A Cloud Over the Cath Lab: An Introduction to the Mitral Valve Interventional Therapy Industry and Product Landscape
Preface
Cast your mind back 120 years, to the last day of the 19th century. Standing at the turn of the century, Lord Kelvin, then the most authoritative figure in physics, delivered his now-famous speech during the Royal Society’s New Year address: “The grand edifice of physics has been completed; all that remains is some finishing work... Yet its beautiful and clear sky is now overshadowed by two dark clouds.” It was precisely these two “dark clouds” that eventually gave rise to relativity and quantum mechanics, both of which have had a profound impact on science.
In 1929, Werner Forssmann, a young German surgeon, inserted a catheter from his own antecubital vein into the right atrium under fluoroscopic guidance, thereby ushering in the era of interventional cardiology. Dr. Forssmann was awarded the 1956 Nobel Prize in Physiology or Medicine for his pioneering contributions to the field of cardiac catheterization.
To date, cardiovascular interventional medicine has undergone 90 years of vigorous development. It is fair to say that the “edifice of cardiovascular intervention” has been largely completed. Built upon this slender catheter, countless scientists, physicians, and patients have made remarkable contributions. Subspecialties such as coronary intervention, neurointervention, and peripheral intervention have flourished, with a continuous emergence of innovations including coronary stents, transcatheter heart valves, thrombectomy stents, endovascular grafts for large arteries, and various types of catheters and guidewires. However, hovering above this “edifice of intervention” is a disquieting cloud—the very subject of our discussion today: transcatheter mitral valve therapy.
[Article Highlights]
I. The Mitral Valve Treatment Market Is Vast
Mitral valve disease is the most common type of valvular heart disease, and an aging society will lead to a large population of patients.
Treatment of Mitral Regurgitation (MR): AHA/ACC Guidelines Prioritize Repair
Low penetration rate of surgical procedures, with a gradual shift from open surgery to minimally invasive and interventional therapies
The Mitral Valve Intervention Market Is Worth Hundreds of Billions; With MitraClip Now Launched in China, the Future Looks Promising
II. Summary of Mitral Regurgitation Treatment Technologies
Surgical techniques for the mitral valve are well-established, and most interventional procedures follow surgical approaches.
Multiple interventional devices have obtained U.S. FDA clearance and EU CE marking, and are commercially available.
Preliminary Success Achieved by China’s Self-Developed Interventional Therapy Devices
Additional Findings: Imaging Devices for Interventional Therapy
III. Summary and Outlook
1.1. Mitral valve disease is the most common type of cardiac valvular disease
For decades, cardiovascular disease has remained the leading cause of death worldwide. In China, the mortality rate from cardiovascular disease has risen by 65% over the past three decades (GBD Compare). Cardiovascular diseases include atherosclerosis, myocardial infarction, stroke, arrhythmia, and valvular heart disease. Valvular disorders, including those affecting the aortic, pulmonary, mitral, and tricuspid valves, are among the major contributors to adverse cardiac events such as heart failure and stroke. Among all valvular diseases, mitral valve pathology is the most prevalent.
Mitral valve diseases primarily include mitral regurgitation (MR) and mitral stenosis (MS). Mitral regurgitation refers to the incomplete closure of the mitral valve orifice and the subsequent backflow of blood into the left atrium, caused by structural or functional abnormalities in any of the following components: the leaflets, annulus, chordae tendineae, papillary muscles, or left ventricle. Regurgitation leads to increased blood volume and elevated pressure in the left atrium, as well as increased pulmonary venous pressure. Severe cases can result in pulmonary edema, myocardial injury, heart failure, and even death. Mitral stenosis refers to the narrowing of the mitral valve opening, which impedes blood flow from the left atrium to the left ventricle. Insufficient supply of oxygen-rich blood leads to fatigue and dyspnea. The accumulation of blood in the left atrium increases left atrial pressure and causes left atrial enlargement, which can also trigger pulmonary edema.
