National Healthcare Security Administration Releases CHS-DRG Subgrouping Scheme: How Hospitals Can Adopt Lean Operations to Navigate Payment Reform
On June 18, the Notice of the General Office of the National Healthcare Security Administration on Issuing the Subgrouping Scheme for China Healthcare Security Diagnosis-Related Groups (CHS-DRG) (Version 1.0) (No. 29 [2020] of the General Office of the NHSA) (hereinafter referred to as the “Notice”) was released by the News Center of the National Healthcare Security Administration. The Notice requires all pilot cities to formulate local DRG subgroups with reference to the CHS-DRG subgroups, or to directly adopt the CHS-DRG subgroups for carrying out national pilot work on local DRG-based payment.
The “Notice” also requires that the 30 pilot cities submit their evaluation reports to the National Technical Guidance Group for DRG Payment Pilots by August 31, and commence simulation operations upon approval. This signifies that the long-discussed DRG payment pilots are about to officially enter the implementation phase.
Based on the experiences of other countries and regions, DRG-based payment will completely disrupt hospitals’ previous revenue strategies, forcing those unable to proactively adapt to the system to exit the market. After the implementation of DRG payment in the United States, 454 hospitals closed and 22,000 emergency beds were shut down between 1987 and 1994.
So, how should healthcare institutions respond to the impending “storm” of payment system reform, and what role will information technology restructuring play in this process? Industry experts have offered diverse perspectives, and VCBeat (WeChat ID: Vcbeat) has compiled and updated recent relevant materials.
Diagnosis Related Groups (DRG) is a case-mix classification scheme, i.e., a system that categorizes patients into several diagnostic groups for management purposes based on factors such as age, disease diagnosis, comorbidities, complications, treatment methods, severity of illness, outcomes, and resource utilization.
DRG was first proposed in 1967 by Robert B. Fetter of the Yale School of Management and John Thompson of the Yale School of Public Health. It is an internationally recognized standardized tool for grouping healthcare services, applicable to medical quality management, performance evaluation, cost control, payment, and budget management. Currently, nearly 40 countries and regions worldwide have adopted DRG. Notably, advanced countries such as the United States and Germany began implementing DRG as early as the 1980s, accumulating extensive experience.
DRGs were originally developed as a tool for healthcare quality management, aiming to assist clinicians and hospitals in monitoring service quality and utilization. By grouping cases based on principles of clinical homogeneity and similar resource consumption, and assigning weight values to quantify them, DRGs enable direct comparison of performance among different service providers, thereby facilitating a scientific and accurate evaluation of the clinical performance of hospitals, clinical departments, and physicians.
DRG-based evaluation of medical capability is primarily achieved through two indicators: the number of DRG groups covered by the hospital and the Case Mix Index (CMI). These two indicators represent the breadth and depth, respectively, of a hospital’s medical service capabilities.
The number of DRG groups covered can measure a hospital’s comprehensive service capability; the greater the coverage, the more comprehensive the hospital’s technical capabilities. For instance, if the obstetrics and gynecology department has 10 DRG groups and a hospital was able to capture all 10 groups over the past year, this indicates that the hospital’s obstetrics and gynecology services are highly comprehensive. By the same token, if Hospital A covers more than 400 DRG groups while Hospital B covers only slightly over 200, this suggests that Hospital B’s comprehensive medical service capability is inferior to that of Hospital A.
CMI is used to measure the overall technical complexity of medical services; a higher value indicates greater complexity and corresponds to a higher level of technical proficiency at the hospital. The calculation of CMI is straightforward: it is the ratio of the average cost of cases within a specific diagnosis-related group to the average hospitalization cost for all diseases in the local area.
Assume a region has 3 million discharged cases per year, with an average hospitalization cost of RMB 15,000, which represents the average hospitalization cost for all diseases in the area. The average cost for the DRG group covering vaginal delivery is RMB 6,900; the ratio of this amount to RMB 15,000 yields the CMI for the vaginal delivery group, i.e., 0.46. The cost for the DRG group covering coronary artery bypass grafting (CABG) is RMB 30,000, so its CMI should be 2. Clearly, compared with vaginal delivery, CABG involves a much higher level of technical complexity.
