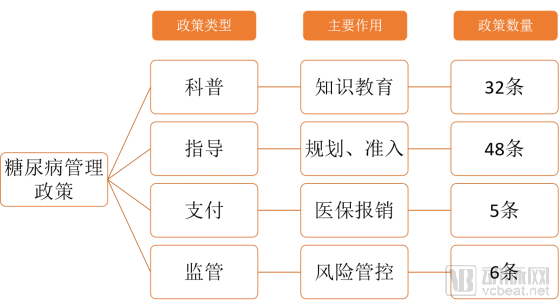
Depending on the purpose, these policies can be categorized intoFour Categories: Science Popularization, Guidance, Payment, and Regulation。
Diabetes Management: 91 Policies Across 4 Major Categories (as of the end of 2019)
Source: VCBeat
Science Popularization Policies: WithObjective of Improving Diabetes Awareness, and provide public health education. For example, the annual "United Nations Diabetes Day" awareness campaign was launched in 2007;
Guidance Policies:Public Health System Proposes Diabetes Management Goals and Overall Planning, such as the "Work Guidance Plan for Comprehensive Prevention and Control Demonstration Zones for Chronic Non-Communicable Diseases" and the "Notice on the Medium- and Long-Term Plan for the Prevention and Control of Chronic Diseases in China (2017–2025)";
Regulatory Policies: Primarily Focused on PatientsMedication Securityissued regulatory documents in this area, proposing specific regulatory measures;
Payment Policies: DiabetesOutpatient Medical Insurance Reimbursement System, such as the “Guiding Opinions of the National Healthcare Security Administration, the Ministry of Finance, the National Health Commission, and the National Medical Products Administration on Improving the Outpatient Medication Coverage Mechanism for Hypertension and Diabetes among Urban and Rural Residents.”
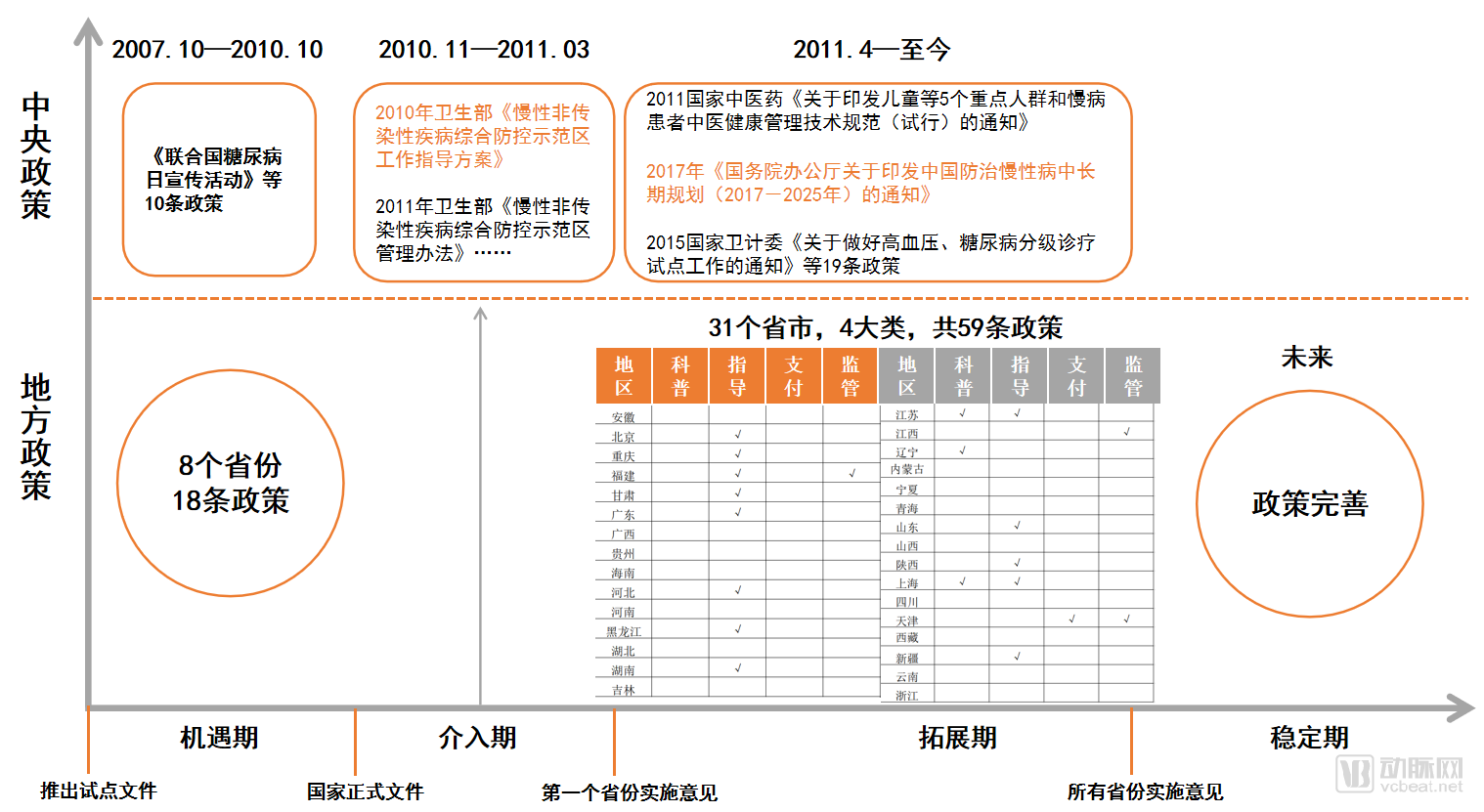
To conduct an in-depth analysis of the impact of policies on diabetes management, VCBeat Institute employs the PA model to analyze from both spatial (central to local) and temporal (developmental history) dimensions.