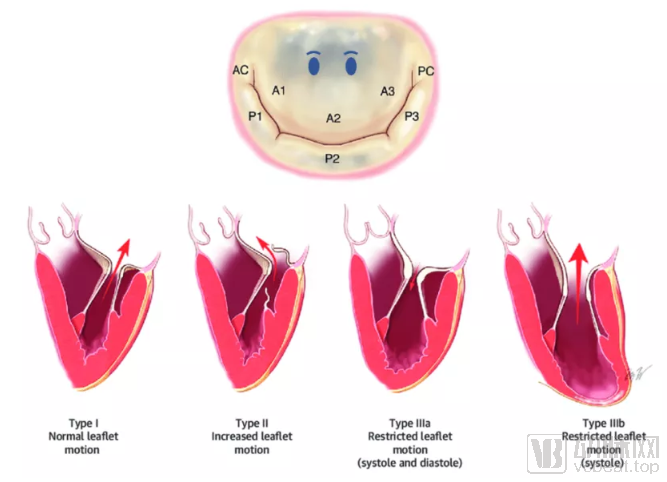
Figure: Classification of Mitral Regurgitation
1.2. An Aging Society Will Bring a Huge Population of Patients
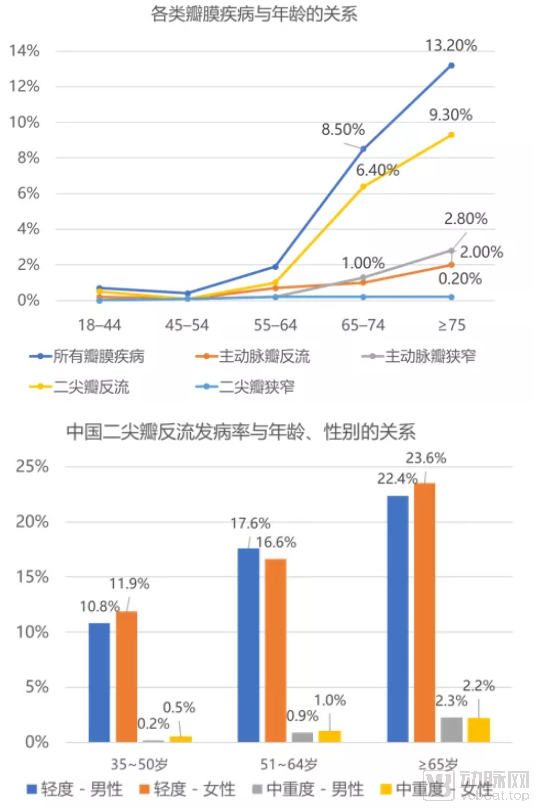
According to a population-based study by the Mayo Clinic in the United States, the incidence of various valvular heart diseases increases with age, with mitral regurgitation (MR) exhibiting a significantly higher incidence than aortic stenosis, aortic regurgitation, and mitral stenosis. The incidence of MR was 6.4% among individuals aged 65–74 years and reached 9.3% in those aged 75 years and older.[1] A survey conducted by Fuwai Hospital of the National Center for Cardiovascular Diseases among individuals aged 35 years and older also found a positive correlation between MR incidence and age. Among those aged 65 years and older, the incidence of mild MR was as high as 23%, while that of moderate-to-severe MR reached 2.3% (Figure 1).[2] With the advent of an aging society, the proportion of the population aged 65 years and older has continued to rise. In China, this proportion increased from 6.91% in 2000 to 11.19% in 2018 and is projected to reach 17.22% by 2035. At that time, the number of Chinese residents aged 65 years and older will exceed 250 million. Assuming a prevalence rate of 10% for moderate or severe MR, the total number of MR patients will surpass 25 million.