Thus, assuming that the average case-mix index across all departments at Hospital A is 1.5 under an equivalent volume of cases, compared to only 0.7 at Hospital B, this indicates that Hospital A has a higher level of technical expertise and greater capability in managing complex and refractory conditions.
In the late 1970s, the United States pioneered pilot programs for Diagnosis-Related Group (DRG)-based payment. Following their success, this model was rolled out nationwide. Therefore, in addition to performance evaluation, DRGs can also be used for payment purposes, specifically under the Diagnosis-Related Group Prospective Payment System (hereinafter referred to as DRG-PPS).
DRG-PPS is a payment method that establishes payment standards for each Diagnosis-Related Group (DRG) to reimburse medical expenses. Under the DRG-PPS system, each case is assigned to a specific DRG group based on differences in diagnosis, treatment modalities, and patient characteristics. Payers then provide bundled payments according to the payment standards associated with the DRG group to which the case is assigned.
DRG-PPS controls expenditures by establishing prospective payment standards and leverages bundled payments to compel healthcare institutions to share financial risks, thereby effectively reducing the likelihood of hospitals profiting from overutilization of medical services and achieving control over healthcare costs. Surveys indicate that following the implementation of DRG-PPS in the United States, the growth rate of healthcare expenditures decreased from 16%–18% prior to 1983 to 7%–8%, and the short-term hospitalization rate declined by 12% within one year.
Under the pressure of the DRG-PPS, healthcare institutions are compelled to proactively standardize the clinical practices of medical personnel, enhance cost awareness, utilize medical resources rationally, and improve service quality and operational efficiency. Since the DRG-PPS balances the interests of multiple stakeholders—including the government, hospitals, and patients—while achieving a reasonable equilibrium between healthcare quality and costs, most countries and regions that have introduced DRG have consistently adopted it for payment purposes.

Image sourced from conference materials, used with authorization from the rights holder.
Compared with fee-for-service and per-diem/per-capita payment models, DRG-PPS indeed offers unique advantages in cost containment.
Single-disease payment and DRG-PPS, while somewhat similar, differ fundamentally in their grouping principles. Single-disease payment does not account for comorbidities or complications and groups cases based on a single disease entity. In contrast, DRG-PPS comprehensively considers comorbidities, complications, and other patient-specific factors, assigning cases into multiple diagnosis-related groups.
Therefore, single-disease payment lacks flexibility in practical application and does not align with real-world conditions. Hospitals can circumvent this system by excluding cases that consume more resources from the single-disease payment framework. For this reason, the DRG-PPS, which accounts for comorbidities, complications, and other patient-specific factors, offers greater operability and scientific rigor compared to single-disease payment.
Of course, the DRG-PPS is not a panacea; it has its own limitations. The DRG-PPS is only suitable for cases where diagnosis and treatment methods significantly impact resource consumption and treatment outcomes, such as acute inpatient cases. It does not leverage the advantages of DRG-PPS for outpatient cases, rehabilitation cases, cases requiring long-term hospitalization, or cases within the same disease group that exhibit significant variations in resource utilization and treatment efficacy (such as mental disorders).
China initiated research on DRG-PPS at an early stage. As early as the late 1980s, the Beijing Institute of Hospital Management (later the Information Center of the Beijing Municipal Health Commission) began conducting DRG research. In 2008, by integrating American and Australian DRG versions, China developed its first domestic DRG grouping scheme, BJ-DRG.
In 2011, Beijing launched a pilot program for DRG-PPS in six Grade A tertiary hospitals, selecting 108 DRG groups, thereby accumulating valuable experience and lessons for the subsequent implementation of DRG-PPS.
With the surge in China’s healthcare expenditures in recent years, which has placed enormous pressure on the medical insurance system, the implementation of DRG-PPS as an effective cost-containment measure has become imperative. From 2011 to 2015, China’s total health expenditure rose rapidly from RMB 2.43 trillion to RMB 4.09 trillion, with its share of GDP increasing from 5.03% to 6.0%.