Level 2: From a spatial perspective, the central government first introduced top-level design policies, followed by local governments issuing detailed implementation rules. Through a cycle of development–problem identification–correction–further development, the healthy advancement of diabetes management is continuously promoted.
Four Stages: Within the policy cycle, from a corporate perspective, four distinct phases can be identified: the opportunity phase, the entry phase, the expansion phase, and the stabilization phase, each with clearly defined temporal boundaries.
Diabetes Management Policy Evolution Roadmap
 Source: VCBeat
Source: VCBeat
Window of Opportunity: Launch of Pilot Documents — As the State issues formal documents, enterprises that strategize at this juncture can seize the first-mover advantage
October 2007–October 2010: The National Health and Family Planning Commission carried out publicity campaigns for “United Nations Diabetes Day,” among other initiatives, issuing a total of 28 policies.
Intervention Phase: The central government issues official documents—the first province releases its implementation guidelines. Entering the market at this stage still offers certain opportunities.
From November 2010 to March 2011, the central government issued four official policy documents, including the “Guidance Plan for Work in Comprehensive Prevention and Control Demonstration Zones for Chronic Non-communicable Diseases.”
Expansion Phase: From the First Province Issuing Implementation Guidelines to All Provinces Issuing Implementation Guidelines—A Stage Characterized by Intense Competition
Since April 2011, following the issuance of the demonstration zone planning document by the central government, multiple provinces and municipalities have successively introduced local policies, with local governments rolling out supporting measures, totaling 59 policies.
In addition, in early 2017, the General Office of the State Council issued the "Notice on the Medium- and Long-Term Plan for the Prevention and Control of Chronic Diseases in China (2017–2025)," which further outlined development goals and pathways for the following eight years. Supporting policies, such as outpatient medical insurance reimbursement and medication coverage, have been progressively improved.
Stable Phase: Continuous regulatory policies across all provinces, with the industry entering a mature stage.
Current policies on diabetes management have not yet reached this stage.
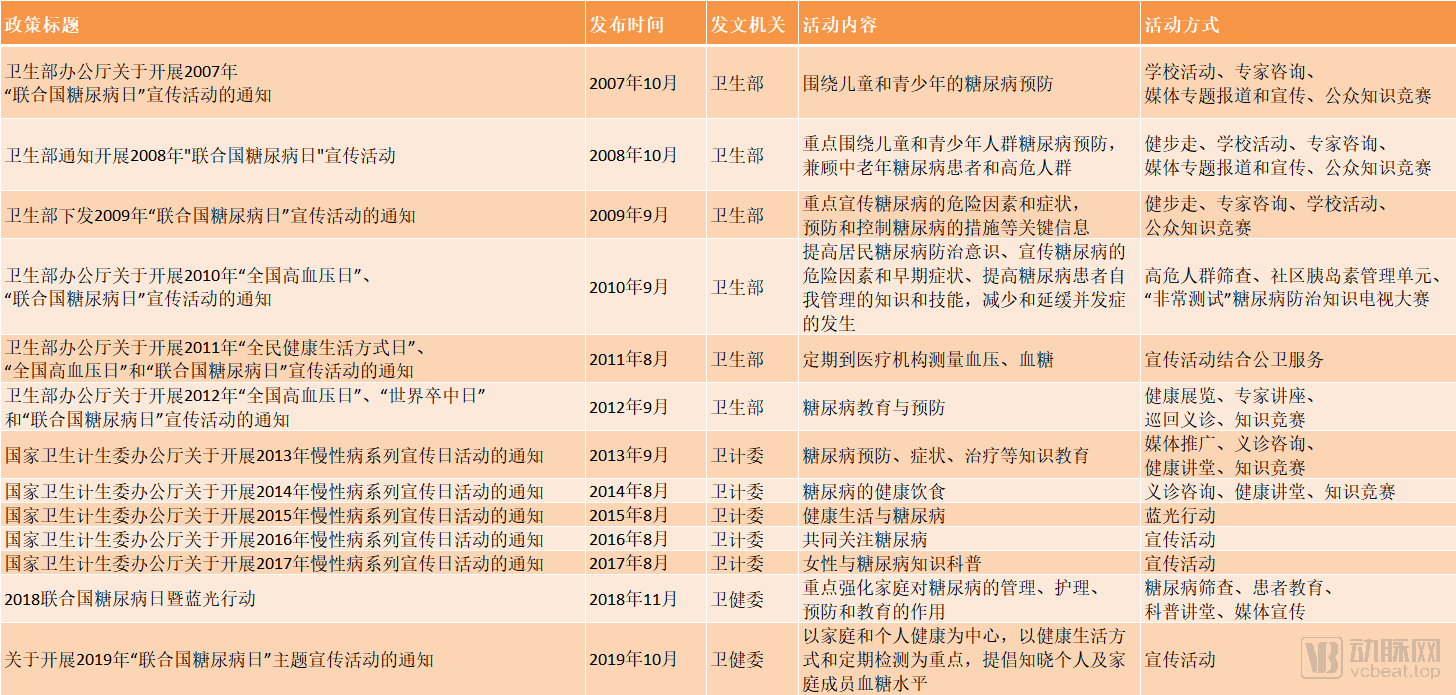
At the end of 2006, the United Nations decided that, starting in 2007, “World Diabetes Day” observed annually on November 14 would be renamed “United Nations World Diabetes Day,” and called upon all Member States, relevant United Nations organizations, other international organizations, and civil society groups to conduct awareness campaigns.