Figure 1: Relationship between valvular heart disease and age in the United States (top); Incidence of mitral regurgitation in China by age and sex (bottom). Source: References [1][2], Shengshan Asset
The etiologies of mitral regurgitation are primarily categorized into two major types: primary and secondary (also known as functional). Primary pathology refers to valvular insufficiency caused by structural and functional abnormalities of the mitral valve itself, including degenerative disease, papillary muscle dysfunction, infective endocarditis, and rheumatic heart disease. Secondary pathology refers to regurgitation resulting from mitral annular dilation due to left ventricular dysfunction associated with ischemic heart disease and other cardiomyopathies. A study based on an echocardiographic database at Zhongshan Hospital indicated that primary and secondary pathologies each accounted for 50% of patients with severe MR, with degenerative disease comprising 63% of primary cases.[3] Another survey conducted at the Second Affiliated Hospital of Zhejiang University School of Medicine found that the proportions of secondary and degenerative lesions (including mitral valve prolapse) among patients increased with age (Figure 2).[4] It is foreseeable that with population aging, degenerative mitral valve disease will become more prevalent, leading to a rapid increase in the number of affected individuals.
Figure 2: Etiological Distribution of Mitral Regurgitation in China (Top); Etiological Distribution of Mitral Regurgitation by Age Group in China (Bottom)
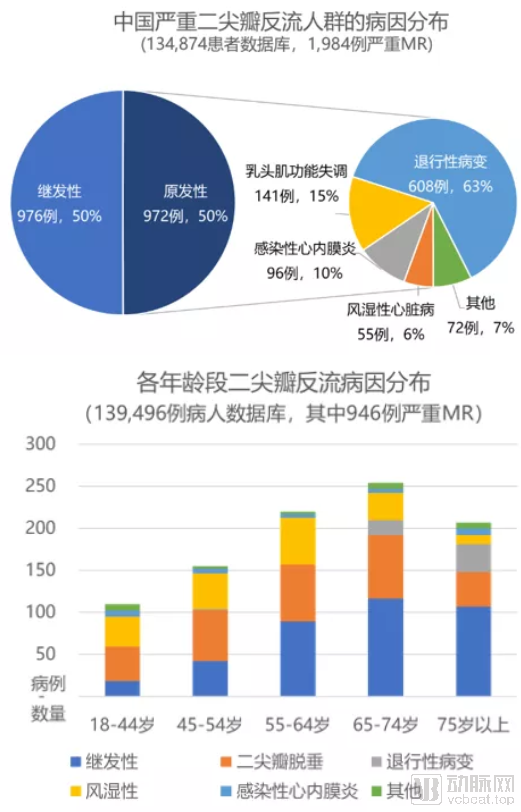
Sources: References [3][4], Shengshan Asset
According to the Guidelines for the Management of Valvular Heart Disease issued by the American Heart Association (AHA) and the American College of Cardiology (ACC), mitral regurgitation (MR) can be classified into three distinct stages—risk stage, progressive stage, and severe lesion stage—based on indicators such as valve morphology, the ratio of regurgitant jet area to left atrial area (RJA/LAA), vena contracta, regurgitant volume (RV), regurgitant fraction (RF), and effective regurgitant orifice area (ERO) (the classification criteria differ for primary and secondary MR) (Table 1). Due to compensatory mechanisms in cardiac function, chronic MR may remain asymptomatic for a prolonged period; therefore, within the severe lesion stage, MR is further categorized into symptomatic and asymptomatic types. Most patients with asymptomatic severe regurgitation may develop symptoms or require surgical intervention within 5 to 10 years after diagnosis, indicating that MR is characterized by a long disease course, low diagnosis rate, and a large population of potential patients.