In the "Statistical Bulletin on the Development of China's Health and Hygiene Undertakings in 2019," recently released by the National Health Commission, the total national health expenditure in 2019 is estimated to have reached RMB 6.52 trillion, accounting for 6.6% of GDP.
Moreover, in 2018, the growth rate of medical insurance expenditures exceeded that of revenues for the first time—if this trend continues, medical insurance funds will eventually face a deficit.
Therefore, on June 28, 2017, the General Office of the State Council issued the “Guiding Opinions on Further Deepening the Reform of Basic Medical Insurance Payment Methods” (Guo Ban Fa [2017] No. 55) (hereinafter referred to as the “Opinions”). The “Opinions” required the gradual promotion and implementation of DRG payment pilots. This is regarded as the beginning of the large-scale advancement of DRG payment in China.
To improve the unified basic medical insurance system for urban and rural residents and the critical illness insurance system, continuously enhance the level of medical security, ensure the rational use and safe control of medical insurance funds, and coordinate the “three-medical linkage” reform of healthcare services, medical insurance, and pharmaceuticals to better guarantee access to medical care, the National Healthcare Security Administration, which bears the significant responsibility of controlling medical insurance costs, was officially established on May 31, 2018.
Subsequently, the National Healthcare Security Administration proposed a master plan for a three-year pilot of the DRG-PPS. The plan stipulated completing the top-level design and formulating grouping schemes in 2019; conducting simulated operations in 30 pilot cities in 2020; and officially implementing the DRG-PPS nationwide in 2021.
In June 2019, the National Healthcare Security Administration, in conjunction with the Ministry of Finance, the National Health Commission, and the National Administration of Traditional Chinese Medicine, jointly launched the national pilot program for Diagnosis-Related Group (DRG) payment in 30 pilot cities. These 30 cities were to implement DRG-based payments in 2020, summarizing lessons learned and best practices from the implementation process to ensure the nationwide rollout of DRG payment across China in 2021.
In 2019, the National Healthcare Security Administration also organized the development of the Technical Specifications for Diagnosis-Related Group (DRG) Classification and Payment under the National Healthcare Security System (hereinafter referred to as the “Technical Specifications”) and the National Healthcare Security DRG (CHS-DRG) Classification Scheme (hereinafter referred to as the “Classification Scheme”). On October 16, it issued the Notice on Printing and Distributing the National Pilot Technical Specifications and Classification Scheme for Diagnosis-Related Group (DRG) Payment (Yi Bao Ban Fa [2019] No. 36).
The “Technical Specifications” and the “Grouping Scheme” constitute the fundamental framework for China’s Healthcare Security DRG (CHS-DRG). They establish that CHS-DRG, which integrates the BJ-DRG, CR-DRG, and CN-DRG versions, is the sole standard for implementing DRG-PPS by healthcare security authorities across China. The documents require all pilot cities to strictly adhere to the CHS-DRG standard and carry out pilot work in accordance with the unified deployment of the National Healthcare Security Administration.
On June 18, 2020, the National Healthcare Security Administration issued a Notice that further subdivided the 376 core groups into 618 groups to serve as the basic units for DRG-based payment. The Notice also required pilot cities to develop local DRG subgroups by referencing the CHS-DRG subgrouping results, the comorbidity/complication and severe comorbidity/complication lists, grouping rules, and naming conventions; alternatively, they could directly adopt the CHS-DRG subgroups to carry out national pilot work on local DRG-based payment.
At this point, DRG-PPS is about to be officially piloted in China.
So, what conditions and key technologies must DRG-PPS meet? The Technical Specifications provide a detailed explanation of this.
Image sourced from conference materials, used with authorization from the rights holder
According to the "Technical Specifications," implementing DRG-PPS must meet four conditions: unified disease diagnosis coding and surgical procedure coding must be ensured within the region. Medical institutions must have medical record quality that meets standards and possess relatively standardized diagnosis and treatment processes. Health insurance agencies and medical institutions must have secure and stable hardware platforms and network services, as well as the capability to develop data interaction with DRG grouping. There must be a competent team for health insurance administration, management, supervision, and assessment locally, maintaining close cooperation with hospitals in the region.