China Has Conducted “UN World Diabetes Day” Awareness Campaigns for 13 Consecutive Years
Source: VCBeat
By 2019, China had conducted public awareness campaigns for 13 consecutive years.From the perspective of target audiences, the themes and recipients of health education initiatives have evolved through five stages: children/adolescents, high-risk populations, women, all citizens, and finally families. This progression represents a shift from isolated points to linear outreach, then to broad coverage, ultimately returning to family-centered diabetes education.。
The activities primarily consist of free expert consultations, knowledge competitions, science popularization lectures, and screening for high-risk populations. In addition, the “Blue Light Action,” launched in 2010, has garnered high public participation and positive feedback, becoming a key promotional initiative that continues to this day.
The treatment of diabetes relies heavily on health education. Health education and management are critical components of diabetes care; treatment cannot be effective without proper management. Outpatient education is particularly important, yet the greatest challenge remains the difficulty patients face in changing their lifestyles.
Meanwhile, science popularization and education drive patient aggregation, creating opportunities to build management platforms that connect various stakeholders across the industry chain, including hospitals, pharmaceutical companies, and insurers. Take Zhiyun Health, a leading enterprise in diabetes management, as an example,It connects and empowers all stakeholders across the healthcare industry chain—including hospitals, patients, pharmaceutical companies, and insurers—through mobile internet and SaaS systems., helping thousands of hospitals and physicians manage and track the full lifecycle of diabetes care, and providing comprehensive solutions for disease management and daily lifestyle interventions based on big data and AI technologies, thereby achieving significant economic and social value.
In addition to patient education on the demand side, physician education on the supply side is also a critical component.
In July 2019, the Ministry of Health issued the "Notice on Launching the Early Intervention Program for Diabetes in Patients with Cardiovascular Diseases,"It is proposed to implement a three-year training program for 20,000 cardiologists across China, focusing on the diagnosis and treatment of cardiovascular disease patients with comorbid glucose metabolism disorders.To improve the diagnosis rate and early intervention rate of glucose metabolism disorders in patients with cardiovascular diseases, and to enhance the quality of life for patients with cardiovascular diseases comorbid with diabetes.
Work Plan for Early Diabetes Intervention in Patients with Cardiovascular Disease

Source: VCBeat
The window of opportunity represents the nascent stage of diabetes management and a period for market education. The former Ministry of Health, on one hand, conducted public science education for patients through initiatives such as “UN World Diabetes Day,” thereby enhancing patients’ demand for self-management; on the other hand, it provided free training for physicians and launched demonstration outpatient clinic programs to improve service capacity on the supply side, reshaping the balance between supply and demand.
In November 2010, the former Ministry of Health issued the national-level official document “Guidance Plan for the Work of Comprehensive Prevention and Control Demonstration Zones for Chronic Non-Communicable Diseases,” which for the first time set forth specific objectives for chronic disease management: to establish a number of comprehensive prevention and control demonstration zones for chronic diseases, based on district/county-level administrative divisions, across China within three to five years.
Among them, the work objectives related to diabetes include:
(1) Knowledge Awareness Rate: Population in the Demonstration AreaAwareness rate of self-monitored blood glucose levels reached 30%;
Awareness rate of core knowledge = (Number of individuals who knew they had diabetes before blood glucose measurement in the survey / Number of diabetes cases identified by epidemiological survey) × 100%.
(2) Early detection rate of chronic diseases: diabetesRegistration Rate No Less Thanlocal survey prevalence or national average prevalence of60%;
Diabetes Registration Rate = (Number of Registered Diabetes Patients / Number of Diabetes Cases Identified by Epidemiological Survey) × 100%.
(3) Chronic Disease Control Rate: Patients with DiabetesBlood Pressure,The blood glucose control rates shall be no less than 30% and 25%, respectively.。
Blood Glucose Control Rate = (Number of patients with fasting blood glucose at target during the most recent follow-up within the year / Number of managed type 2 diabetes patients within the year) × 100%.
(4) Chronic disease management rate: diabetic patientsThe standardized management rate shall be no less than 30%, respectively.;
Standardized Management Rate of Diabetes Patients = (Number of diabetes patients receiving health management in accordance with standardized requirements / Total number of diabetes patients managed within the year) × 100%.
What Is Standardized Management?The former National Health Commission has issued detailed regulations stipulating that, upon entering a medical institution within their jurisdiction, patients shall first undergo blood glucose and blood pressure monitoring and have their symptoms assessed for the period between the previous and current visits; second, receive corresponding therapeutic interventions based on the assessment results; and finally, have a relatively detailed schedule for regular follow-up visits established.