Table 1: Stage Classification and Criteria for Primary and Secondary Mitral Regurgitation
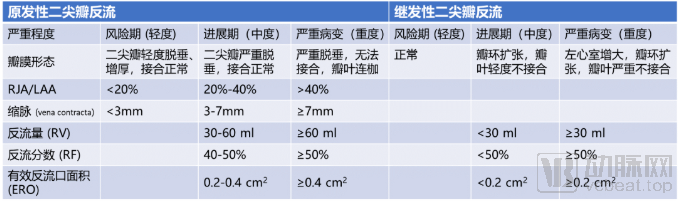
Source: 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease, Shengshan Asset
1.3. Treatment of MR: AHA/ACC Guidelines Prioritize Repair
Since mitral regurgitation is an organic lesion, no current medications can alter the progression of the disease; they only serve to alleviate symptoms. Therefore, surgery remains the primary treatment modality. Depending on the underlying etiology (primary vs. secondary), the stage of disease progression (progressive phase vs. severe pathology), as well as specific clinical indicators and associated symptoms, management options include regular monitoring or surgical valve intervention (Figure 3). Surgical valve interventions are categorized into repair and replacement. In the 2014 guidelines, transcatheter edge-to-edge repair (MitraClip) was included as a treatment option for the first time, marking a gradual shift in mitral valve therapy from open surgery to catheter-based interventions. Given the higher safety profile of valve repair, the guidelines recommend prioritizing repair over replacement, tailored to the patient’s individual clinical circumstances.
Figure 3: Treatment Pathway for Mitral Regurgitation
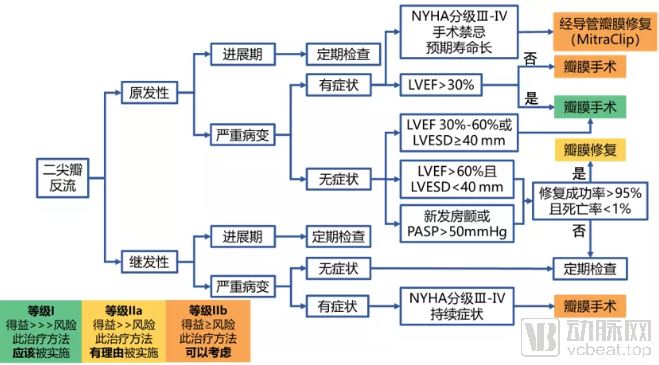
Source: 2014 AHA/ACC Guideline on the Management of Valvular Heart Disease, Shengshan Asset
1.4. Low Penetration Rate of Surgical Mitral Valve Procedures
In China, the estimated total number of patients with moderate-to-severe mitral regurgitation (MR) reaches 16.8 million. Among them, approximately 6.84 million patients have severe MR with symptoms requiring surgical intervention. However, due to the high risks associated with traditional open-heart surgery—which requires thoracotomy, cardiopulmonary bypass, and cardiac arrest—only about 50% of these patients are eligible for surgery. Currently, only around 40,000 mitral valve surgeries are performed annually in China, resulting in a surgical penetration rate of less than 1%. Similarly, in the United States, only 30,000 surgeries are conducted among the approximately 1.67 million MR patients who require surgical treatment. The combination of low diagnosis rates, low treatment rates, and high surgical risks has led to an accumulating backlog of MR patients with worsening conditions, highlighting a significant unmet need for safe and effective therapeutic options. Furthermore, improving diagnosis rates and providing early preventive repair for asymptomatic patients are crucial strategies for extending survival and enhancing quality of life.