After meeting the basic prerequisites, the DRG-PPS requires the implementation of several key technologies to achieve its intended effectiveness. These key technologies include data collection and quality control, DRG grouping and weight setting, payment standard calculation and settlement, and regulatory assessment and evaluation systems.
Data collection and quality control must adhere to standardized acquisition principles. Both historical data collected prior to the implementation of DRG-PPS and data collected thereafter must comply with DRG data collection standards and quality assessment frameworks. The processes of data acquisition and quality review should be standardized, normalized, and intelligentized to ensure data integrity, rationality, and compliance.
DRG Grouping and Weight Setting Must Adhere to Several Principles: Cases Should Be Grouped Based on Similar Clinical Processes (Including Disease Diagnosis, Surgery, or Procedures) and Comparable Resource Utilization; Integration of Clinical Data with Data Validation; and Balancing the Administrative Requirements of Health Insurance Payment with the Practical Needs of Healthcare Services.
The calculation of payment standards must adhere to several overarching principles: First, regional global budgets should be taken into account. Second, while upholding the principle of equal pricing for the same disease at hospitals of the same tier, differences in service capabilities among medical institutions must be considered, and reasonable room for growth in medical expenses should be provided. Finally, the standards must undergo multi-perspective validation before implementation, thereby ensuring a win-win outcome for hospitals, health insurance funds, and patients.
In the settlement component of payment standards, local healthcare security administrations are required to specify in their DRG settlement detailed rules or measures how DRG-PPS payments are calculated and disbursed to contracted hospitals. By formulating these detailed settlement rules, healthcare security administrations can provide comprehensive provisions on matters such as the scope of DRG-PPS application, coding methodologies, settlement approaches for special cases, and the methods for fund settlement and disbursement.
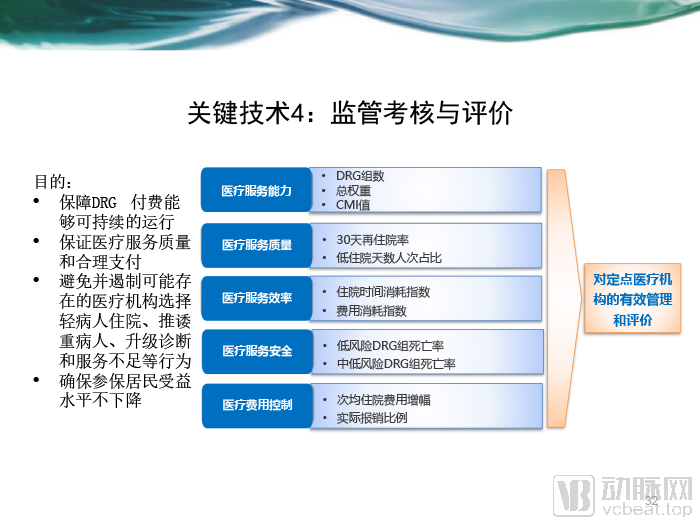
Image sourced from conference materials, used with authorization from the rights holder
The primary objectives of regulatory assessment and evaluation are to ensure the quality of medical services and appropriate reimbursement, while preventing and curbing potential misconduct by healthcare institutions—such as cherry-picking low-risk patients, shirking responsibility for critically ill patients, upcoding, and under-provision of services. These measures aim to safeguard the sustainable operation of the DRG-PPS system and ensure that the benefit levels for insured residents do not decline. The design of DRG-PPS regulatory assessments must balance effective control of medical expenditures with the maintenance of healthcare service capacity, quality, efficiency, and safety.
From the definition, characteristics, and key technologies of DRG-PPS, it is evident that DRG-PPS will significantly alter the revenue structure of healthcare institutions and exert a profound impact on the medical industry. Under the previous fee-for-service model, hospitals generated revenue from every item provided—whether diagnostic tests, pharmaceuticals, or medical consumables—with higher volumes of services directly translating into greater hospital income.