Standard for the Standardized Management of Diabetes
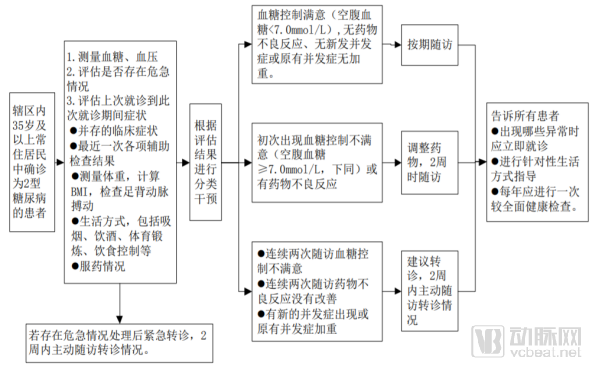
Source: National Basic Public Health Service Specifications (Third Edition)
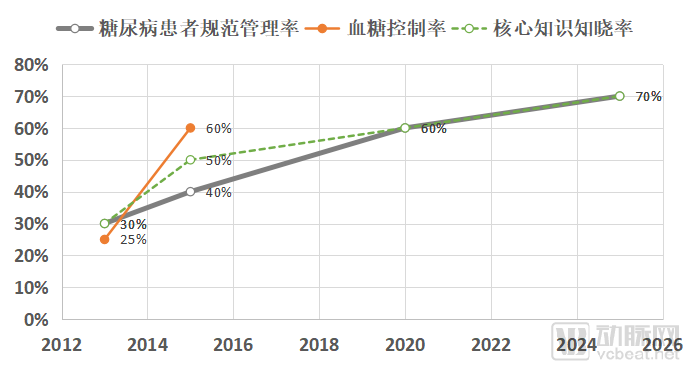
Standardized Management Rate, Blood Glucose Control Rate, and Core Knowledge Awareness Rate among Patients with DiabetesThese are three key indicators for diabetes management, repeatedly emphasized in subsequent clinical practice guidelines. The evolution of these guideline-based policies has centered on improving the rate of standardized patient management, rising from 30% in 2010 to 70% by 2025.
Objectives for Diabetes Management Proposed in the Three Major Guideline Documents
Source: Former National Health Commission, VCBeat Institute
In addition to the Work Guidance Plan for Demonstration Zones, the “China National Plan for Chronic Disease Prevention and Control (2012–2015)” issued in 2012 set targets to be achieved by 2015: a standardized management rate of 40% for patients with diabetes, a blood glucose control rate of 60%, and an awareness rate of blood glucose levels of 50%.
In 2017, the former National Health and Family Planning Commission released the latest “Medium- and Long-Term Plan for the Prevention and Control of Chronic Diseases in China (2017–2025),” which set final targets for 2025: both the standardized management rate and the core knowledge awareness rate among diabetes patients should reach 70%.
Key Indicators of the Medium- and Long-Term Plan for the Prevention and Control of Chronic Diseases in China (2017–2025)
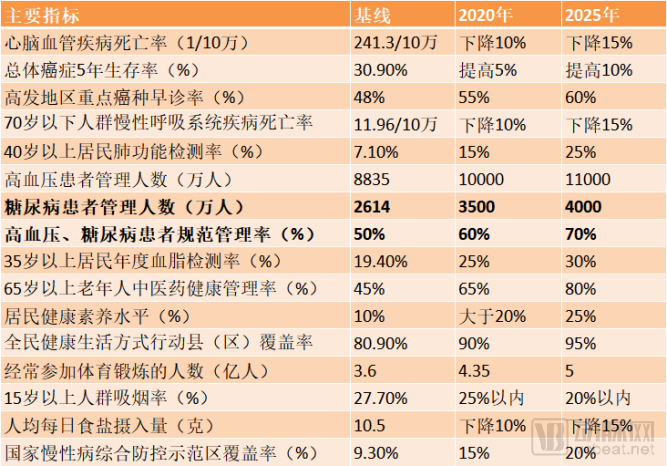
Source: General Office of the State Council, VCBeat
The large patient population and increasingly ambitious management goals are driving sustained high growth in the diabetes management market. According to data released by the International Diabetes Federation (IDF), the potential size of the overall diabetes market will reach RMB 134.9 billion in 2025.
From the perspective of the overall diabetes market structure, oral hypoglycemic agents and insulin represent two large sub-segments, accounting for 75% of the entire diabetes management market. Therefore, these two segments are currently the primary areas where digital technologies should be deeply integrated. Blood glucose smart monitoring technology is relatively mature, with a diverse range of related products. In contrast, patient willingness to pay in the personalized services market remains weak, indicating that market education will require additional time.
With the application of digital technologies across all aspects of diabetes management, digital diabetes management can cover the entire diabetes market, and the market size is promising.
>>>>
4.1 Tiered Diagnosis and Treatment System for Diabetes Management
After establishing development goals for diabetes management, the former National Health and Family Planning Commission issued the Notice on Conducting Pilot Programs for Tiered Diagnosis and Treatment of Hypertension and Diabetes in 2015, proposing tiered patient management and two-way referrals based on the functional positioning of medical institutions at different levels.