Figure 4: Treatment Pathway for Mitral Regurgitation
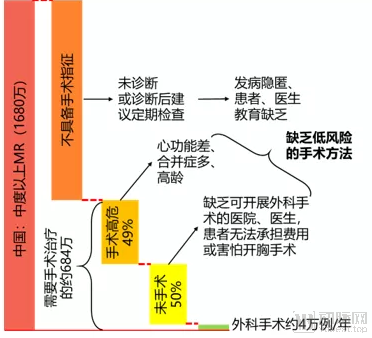
Source: Public Information, Shengshan Asset
1.5. Mitral Valve Treatment Shifts from Surgical Procedures to Minimally Invasive and Interventional Therapies
The team led by Academician Ge Junbo, a renowned cardiologist in China, proposed that heart valve therapy can be divided into three eras (Table 2): The 1.0 era, or the era of traditional surgical valve replacement, dates back to the early 20th century. It involves median sternotomy, complete sternal splitting, and opening and exposing the heart for surgery. This approach is suitable for treating complex lesions but requires cardiopulmonary bypass and cardiac arrest, resulting in significant trauma and high risk. The 2.0 era, or the era of minimally invasive surgical therapy, began to develop gradually in the late 20th century. It utilizes small incisions and avoids complete sternal splitting to reduce surgical trauma. This approach offers advantages such as less postoperative pain, faster recovery, reduced blood loss, and smaller scars, but still requires cardiopulmonary bypass and cardiac arrest. The 3.0 era, or the era of transcatheter therapy, involves repairing or replacing valves via peripheral vascular access to the heart. It does not require thoracotomy, cardiopulmonary bypass, or cardiac arrest, significantly reducing surgical mortality and postoperative complication rates in patients who are contraindicated for or at high risk from traditional surgery.[5] Currently, transcatheter aortic valve replacement (TAVR) has matured and been widely adopted globally, while transcatheter mitral valve repair, represented by MitraClip, is also progressively developing.
Table 2: Eras of Heart Valve Therapy
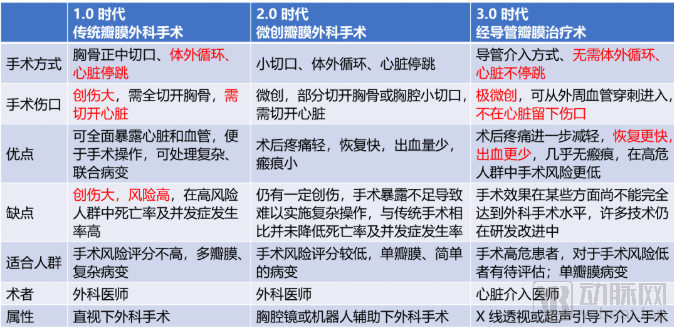
Source: Reference [5], Shengshan Asset
Transcatheter mitral valve therapies are also categorized into repair (Transcatheter Mitral Valve Repair, TMVR) and replacement (Transcatheter Mitral Valve Implantation, TMVI). Current transcatheter repair techniques include edge-to-edge repair, artificial chordae tendineae implantation, and annuloplasty ring implantation. These procedures share the same principles as surgical interventions but deliver repair devices to the mitral valve via minimally invasive approaches, such as transfemoral or transapical access. This method maximizes preservation of the native mitral valve structure, offering high safety profiles but carrying a risk of recurrence. TMVI involves delivering a prosthetic valve (primarily a bioprosthetic valve) to the mitral position via transfemoral or transapical routes; after deployment, it is anchored within the annulus to replace the diseased valve. Currently, TMVI appears to have lower safety margins and carries a risk of bioprosthetic valve degeneration.[6]
Although mitral valve surgery is a relatively mature technique, its significant invasiveness and high surgical risk have hindered the increase in procedural penetration. Therefore, it is anticipated that the market for minimally invasive interventional therapies will experience rapid growth over the next five to ten years, starting with patients at high surgical risk and gradually expanding to those at moderate and low risk, ultimately becoming the primary treatment modality for mitral regurgitation.
1.6. Market Size Estimation for Transcatheter Mitral Regurgitation Interventional Procedures in China (Primarily Edge-to-Edge Repair)
Starting with a population of 16.8 million individuals with moderate-to-severe mitral regurgitation (MR) in China in 2019, and assuming an annual growth rate of 3%, the number of patients with moderate-to-severe MR in China is projected to exceed 20 million by 2025. Among these patients, approximately 40% require surgical intervention, and about 50% of those requiring surgery are classified as high-risk. Currently, Abbott’s MitraClip edge-to-edge repair system is the only transcatheter therapy available globally. Based on sales data from the second quarter of 2019, the estimated global sales volume for the full year 2019 was approximately 18,000 units, resulting in a penetration rate of around 0.12% among the global high-risk patient population [7].