Under the DRG-PPS framework, health insurance payments are made as bundled amounts based on diagnosis-related group classification. Consequently, examinations, pharmaceuticals, and medical consumables, which were previously revenue sources, have all become costs. Hospitals must minimize these costs as much as possible while ensuring medical quality to achieve a surplus; otherwise, they will incur losses. Chen Xianli, Vice President of Beijing Dongruan Wanghai Technology Co., Ltd., believes that the implementation of DRG-PPS will significantly impact the medical service revenues of many hospitals.
To illustrate, consider Public Hospital A, a Grade 3A tertiary public hospital with an annual revenue of approximately RMB 3.8 billion. Its surplus from medical service operations accounts for only 0.76% of the hospital’s total, yet inpatient revenue constitutes as high as 81% of its income, significantly exceeding the average inpatient revenue proportion of around 60% typically seen in Grade 3A hospitals.
The hospital’s average cost per inpatient stay exceeds RMB 21,000. DRG-based payment has the greatest impact on the hospital’s inpatient revenue. Based on the experience of Hospital B, which is comparable in scale and located in a region where DRG-PPS has already been piloted, its average cost per inpatient stay decreased from RMB 19,000 before DRG-PPS implementation to RMB 15,000 afterward. Therefore, Hospital A is expected to see a substantial decline in its average cost per inpatient stay after implementing DRG-PPS. Using this reduction as a benchmark, the hospital’s overall revenue would be affected by 10% to 20%. Chen Xianli stated that this would directly threaten the hospital’s viability.
In fact, China has been striving to improve this situation through its healthcare reforms over the years and has achieved some results.
According to the National Health Commission’s Statistical Yearbooks from previous years, in 2014, drug revenue accounted for the largest proportion of public hospital income in China, reaching as high as 42.2%; meanwhile, service revenue—excluding income from drugs, consumables, and diagnostic tests—accounted for only 32.7% that year. By 2018, this trend had reversed: service revenue rose to 40.8%, while the share of drug revenue declined to 32.7%.
The cost structure of hospitals has also undergone significant changes over the years. In 2014, pharmaceutical expenses accounted for 30.3% of the costs in public hospitals, while labor costs represented only 14.8%. By 2018, the share of pharmaceutical expenses had slightly decreased to 28.6%, whereas labor costs rose substantially to 34.4%.
Nevertheless, there remains a significant gap between the revenue and cost structures of hospitals in China and those of German hospitals that have implemented the DRG-PPS system. In German hospitals, pharmaceutical costs account for only 4% of total costs; even when including medical supplies, which constitute 15%, the combined proportion remains below 20%. In contrast, labor costs in German hospitals exceed 60%.
Therefore, implementing the DRG-PPS will optimize hospitals’ revenue and cost structures, steer them away from the path of over-treatment, effectively alleviate patients’ financial burden, and ensure the long-term sustainability of medical insurance funds.
To adapt to the DRG-PPS, hospitals need to improve the overall quality of medical services as much as possible, i.e., increase the difficulty and breadth of case grouping, thereby stimulating hospitals to shift towards enhancing the value of technical labor and increasing hospital staff income. Therefore, from a revenue perspective, DRG-PPS has a direct incentive effect on doctors.
In contrast, physicians also play a crucial role in the smooth implementation of the DRG-PPS. Clinicians are key to the accurate completion of the medical record face sheet, which directly determines the appropriateness of case grouping. Inappropriate grouping due to non-compliant medical record face sheets may, in minor cases, result in denial of reimbursement by medical insurance and financial losses for the hospital; in severe cases, it may lead to penalties arising from repeated instances of unintentional medical insurance fraud.
Certainly, DRG may also lead to some unintended behaviors, such as: hospitals refusing critically ill patients and only admitting cases that are profitable; cost-cutting resulting in inadequate medical services and a decline in the quality of drugs and consumables; splitting hospitalizations, shifting costs to outpatient care; and overdiagnosis.
