Impact of the Implementation of the People's Republic of China Basic Medical and Health Care Promotion Law on the Healthcare Services Industry
The Basic Healthcare and Health Promotion Law of the People’s Republic of China (hereinafter referred to as the “Healthcare Law”) was adopted at the 15th Session of the Standing Committee of the 13th National People’s Congress on December 28, 2019, and came into effect on June 1, 2020.
As the first foundational and comprehensive legislation in China’s medical and health sector, the “Healthcare Law” holds significant strategic importance for the nation as a whole. Its implementation will greatly accelerate the deepening of healthcare system reforms and foster prosperity across the entire medical and health industry.
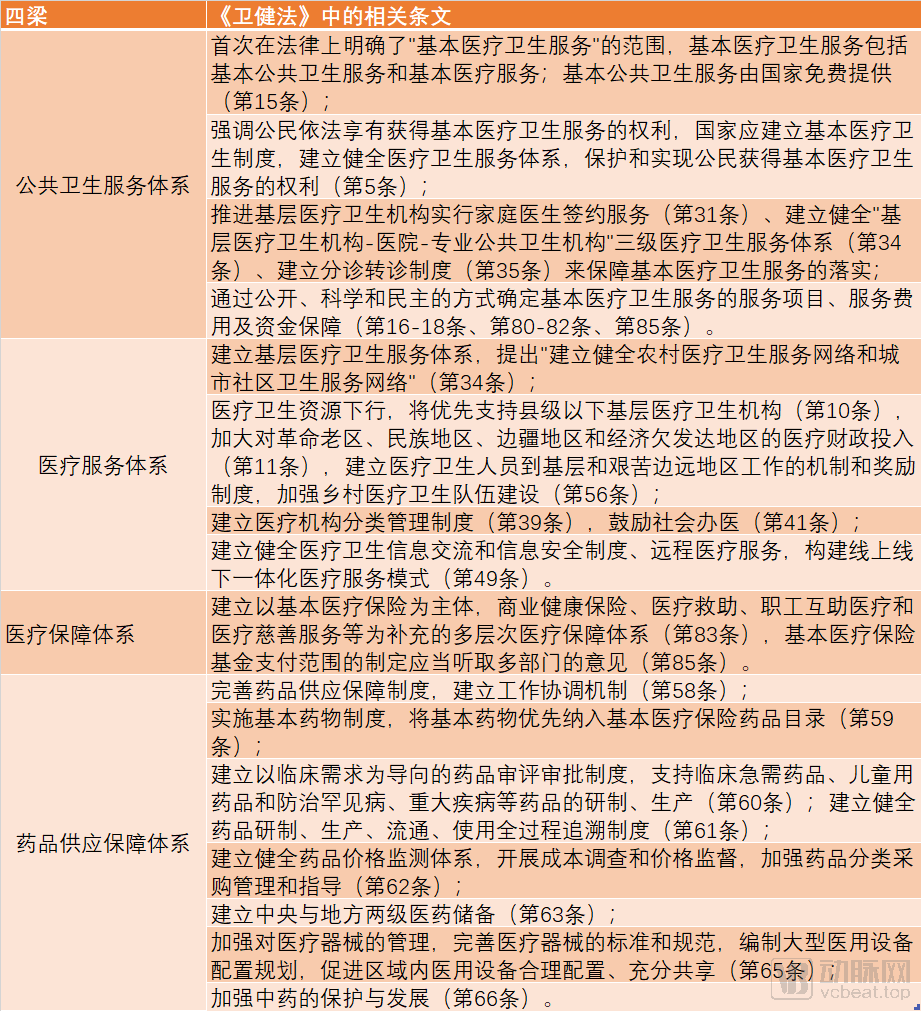
Building upon the “Opinions on Deepening the Reform of the Medical and Healthcare System” issued by the Central Committee of the Communist Party of China and the State Council in 2009, the Basic Healthcare and Health Promotion Law has established the “four pillars.”1"Eight Pillars"2 architectural legal framework; for specific details, please refer to the table below:
Note: The “Eight Pillars” are also reflected in the aforementioned provisions and will not be reiterated here.