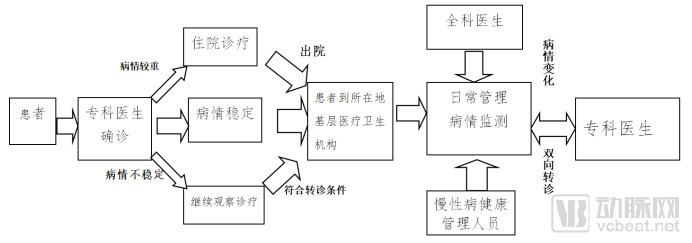
Diabetes Tiered Diagnosis and Treatment Service Process
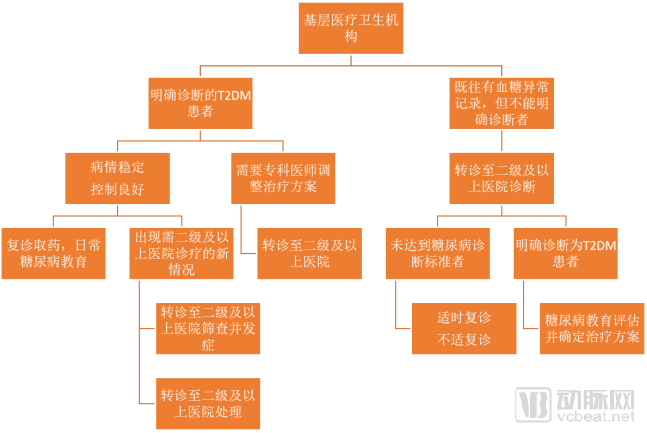
Source: "Technical Scheme for Tiered Diagnosis and Treatment Services for Diabetes," VCBeat
Primary healthcare institutions and secondary or higher-level hospitals have distinct division of responsibilities. Primary healthcare institutions are mainly responsible for the initial clinical diagnosis of diseases, formulating individualized and standardized treatment plans in accordance with disease diagnosis and treatment guidelines and norms; establishing health records and disease-specific registries, and ensuring proper information reporting; conducting routine annual physical examinations for patients, with screening for complications where feasible; carrying out patient follow-up, basic treatment, and rehabilitation services; providing health education and guiding patients in self-health management.
Hierarchical Diagnosis and Treatment Service Process in Primary Healthcare Institutions
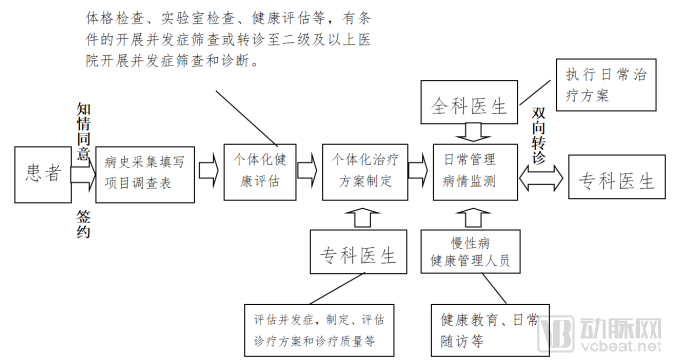
Source: Notice on Conducting Pilot Programs for Tiered Diagnosis and Treatment of Hypertension and Diabetes
Hospitals at Level II and above are primarily responsible for the clinical diagnosis of diseases, formulating individualized and standardized treatment plans in accordance with disease diagnosis and treatment guidelines and norms; conducting annual specialized physical examinations for patients, screening for complications, providing guidance, and implementing two-way referrals; and regularly evaluating the medical quality and outcomes of primary healthcare institutions. Among these, Level II hospitals are responsible for the treatment of emergency and critically ill patients, while Level III hospitals are responsible for the treatment of patients with complex, refractory, and critical conditions.
Service Process for Tiered Diagnosis and Treatment in Hospitals at Level II and Above
Source: “Notice on Doing a Good Job in the Pilot Program for Tiered Diagnosis and Treatment of Hypertension and Diabetes”
Overall,Patients with diabetes should first undergo examinations and health assessments at primary healthcare institutions. If a definitive diagnosis cannot be established, the condition is severe, or treatment adjustments by specialists are required, patients should be referred to secondary or higher-level hospitals. Once the patient’s condition stabilizes following treatment at a higher-level hospital and a detailed treatment plan has been formulated, they can be transferred back to primary healthcare institutions for routine management and disease monitoring.
In October 2017, under the guidance of the former National Health and Family Planning Commission, the Chinese Diabetes Society of the Chinese Medical Association and the Bethune Public Welfare Foundation jointly launched a national public welfare initiative titled “Action for Exploration and Evaluation of Tiered Diagnosis and Treatment Models for Diabetes in China” ((Landmark Research), aiming to evaluate the achievements of tiered diagnosis and treatment for diabetes over the past few years, and to establish a new model of three-tier (county, township, and village) primary care-based tiered diagnosis and treatment for diabetes suited to China’s national conditions.
According to the mid-year summary meeting held at the end of 2018, the study covered 864 communities/villages across 144 districts and counties in 25 provinces throughout China, enrolling nearly 20,000 patients. Patients were organized and enrolled through baseline surveys. Follow-up and referral management were conducted via a tiered diagnosis and treatment app, while patient-provider communication, health education, and blood glucose data monitoring were facilitated through a diabetes patient education and management platform app. The ultimate goal was to achieve target control of blood pressure and blood glucose levels in diabetic patients, thereby preventing the onset and progression of complications.