Meanwhile, as hospitals focus primarily on the costs associated with the DRG-PPS system, they tend to overlook other critical aspects, such as nursing care. Currently, the pricing of nursing services in China significantly deviates from actual costs. For instance, in Beijing, the price for Level I nursing care remained at only 7 RMB per day for two decades. This severe mismatch between costs and revenue has resulted in nearly all hospitals across China having nurse-to-bed and nurse-to-physician ratios below the standards issued by health authorities.
In fact, high-quality nursing care significantly enhances overall medical quality. Otherwise, even a high-quality surgical procedure may be substantially compromised by inadequate nursing care, potentially leading to adverse medical events or even medical malpractice. Notably, the labor cost of nurses is considerably lower than that of physicians. Therefore, under the DRG-PPS payment system, hospitals must also place greater emphasis on nursing care.
In addition to issues of medical quality, healthcare institutions may engage in upcoding—intentionally assigning higher-weight codes to simple diseases treated—in order to secure higher health insurance reimbursements. Through various maneuvers, these institutions can also increase insurance payouts by shifting portions of patient treatment to outpatient settings for cross-subsidization or by splitting a single hospitalization into two or more separate admissions.
Upcoding, in particular, is not uncommon in countries and regions that have previously implemented DRG-PPS. Chen Xianli believes that, from the perspective of economic interests, hospitals are inevitably prone to such practices. In fact, some vendors have already attempted to cater to these demands by providing technical means for hospitals to engage in upcoding. However, hospitals should fundamentally recognize that DRG is not merely a tool for payment reform but also a management instrument that can genuinely help hospitals strengthen internal management and enhance long-term competitiveness.
Drawing on the practices of other countries, China can mitigate these unintended behaviors by establishing a unified DRG regulatory framework, periodically adjusting DRG groupings, introducing clinical pathways to enhance standardization of diagnosis and treatment processes, leveraging information systems for real-time monitoring of healthcare quality, and formulating policies to ensure the quality and safety of medical services along with corresponding incentive measures.
By examining the experiences of other countries and regions, Chen Xianli believes that the implementation of DRG-PPS has the potential to increase the share of commercial health insurance in China’s healthcare payment system. Taking the United States as an example, the proportion of commercial health insurance in U.S. healthcare payments grew rapidly after the adoption of DRG-PPS.
The rapid rise of commercial health insurance is straightforward: it covers many new medical supplies, pharmaceuticals, and therapies that public health insurance does not, thereby providing policyholders with higher-quality medical services. In contrast, the role of public health insurance in the United States has gradually evolved into a basic coverage plan, reimbursing only the most essential medications and treatments.
Chen Xianli explained that U.S. physicians initially categorize patients into three groups based on payment methods: those with commercial insurance, those with public health insurance, and self-pay patients. While ensuring basic medical quality, different insurance plans cover varying costs, which may lead to differences in selected diagnostic and treatment protocols. For patients covered by public health insurance, doctors may opt only for foundational treatment approaches. In contrast, patients with commercial insurance can choose novel therapies with rapid efficacy and fewer side effects, thereby enhancing their healthcare experience.
So, how should hospitals respond to the upcoming DRG-PPS reform? Enhancing refined operational management is clearly the only effective approach.
Adjustment of Hospital Operating Models: Implementing Refined Operational Management
Lu Bei, Deputy Director of the Medical Insurance Office at Fuwai Hospital, Chinese Academy of Medical Sciences, believes that the approach to refined hospital management should begin with process management of clinical pathways and comprehensive evaluation of disease-specific management. This aims to form a closed loop integrating cost control, performance assessment, and quality evaluation, thereby achieving reasonable revenue under the DRG payment system through refined management. The specific implementation steps for preparing hospitals for refined management can be carried out in four phases: optimization of internal diagnosis and treatment processes, centralized procurement of drugs and consumables, informatization of medical insurance coding, and refined disease-specific management.