The Healthcare Promotion Law embodies the state’s strong will to vigorously advance new types of medical services, including medical AI, family doctor contract services, medical consortia, telemedicine, and integrated elderly care with medical support. The Healthcare Promotion Law provides top-level design for the future development paths of these sectors, which will significantly propel the growth of these emerging business models. We have specifically selected two areas—family doctor services, whose market cultivation has already taken shape, and “AI + Healthcare” (hereinafter referred to as “Medical AI”)—for in-depth analysis.
1. Family Doctor Services
Family doctor services refer to an integrated service model in which family doctors sign contracts with residents, acting as "gatekeepers" of their health. These services include preventive healthcare, diagnosis and treatment of common and frequently occurring diseases, referral services, patient rehabilitation, chronic disease management, and health management. Prior to the promulgation of the Healthcare Law, the state had successively issued documents such as the Guiding Opinions on Establishing a General Practitioner System, the Work Plan for Pilot Reforms in the Practice Models and Service Delivery of General Practitioners, the Notice on Issuing the Guiding Opinions on Promoting Family Doctor Contract Services, and the Guiding Opinions on Standardizing the Management of Family Doctor Contract Services, thereby laying the groundwork for the development of family doctor services in China.
Through active exploration across various regions, the contracted service model for family doctors has become highly diversified. Taking Shanghai as an example, two major contracting models have been developed: the “1+1+1” model and the “3+X” model. (1) The “1+1+1” model allows residents, after signing a contract with a family doctor at a community health service center, to additionally select one district-level medical institution and one municipal-level medical institution for contracting, thereby forming a “1+1+1” contracting combination. This model is currently being implemented in all districts of Shanghai except Jiading District. (2) The “3+X” model is a distinctive family doctor contracting service model pioneered by Jiading District. In this model, “3” refers to one family doctor, one health manager, and one Family Doctor Service Management Center; “X” represents several support service centers. The family doctor and health manager provide front-end services to residents, while the Family Doctor Service Management Center and the various support service centers provide back-end support.
Beyond these models, a broad range of social forces have also actively participated in exploring service delivery models for family doctor services, primarily giving rise to two major approaches: (1) the offline model, where private capital directly establishes private medical institutions as a complement to public healthcare facilities, leveraging their own medical resources to provide in-person family doctor services; and (2) the online model, where private capital utilizes intelligent service platforms to offer services such as online contract signing, health management, real-time consultations, health advice, and outpatient referral appointments, exemplified by mobile applications and other products launched by internet healthcare platforms that incorporate family doctor services.
However, current family doctor services still suffer from low public recognition and the challenge of “easy enrollment but difficult fulfillment.” The primary reason is that family doctor resources in primary healthcare institutions are insufficient relative to the vast demand from patients. Furthermore, outdated information management systems and redundant medical record creation have prevented the efficient allocation of limited family doctor resources, thereby undermining the ability of enrolled family doctors to fulfill their contractual obligations. We believe that addressing these issues primarily requires leveraging social forces to empower the service capacity of primary healthcare institutions.
Article 31 of the Healthcare and Health Promotion Law stipulates that the State shall promote the implementation of family doctor contract services in primary healthcare institutions, establish family doctor service teams, sign agreements with residents, and provide basic medical and health services based on residents’ health status and medical needs. Article 29 of the Healthcare and Health Promotion Law provides that basic medical services shall be primarily delivered by government-run medical and health institutions. Socially funded medical and health institutions are encouraged to provide basic medical services.
Based on the provisions of the Healthcare Law, future mainstream family doctor services will continue to be promoted primarily by primary healthcare institutions. According to the definition in the Healthcare Law, primary healthcare institutions refer to township health centers, community health service centers (and stations), village clinics, medical offices, outpatient departments, and clinics. Due to the strong public-welfare nature of primary healthcare institutions, social capital has entered this sector with caution, resulting in few disclosed financing cases. This has led to a limited talent pool and low levels of informatization in China’s primary healthcare institutions, making it difficult for them to cope with the pressure of signing up large numbers of residents for family doctor services.