4.2 Digital Management of Diabetes: Evolving from Single-Disease Monitoring to an Integrated, Interconnected Platform
As the goals for standardized diabetes management continue to rise, traditional manual management approaches can no longer meet the demands, making digital management upgrades an urgent imperative. It should be emphasized thatDigital management is merely a new production tool; the ultimate goal remains unchanged.
In November 2010, the “Guidance Plan for the Work of Comprehensive Prevention and Control Demonstration Zones for Chronic Non-communicable Diseases” proposed for the first time to establish and improve a chronic disease surveillance system, so as to monitor basic content including mortality surveillance for chronic diseases, tumor registration, reporting of cardiovascular and cerebrovascular events, surveillance of risk factors for chronic diseases, and information on basic public health service programs.
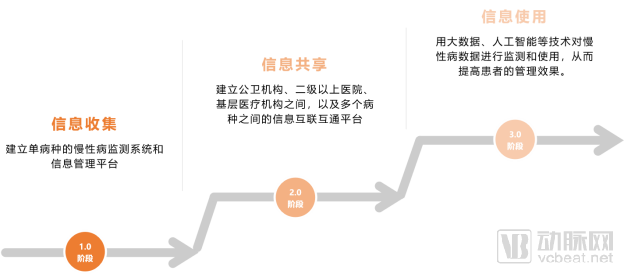
Digital Management Evolves from Single-Disease Monitoring to an Integrated Interconnected Platform

Source: VCBeat
Digital Management of Diabetes (Chronic Disease) Will Generally Go Through Three Stages, Currently in the Second Stage:
Phase 1.0: Primarily involves establishing a chronic disease surveillance system and information management platform for single diseases, with an emphasis on “Information Collection”;
Phase 2.0: Primarily focuses on establishing information interoperability among public health institutions, secondary and tertiary hospitals, and primary healthcare facilities, as well as across multiple disease categories, through regional medical and health information platforms, with an emphasis on “Information Sharing”;
Phase 3.0: Future digital management will move toward “Information Use”direction, leveraging technologies such as big data and artificial intelligence to monitor and utilize chronic disease data, thereby enhancing patient management outcomes.
Three Stages of Digital Diabetes Management
Source: VCBeat
The major trend of upgrading digital management brings certain opportunities to informatization enterprises, especially those providing data interoperability services for public health systems and hospitals.
4.3 Comprehensive Coverage of Outpatient Medication Benefits; Pilot Programs for Capitation and Diagnosis-Related Group (DRG) Payment Models
Patients with diabetes require long-term use of glucose-lowering medications, with oral hypoglycemic agents and insulin representing the two largest expenditure segments, accounting for 75% of the total diabetes market. Including outpatient medications in medical insurance reimbursement can significantly alleviate the financial burden on patients.
In October last year, the National Healthcare Security Administration and three other ministries jointly issued the "Guiding Opinions on Improving the Outpatient Medication Guarantee Mechanism for Hypertension and Diabetes among Urban and Rural Residents," which includes outpatient medications for diabetic patients participating in urban and rural resident medical insurance and undergoing drug therapy in the medical insurance reimbursement, with a payment ratio of over 50%.
Reimbursement System for Outpatient Medications for Urban and Rural Residents with Diabetes

Source: "Guiding Opinions on Improving the Outpatient Medication Guarantee Mechanism for Hypertension and Diabetes among Urban and Rural Residents," VCBeat
It should be noted that the current outpatient reimbursement system under the basic medical insurance schemeApplicable only to participants in the Urban and Rural Resident Basic Medical Insurancediabetic patients, employee basic medical insurance continues to provide the original relevant benefits, andCannot be duplicated with the special outpatient benefits for diabetes.。
Residents enrolled in the basic medical insurance scheme can only be treated atMedical Insurance-Designated Medical Institutions Below Level IIOutpatient reimbursement still requires out-of-pocket payment for services at secondary-level hospitals and above. However, prior to reimbursement, patients must first obtain a confirmed diabetes diagnosis at a secondary-level or higher hospital, have a detailed treatment plan established, and then return to primary healthcare institutions for medication.
This aligns with the tiered diagnosis and treatment system mentioned in the previous section, whereby the state leverages payment mechanisms to encourage patients with diabetes to return to primary care settings for routine management and disease monitoring.
Reimbursement for medications is limited to those included in the latest edition of the National Basic Medical Insurance Drug List.Prioritize the selection of Class A drugs, products that have passed the consistency evaluation, and those included in centralized procurement.