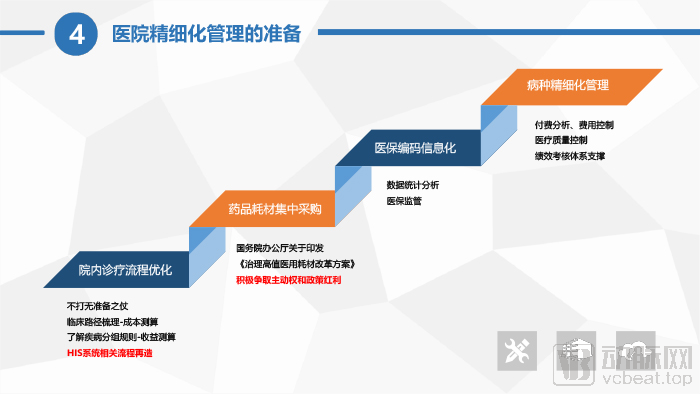
Image sourced from conference materials; used with authorization from the rights holder.
Chen Xianli also expressed a similar view, stating that hospitals must first implement refined management based on costs and an overall cost-control system. On this basis, she believes the most core issue is that hospitals need to adjust their structures and optimize clinical pathways—specifically, how hospitals can ensure medical quality while efficiently utilizing resource consumption on the foundation of guaranteed quality, and how they can optimize diagnosis and treatment plans. This process requires the joint integration of clinical teams and refined operational management teams, and can only be accomplished through the restructuring of hospital information systems.
At the top-level design stage, hospitals can also leverage management tools—including performance appraisal and bonus systems, cost control, Diagnosis-Related Group Prospective Payment System (DRG-PPS), and the Resource-Based Relative Value Scale (RBRVS) physician compensation model—using performance metrics as a lever to regulate physicians’ behavior, thereby ensuring the smooth implementation of refined hospital operational management.
How Information Technology Restructuring Supports Refined Operational Management in Hospitals
Chen Xianli proposed that informatization restructuring can play a significant role in helping hospitals optimize diagnosis and treatment plans. First, information technology tools, such as intelligent coding and medical record quality control, can assist hospitals in achieving accurate coding.
Through these measures, the quality of hospital medical records can be significantly improved, and coding results will be more accurate, preventing potential "under-coding" or "over-coding." This ensures that hospitals do not fail to receive due compensation due to under-coding, nor do they engage in potential health insurance fraud due to over-coding. In the long run, only accurate coding can provide a reliable reference for subsequent optimization and improvement in hospitals.
Secondly, and more importantly, under the DRG system, hospitals must prioritize adjusting their case-mix and disease-type structures based on accurate coding and grouping. The key challenge is to deliver care with rational resource utilization while ensuring diagnostic and treatment quality as well as a positive patient experience; this is what hospitals need to focus on most in responding to DRG payment reform. Information-based tools—such as DRG cost accounting, DRG cost control systems, and specialized disease management training platforms—can help hospitals strengthen management in these areas. If physicians continue to follow established habitual practices, these information systems can provide alerts and recommend alternative diagnostic and treatment plans that align with both quality standards and cost-containment objectives for their reference.
Finally, the informatization restructuring should also incorporate evaluations of diagnostic and therapeutic outcomes, including metrics such as cure rates and 30-day readmission rates, to prevent drawbacks such as under-treatment.
She also stated that information technology restructuring is a personalized solution. An identical diagnosis and treatment protocol may be profitable at Hospital A but result in losses at Hospital B. Therefore, IT restructuring helps hospitals determine the diagnosis and treatment protocols best suited to their specific circumstances.
The comprehensive informatization restructuring is a systematic engineering endeavor, which inevitably gives rise to numerous derivative issues. Merely adjusting medical record quality or solely addressing upcoding in health insurance reimbursement yields limited benefits. The correct approach for hospitals is to implement refined management through end-to-end informatization restructuring, thereby effectively responding to DRG-PPS and even achieving greater development.
Chen Xianli introduced that hospitals often encounter many problems in the early stage of information reconstruction. According to current experience, hospitals usually need about one year to adapt to the impact brought by DRG-PPS.