Based on this, a conservative estimate suggests that the volume of transcatheter mitral valve interventions in China will reach approximately 6,000 cases by 2025. Currently, the MitraClip system is priced at around RMB 200,000. Assuming a slow price decline, with the price dropping to RMB 170,000 by 2025, the total market size would reach RMB 1 billion. If surgical penetration grows rapidly, reaching 0.8% by 2025, and prices drop more quickly to an end-user price of RMB 120,000 by 2025, the total number of procedures would exceed 30,000, resulting in a total market size of nearly RMB 4 billion (Table 3). Considering population aging and improved diagnosis rates, the growth rate of the total patient population will accelerate. Advances in interventional techniques will increase the number of patients eligible for surgery. As mitral valve intervention devices become increasingly commercialized and insurance coverage expands, patients’ affordability will improve, further driving up surgical penetration rates. In light of these factors, it is predicted that the market for mitral valve interventions and related devices in China will be substantial, with broad prospects.
Table 3: Estimation of the Mitral Valve Surgery Market in ChinaSource: Public Information, Shengshan Asset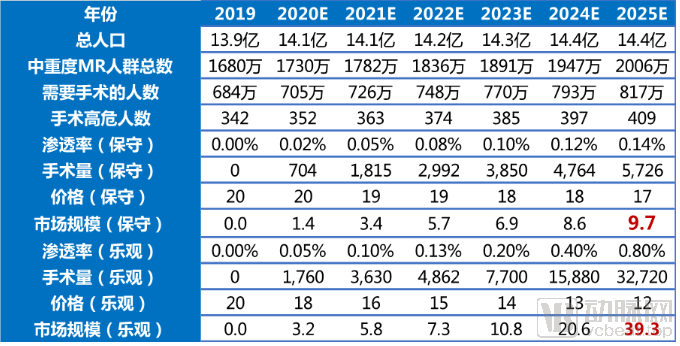
After decades of development in cardiac surgery, particularly with the increasing maturity of surgical mitral valve repair, mitral valve intervention techniques, as a later arrival, have largely been guided by the principle of replicating and mimicking the procedures and outcomes of open-heart surgery as closely as possible. Therefore, before discussing interventional techniques, we first review surgical approaches to the mitral valve.
Surgical treatment for mitral regurgitation is categorized into two approaches: repair and replacement. Globally, surgical repair accounts for more than 70% of cases. The specific techniques employed in repair surgery vary depending on the location of the mitral valve lesion. Traditional techniques for posterior leaflet prolapse include quadrangular resection, triangular resection, sliding leaflet repair, and folding technique. Common techniques for bileaflet prolapse include artificial chordae implantation, edge-to-edge repair, and annuloplasty. Among these, leaflet repair is often supplemented with the implantation of an annuloplasty ring to further stabilize the annulus and reduce recurrence. Currently, mitral valve repair surgery has matured significantly; the mortality rate for various repair procedures is approximately 1%, the five-year reoperation rate is below 10%, and the recurrence rate is under 20%, indicating that both safety and efficacy have reached high standards.[8]
For patients with poor native mitral valve anatomy that is difficult to repair, mitral valve replacement is performed. Similar to aortic valve replacement, prosthetic mitral valves are categorized into mechanical and biological valves (Figure 5). Mechanical valves are commonly used in younger patients; although durable, they require lifelong anticoagulation therapy. Biological valves are typically preferred for older patients; they necessitate only short-term anticoagulation but have an effective lifespan of approximately 10 to 20 years. Compared with aortic valve replacement, mitral valve replacement is more challenging and carries higher risks due to the complex native anatomy that complicates secure fixation, the diverse etiologies, and the risk of left ventricular outflow tract obstruction. Consequently, existing aortic valve products cannot be directly applied to the mitral position.