Search Results
Web result
Diabetes Medications (Class A) in the 2019 National Reimbursement Drug List
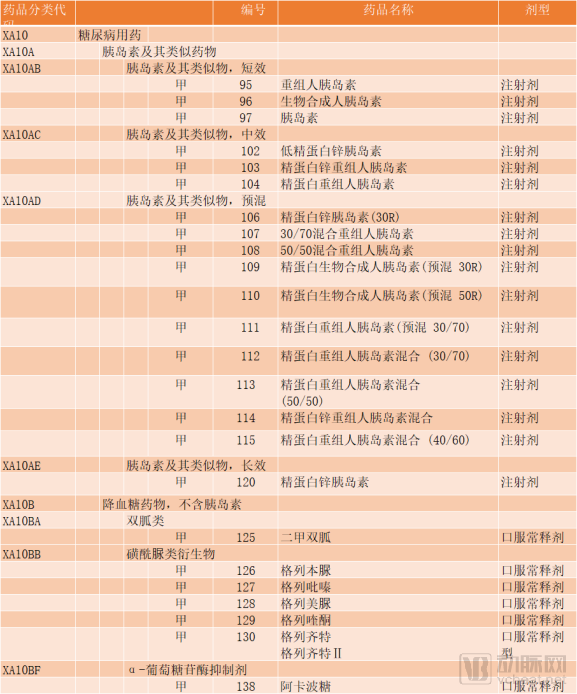
Source: National Healthcare Security Administration, VCBeat
Pharmacological therapy primarily includes sulfonylureas, biguanides, and α-glucosidase inhibitors. The Chinese Guidelines for the Prevention and Treatment of Type 2 Diabetes state that patients with type 1 diabetes require insulin therapy, while combination therapy is preferred for patients with type 2 diabetes who have failed oral hypoglycemic agents. Among these,MetforminDemonstrating favorable efficacy in glycemic control and a strong safety profile, metformin is recommended by major diabetes guidelines both domestically and internationally as the initial pharmacological therapy for patients with type 2 diabetes, regardless of whether they are overweight or have normal body weight, unless contraindicated or not tolerated. Furthermore, metformin should be included in all combination therapy regimens, underscoring its pivotal role in the management of diabetes.
In addition to the outpatient reimbursement system, the National Health Commission encourages local governments to implement capitation and diagnosis-related group (DRG) payment models based on the distribution of medical visits and medication use among insured patients with diabetes.Tianjin Is at the Forefront in Capitation Payment。
“Capitation” refers to the calculation of a reasonable payment amount based on the average cost per patient in that category. The medical insurance fund pays this predetermined amount to designated hospitals on a per-capita basis. The hospitals assume full financial responsibility under a lump-sum arrangement, where they retain any surplus but receive no additional reimbursement for any deficit.
In November 2013, Tianjin first piloted a capitation-based payment model for outpatient diabetes care at Santan Hospital in Nankai District. Under this model, the portion of medical expenses incurred by diabetic patients covered by medical insurance that is reimbursable from the medical insurance fund is settled between the medical insurance agency and designated medical insurance hospitals on a per-capita basis.For antidiabetic medication costs exceeding RMB 10,000, direct network reimbursement will continue to be implemented, eliminating the need for patients to make upfront payments.
In June 2014, the Tianjin Municipal Human Resources and Social Security Bureau issued the “Notice on Expanding the Pilot Program for Capitation-Based Payment for Outpatient Special Diseases Related to Diabetes,” extending the pilot scope to 16 primary healthcare institutions.
Service offerings break through the “three directories” restrictions:In addition to the National Reimbursement Drug List, patients can also benefit from services provided by pilot hospitals that exceed the scope of the “Three Basic Medical Insurance Catalogs” (the Catalogue of Drugs for Basic Medical Insurance, the Catalogue of Diagnostic and Therapeutic Services, and the Catalogue of Medical Service Facilities), provided that these services are filed with the Municipal Social Security Center in advance and detailed cost information is uploaded promptly.
Capitation Payment Standards:Based on the average payment levels across the city over the past three years and with reference to the reimbursement ratios of employee basic medical insurance and resident basic medical insurance, calculate the per-capita cost standards for outpatient special care for diabetes among various groups, including employees, retirees, students and children, adult residents, and elderly residents. Furthermore, determine the total annual budget for medical expenses related to the diagnosis and treatment of outpatient special care for diabetes at contracted hospitals, based on the population of enrolled patients.
In 2015, the annual per capita payment standard for urban and rural residents was RMB 1,900–5,200 (for non-medical assistance recipients) or RMB 6,300–9,100 (for medical assistance recipients); the annual payment standard for urban employees was RMB 10,800–13,100 (for non-medical assistance recipients) or RMB 15,300–15,500 (for medical assistance recipients).
Three-Party Settlement Model Involving Medical Insurance, Hospitals, and Individuals:
Capitation-Based Payment Settlement for Tianjin’s Special Outpatient Diabetes Program
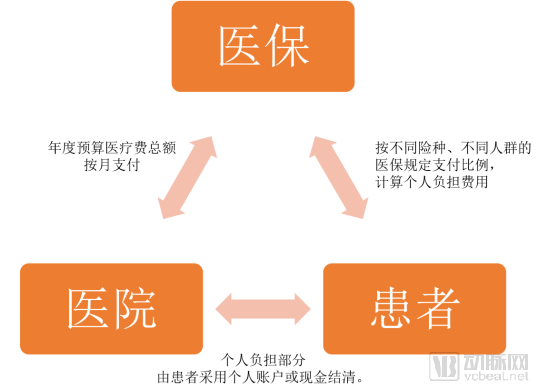
Source: Tianjin Social Security Bureau, VCBeat
Settlement between Medical Insurance Agencies and Contracted Hospitals:Based on the annual total budget for medical expenses, medical insurance agencies shall disburse monthly reimbursements for diabetes outpatient special diseases to contracted hospitals.At year-end, final accounts shall be settled in accordance with the principle of “retaining surpluses and providing no subsidies for deficits,” based on the performance of indicators such as actual workload, the out-of-pocket burden level of insured individuals, and insured individuals’ satisfaction.