Therefore, after the implementation of the "Healthcare Law," on one hand, social capital may enter the renovation and empowerment of primary healthcare institutions on a large scale. Only by integrating emerging business models such as medical institution informatization, physician groups, telemedicine, and internet-based healthcare with family doctor services can these services be truly operationalized. On the other hand, only through the active participation of social forces in providing basic medical services, with family doctors serving as the entry point for patient flow, can residents enjoy diversified medical services without leaving their homes.
2. Medical AI
Healthcare is one of the four key priority areas for the initial application of artificial intelligence in China. Entrepreneurial activities in China’s medical AI sector are primarily concentrated in disease risk prediction, medical imaging, assisted diagnosis and treatment, drug discovery, health management, hospital administration, platforms for auxiliary medical research, and virtual assistants. During the pandemic this year, medical AI products also demonstrated outstanding performance in the prevention and control of COVID-19. Intelligent imaging analysis systems for COVID-19 were rapidly developed and deployed, assisting physicians in the screening of suspected cases and the confirmed diagnosis of COVID-19 patients.
However, our current regulatory framework for medical products is not yet fully prepared to comprehensively embrace AI-driven medical products. Taking the registration of AI-based medical products as an example, the latest Medical Device Classification Catalog classifies them as “medical software.” Depending on whether the AI product can independently provide clinical diagnostic recommendations or conclusions, it is categorized as either a Class II or Class III medical device, requiring the corresponding Class II or Class III medical device registration certificate.
On November 2, 2018, the National Medical Products Administration (NMPA) issued the Special Review Procedures for Innovative Medical Devices, providing legal support to expedite the registration process for certain medical AI products. However, medical devices applying for this expedited registration must hold invention patents for their core technologies, and their primary working principles, performance, or safety must meet the criteria of being “first-of-its-kind” and “innovative” to qualify for the special review. These high thresholds have deterred the majority of medical AI companies from pursuing this pathway.
Through the Special Review Procedure for Innovative Medical Devices, the “Coronary Flow Reserve Fraction Calculation Software” became the first to obtain Class III medical device registration in January 2020. The product took nearly two years from entering the special review procedure to final approval, indicating that the review process remained relatively lengthy.
Article 49 of the Healthcare and Health Promotion Law stipulates that the State shall promote the informatization of national health, foster the application and development of big data in health and medical care, artificial intelligence, and other technologies, accelerate the construction of information infrastructure for healthcare, establish technical standards for the collection, storage, analysis, and application of health and medical data, and leverage information technology to facilitate the widespread availability and sharing of high-quality healthcare resources. People’s governments at or above the county level and their relevant departments shall take measures to promote the application of information technology in the healthcare sector and medical education, and support the exploration and development of new models and formats of healthcare services. The State shall take measures to promote the establishment and improvement of systems for health information exchange and information security in healthcare institutions, apply information technology to develop telemedicine services, and build an integrated online-offline healthcare service model.
We believe that the implementation of the Healthcare Law will expedite the integration of medical AI products into China’s healthcare regulatory framework, for instance, by establishing a dedicated “green channel” for the registration and approval of medical AI products to accelerate their market launch. Furthermore, the formulation of unified technical standards for the collection, storage, analysis, and application of health and medical data is expected to provide a higher-quality data foundation for the research, development, and updating of medical AI products, while offering clear guidance on data compliance for medical AI enterprises.