Figure 5: Schematic diagram of a prosthetic mitral valve
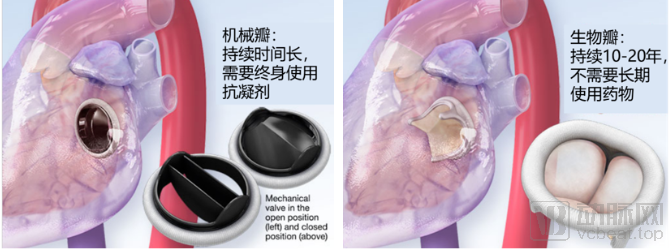
Source: American Heart Association, Shengshan Asset
2.1. Rapid Growth in Mitral Valve Surgery Volume, with Repair Remaining the Mainstream Approach
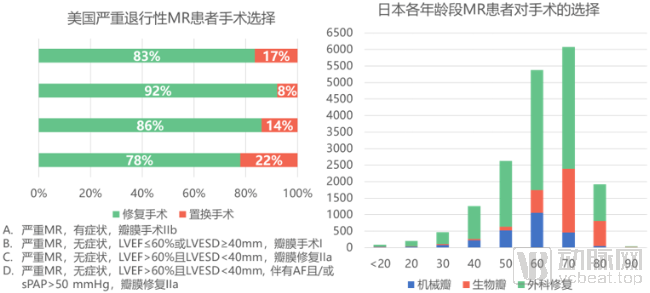
A U.S. study based on a cardiothoracic surgery database found that from 2011 to 2016, the volume of isolated mitral valve surgeries increased by 24%, with a compound annual growth rate (CAGR) of 4.4%. The growth was even faster among patients with degenerative lesions, reaching a CAGR of 7.6%, significantly outpacing the overall growth in cardiac surgery volume (CAGR of 2.1%). Among mitral valve surgeries performed for degenerative leaflet prolapse, repair procedures accounted for more than 80%, while replacement procedures ranged from 8% to 22% across various patient groups (Figure 6, left). [9] A survey in Japan also found that surgical repair was the predominant choice for patients with mitral regurgitation across all age groups, and the proportion of patients receiving bioprosthetic valves increased with age (Figure 6, right). [10]
Figure 6: Surgical Options for Patients with Severe Degenerative Mitral Regurgitation Source: References [9][10], Shengshan Capital
Compared with valve replacement, valve repair demonstrates superior safety in terms of intraoperative, postoperative, and long-term outcomes (Figure 7) [11][12][13]. Multiple meta-analyses have also indicated that mitral valve repair is associated with lower mortality but a higher recurrence rate compared with valve replacement [14][15].
Figure 7: Comparison of Intraoperative, Postoperative, and Long-Term Outcomes of Mitral Valve Repair and Replacement
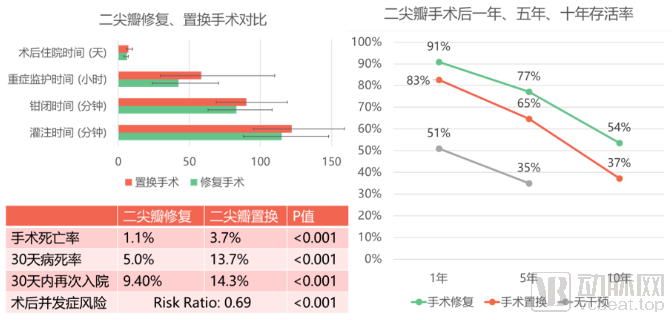
Source: References [11][12][13], Shengshan Assets
2.2. Multiple interventional devices have obtained U.S. FDA and EU CE certifications for commercial use
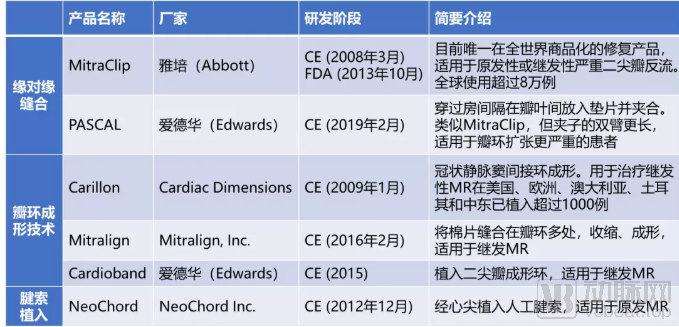
Since the first MitraClip implantation in 2003, the field of interventional devices for the mitral valve has made significant progress. Currently, more than 50 devices for treating mitral regurgitation have entered animal testing stages globally, with over 20 advancing to early-phase human trials. As of February 2019, six repair products had received CE marking in the European Union, among which one (Abbott’s MitraClip edge-to-edge repair system) had obtained FDA approval and was commercially available in multiple countries and regions, including Europe, North America, and Japan. The following provides a brief overview of the status and advancements of several categories of interventional mitral valve products.