Meanwhile, Chen Xianli believes that with the implementation of DRG-PPS, hospitals will pay more attention to costs. However, this does not mean that hospitals should compress costs without limits. Hospitals must first ensure medical quality, then consider reasonable resource consumption, and should not pursue the lowest cost in all aspects. Information technology tools can help hospitals understand the priorities of cost control.
During the current outbreak of novel coronavirus pneumonia, excessive cost-cutting has led to certain problems. Some hospitals, in their pursuit of ultra-refined management, have even mandated zero inventory for medical consumables, resulting in insufficient disaster preparedness. Consequently, when a major public health emergency arises, there is a severe shortage of protective supplies. Therefore, Chen Xianli believes that refined operational management must be balanced; it should focus on reasonable resource consumption rather than minimizing resource costs at all costs.
With the implementation of DRG-PPS and the National Healthcare Security Administration’s “teng long huan niao” strategy (phasing out markups on consumables and pharmaceuticals to make room for increased service fees), hospitals will focus on boosting revenue from medical services. Meanwhile, new technologies may enhance medical quality and patient experience, ensuring greater procedural consistency and reducing medical risks. In the long run, novel therapies could potentially lower overall costs. Of course, all these benefits will become evident once data collection and analysis are achieved through informatization-driven restructuring.
Hospitals Must Shift Their Mindset and Proactively Support the Implementation of Tiered Diagnosis and Treatment Under the DRG-PPS
DRG-PPS may ultimately facilitate the implementation of tiered diagnosis and treatment, a policy that has long struggled to gain traction. Chen Xianli illustrates this point using cataract surgery, which can be performed in both tertiary (Grade III) and secondary (Grade II) hospitals with minimal differences in quality. Since tertiary hospitals have more expensive equipment and higher labor costs, the cost of performing surgeries is obviously higher. Assuming the cost at a tertiary hospital is 5,000 yuan and at a secondary hospital is 3,000 yuan, a uniform DRG-PPS payment of 4,000 yuan would result in a loss for the tertiary hospital but a surplus for the secondary hospital. Consequently, tertiary hospitals may reduce their volume of such procedures.
Meanwhile, this objective can also be achieved from the perspective of DRG performance evaluation: if tertiary Grade A hospitals undertake an excessive number of cases with low Case Mix Index (CMI), their overall CMI will decline, thereby adversely affecting their institutional ratings. In such circumstances, these hospitals will adjust their operational strategies, and participation in urban medical groups and county-level medical consortia represents a viable approach.
Under the previous extensive growth model, tertiary hospitals could generate profits regardless of the conditions treated, leading to continuous expansion and even the emergence of “super-hospitals.” In this context, the so-called tiered diagnosis and treatment system often became merely formalistic, as tertiary and secondary hospitals failed to form a community of shared interests.
With the implementation of DRG-PPS, tertiary hospitals, under the dual pressure of payment reforms and performance assessments, can form alliances with community hospitals to establish large urban medical groups or county-level medical consortia. As resources are integrated and barriers in human resources, finance, procurement, and other areas are systematically removed, these tightly integrated medical consortia will ultimately evolve into genuine interest groups. Chen Xianli believes that under this model, complex and critical cases will be managed by central hospitals, while common conditions will be treated by subordinate facilities, thereby achieving the goal of tiered diagnosis and treatment.
DRG-PPS can also promote the development of private hospitals. Under the premise of equivalent medical quality, regardless of whether a hospital is public or private, those with lower costs will offer more affordable care and thus gain greater advantages. Compared with public hospitals that are relatively resource-rich, private hospitals with limited resources have always placed greater emphasis on cost control and refined management, which may become their competitive advantage.
The implementation of the DRG-PPS is an irreversible reality. Whether hospitals can survive, let alone thrive and expand, in this competitive landscape will depend on their clinical service capabilities and the level of refined operational management.
Hospitals need to transform their management philosophies and models; achieve effective integration of operational and financial management; implement the integration and restructuring of information systems to enable refined, data-driven management; and prioritize data quality by standardizing data entry processes.
For the unprepared, DRG-PPS may spell disaster; yet for practitioners who are well-prepared and persistent, it could present a new opportunity.