**Calculation of Out-of-Pocket Expenses for Insured Individuals:** The medical insurance handling agency shall calculate the out-of-pocket medical expenses to be borne by insured individuals based on the actual medical costs incurred for the outpatient special treatment of diabetes at contracted hospitals (excluding costs for services requested voluntarily by the insured). The calculation shall adhere to the reimbursement ratios stipulated under current policies, which vary by insurance type and beneficiary category.
Settlement between Insured Individuals and Contracted Hospitals: For the special outpatient expenses for diabetes incurred by insured individuals, the portion to be borne by the individual shall be settled with the contracted hospital by the insured patient through methods such as personal account funds or cash.
Evolution of the Capitation Payment Policy for Outpatient Special Diseases of Diabetes in Tianjin
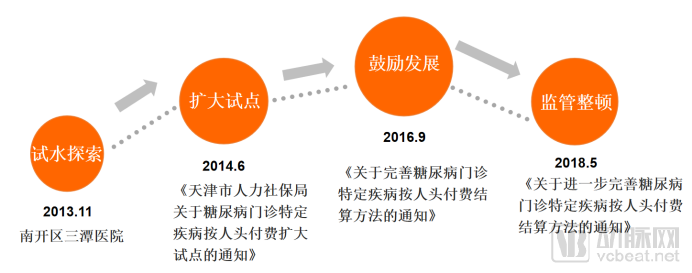
Source: Tianjin Healthcare Security Administration, VCBeat
However, the payment standards based on the total annual budget for medical expenses have faced issues with low implementation enthusiasm.In September 2016, the Tianjin Social Security Bureau issued the “Notice on Improving the Capitation-Based Payment and Settlement Method for Outpatient Treatment of Diabetes as a Specified Disease,” thereby revising the settlement approach.
The notice proposes that medical insurance will be based on hospitalsNumber of Effectively Signed-up Service Users in the Current Month and Monthly Average Per Capita Payment Standard, and settle accounts with pilot medical institutions on a monthly basis based on actual costs. Moreover, the medical insurance expenses for outpatient special care for diabetes are paid on a capitation basis.Exclusion from the annual medical insurance total budget quota management for pilot medical institutions. This further alleviates hospitals' concerns about medical insurance cost containment and enhances their proactivity in managing patients with diabetes.
Things turned to their opposite when things reached the extreme, and then various pilot medical institutions grew wildly, resulting in a sharp increase in diabetes management costs. In May 2018, Tianjin Medical Insurance Bureau issued again the "Notice on Further Improving the Capitation Payment Settlement Method for Diabetes Outpatient Specific Diseases" to standardize capitation fees and payment settlement methods.
The per-capita cost requirement shall be based on the previous year’s citywide outpatient special disease expenses for diabetes patients, with costs capped between 25% and 75%.Strengthen the supervision of settlement methods, calculated based on actual medical expenses incurred and current medical insurance reimbursement policies.The capitation fee for diabetic patients at designated service institutions shall be jointly paid by the patients and the medical insurance fund.
Among this, the patient's out-of-pocket portion is calculated based on their actual medical expenses and current medical insurance reimbursement policies, ensuring that patients' financial burden does not increase and the level of medical insurance benefits does not decrease after the reform; the difference between the patient's out-of-pocket payment and the capitation fee will be paid by the medical insurance fund according to actual costs.Does not consume the original medical insurance budget quota of designated service institutions。
To ensure patients’ reasonable healthcare needs are met and alleviate the financial burden of upfront payments, full implementation of card-swipe settlement for outpatient special disease services for diabetes has been adopted.Remove Swipe Card Settlement Limit. For those who were unable to settle payments by card in a timely manner due to unforeseen circumstances,Card swiping can be delayed.Reimbursement of medical expenses.
Insufficient patient willingness to pay is the most pressing challenge facing the diabetes management industry today. Balancing the interests of multiple stakeholders—including enterprises, medical insurance providers, hospitals, and patients—is key to the industry’s healthy development.
Future policy breakthroughs in the industry are highly likely to continue focusing on the payment side. In addition to the “Guiding Opinions on Improving the Outpatient Medication Guarantee Mechanism for Hypertension and Diabetes among Urban and Rural Residents” already issued by the National Healthcare Security Administration, the scope of covered populations and the intensity of coverage may be further expanded.
"Local governments will also successively implement the policies of the National Healthcare Security Administration to advance outpatient medication coverage for chronic diseases such as hypertension and diabetes."
In addition to traditional payment methods, China’s basic medical insurance system is also encouraging a shift toward innovative payment models such as capitation and diagnosis-related group (DRG)-based payments. Fortunately, Tianjin has been actively piloting these approaches; as experience accumulates and the models mature, they may be rolled out nationwide.
Furthermore, commercial insurance is also a potential payer. In particular, collaborating with pharmaceutical companies, internet-based chronic disease management enterprises, and mobile monitoring device manufacturers to build a vertically integrated, closed-loop service system for diabetes management is likely to become a key focus of industry development.