The Healthcare Law maintains an encouraging stance toward the establishment of medical institutions by non-governmental entities, including: (1) Encouraging and guiding non-governmental entities to establish medical and health institutions, and encouraging cooperation between government-run medical and health institutions and non-governmental entities to jointly establish non-profit medical and health institutions; (2) Medical institutions established by non-governmental entities shall enjoy equal treatment with public medical institutions in terms of qualification assessment and rights (such as designation for basic medical insurance, development of key specialties, scientific research and teaching, grade evaluation, access to specific medical technologies, and professional title evaluation of medical and health personnel); (3) Non-profit medical and health institutions established by non-governmental entities shall enjoy the same policies as public medical institutions regarding the application of fiscal preferential policies and public utility services (such as taxation, fiscal subsidies, land use, water supply, electricity supply, gas supply, and heating supply).
Following the further deregulation of privately-run healthcare, and in order to prevent excessive inflow of private capital into the healthcare sector—which could lead to the de facto commercialization of high-quality medical resources within public and non-profit medical institutions, thereby undermining public interests—the Healthcare Promotion Law has introduced certain institutional designs, including:
1.Social Capital Must Adhere to the “Two Prohibitions” When Cooperating with Public Medical Institutions in Joint Healthcare Ventures
The Healthcare Law emphasizes the “public welfare” nature of medical and health institutions established by the government, clearly stipulating that medical and health institutions established or participated in (including through cooperation with social capital) using government funds or donated assets shall not be established as for-profit medical and health institutions. Meanwhile, the Healthcare Law also provides that medical and health institutions established by the government shall not invest jointly with other organizations to establish medical and health institutions without independent legal person status.
In previous practices of social capital participation in healthcare, private investors have pioneered numerous operational models for establishing medical and health institutions in collaboration with government-run medical facilities, including (1) the “One Site, Two Hospitals” model3, such as the collaboration between Fuxing Hospital of Capital Medical University and Beijing Fuxing Bo'ai Eye Center; (2) establishing new campuses or branches of government-run public hospitals through cooperation or joint ventures; (3) directly establishing for-profit medical institutions through joint ventures with social capital, such as Beijing New Century Children's Hospital, jointly established by Beijing Children's Hospital of Capital Medical University and New Century Healthcare. Following the implementation of the Healthcare Promotion Law, the aforementioned cooperation models may require adjustments.
2.Non-profit healthcare institutions are prohibited from distributing dividends or engaging in disguised dividend distributions.
Prior to the enactment of the Healthcare Promotion Law, China’s policies regarding whether non-profit medical institutions could distribute surpluses underwent a shift from comprehensive tightening to slight relaxation. Both the Implementation Opinions on the Classified Management of Urban Medical Institutions, formulated by four ministries and commissions including the former Ministry of Health and the Ministry of Finance and effective as of September 1, 2000, and the Opinions on Further Encouraging and Guiding Social Capital to Establish Medical Institutions, formulated by five ministries and commissions including the former Ministry of Health and the National Development and Reform Commission and effective as of November 26, 2010, explicitly stipulated that the revenue generated by non-profit medical institutions, after deducting prescribed reasonable expenditures, could only be used for the continued development of the medical institutions.
On June 11, 2015, the General Office of the State Council issued and implemented the “Several Policy Measures on Promoting the Accelerated Development of Socially-Run Medical Institutions,” which encourages local authorities to explore the establishment of incentive mechanisms for sponsors of private non-profit medical institutions, with some provinces4To encourage private non-profit medical institutions, breakthrough innovations have also been implemented. For non-profit medical institutions established with social capital, after deducting operational costs, setting aside development funds, and allocating other necessary expenses in accordance with relevant national regulations, the organizers are permitted to obtain reasonable returns from the surplus or to allocate a certain percentage of the surplus as rewards for the organizers.
During the policy exploration phase, social capital typically achieves profit transfer from non-profit medical institutions through the following two models: (1) IOT (Invest-Operate-Transfer) model5(such as the collaborations between China Resources Healthcare and non-profit medical institutions including Beijing Yanhua Hospital Group and Beijing Jingmei Group General Hospital); and (2) the service agreement model (such as the collaborations between Honghe Renai Medical and Yangsi Hospital and Jinhua Hospital).
The Healthcare Law reiterates that non-profit medical institutions are prohibited from distributing or indirectly distributing profits to investors or sponsors, and establishes corresponding penalties, thereby reaffirming a prudent and stringent regulatory stance on the issue of surplus distribution by non-profit medical institutions. In this context, the practice of social capital obtaining management fees or service fees under the aforementioned IOT model and service agreement models carries a certain risk of being deemed as disguised dividend distributions.
We believe that the restrictive provisions in the Healthcare Promotion Law regarding cooperation between social capital and public medical institutions, as well as profit distribution from non-profit medical institutions, continue to uphold the principle of public welfare inherent to public and non-profit medical institutions. However, how to resolve the inconsistencies between current private healthcare practices and the Healthcare Promotion Law remains to be further clarified by subsequent supporting policies or practical guidelines.
The promulgation of the Health Care Law has filled the gap in China’s foundational and comprehensive legislation in the health sector, establishing a framework for the steady advancement of medical reform. While affirming the public-welfare nature of healthcare services, the law also supports and encourages social forces to participate in the healthcare sector, while simultaneously strengthening regulatory oversight over privately run medical institutions. We anticipate the final implementation of the detailed rules for the Health Care Law and will closely monitor the significant impact this will have on the entire industry.
[1] The “Four Pillars” refer to the public health service system, medical service system, medical security system, and pharmaceutical supply guarantee system.
[2] The “Eight Pillars” refer to a coordinated and unified healthcare administration system, an efficient and standardized operational mechanism for healthcare institutions, a scientific and rational drug pricing mechanism, a government-led diversified healthcare financing mechanism, a strict and effective healthcare regulatory system, sustainable mechanisms for healthcare technological innovation and talent support, a practical and shared healthcare information system, and a sound legal framework for healthcare.
[3] The “One Site, Two Hospitals” model refers to a public government hospital partnering with social capital by leveraging part of its existing assets to establish a for-profit hospital at the same location as the original public hospital, resulting in a model where both non-profit and for-profit hospitals coexist within the same campus.
[4] These provinces specifically include Jiangsu, Yunnan, Jiangxi, Changsha, Henan, Fujian, Anhui, and Liaoning.
[5] The IOT (Invest-Operate-Transfer) model refers to a arrangement in which private capital provides investment to medical institutions in exchange for the right to operate such institutions and collect management fees for a specified period.
Authors: AnJie Broad’s Healthcare Team
Contact QR Code


Introduction to Attorney Cai Hang: For over a decade, he has specialized in investment and financing services within the healthcare, TMT, and artificial intelligence sectors, wielding significant influence in China’s venture capital legal services landscape. *China Business Law Journal* named him one of the “Top 100 Legal Elite in China,” recognizing him as one of the country’s most outstanding commercial lawyers. He has also been repeatedly recommended by leading legal ranking agencies such as The Legal 500 and Legalband in the fields of TMT and venture capital. In addition to venture capital practice, he is highly proficient in mergers and acquisitions and capital markets. Mr. Cai is the Managing Partner of AnJie Broader Law Firm’s Shanghai office.

Introduction to Attorney Wang Fei: Represented renowned domestic and international funds in completing a substantial number of investment and M&A transactions, while also providing legal services for corporate clients’ financing and investment activities. The industries involved primarily include healthcare, entertainment and media, enterprise digital services, fresh food e-commerce, and new retail. In the area of compliance within the healthcare and wellness sector, Attorney Wang Fei assisted healthcare industry funds in deeply engaging in compliance matters for community healthcare groups and represented clients in completing investments and acquisitions of multiple medical institutions and internet healthcare companies.

Introduction to Wu Yao: She primarily specializes in private equity investment and financing, mergers and acquisitions, restructuring, and compliance. She has represented numerous renowned USD-denominated and dual-currency funds, as well as industry-leading enterprises, in completing multiple domestic and cross-border private equity investment legal services. The industries involved include online and offline healthcare, enterprise management, and new retail. Additionally, she has provided legal services for financing activities of high-quality enterprises in sectors such as electronic product recycling, big data service and analytics platforms, and social networking software.