2.2.1. Edge-to-Edge Repair
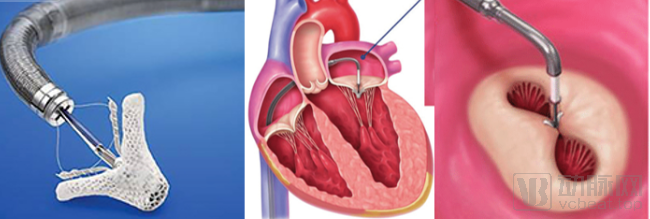
Abbott – MitraClip: The MitraClip, an edge-to-edge repair device, was originally developed by Evalve, Inc., a cardiac valve interventional device R&D company founded in California, USA, in 1999. The delivery catheter is advanced via the femoral vein through the inferior vena cava and across the interatrial septum into the heart to grasp the mitral valve leaflets; once adjusted to the optimal position, the clip is deployed to reduce the valvular orifice area (Figure 8). The product took shape in 2002, with the first successful human implantation performed in 2003. Feasibility studies were conducted in 2006, and CE certification was obtained in March 2008. In November 2009, Abbott acquired Evalve, Inc. for $410 million. The MitraClip received FDA approval in 2013, was approved for marketing in Canada the following year, and gained approval in Japan in 2017. As of March 2019, more than 80,000 patients worldwide had undergone mitral valve repair using the MitraClip system.
Figure 8: Schematic of the MitraClip Edge-to-Edge Mitral Valve Repair System. Source: Abbott Official Website, ResearchGate, Shengshan Asset
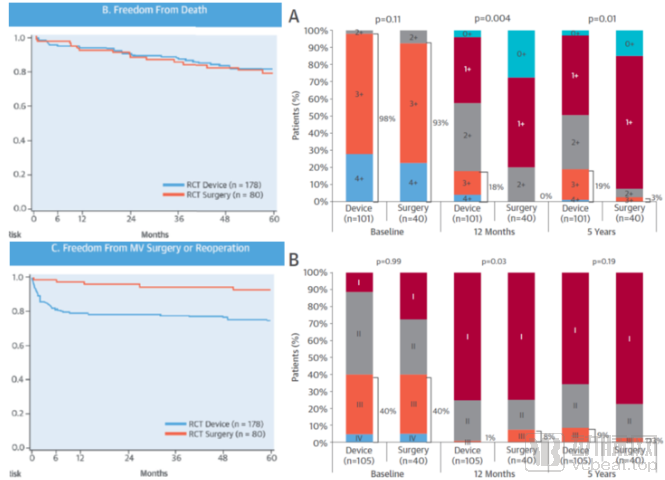
Multiple clinical trials have demonstrated the safety and efficacy of this product. The randomized controlled trial EVEREST II, conducted prior to FDA approval, enrolled patients with moderate-to-severe primary or secondary mitral regurgitation (MR) who met guideline-defined indications for surgical intervention. By comparing the MitraClip system with conventional surgical repair, the trial showed that the system significantly improved MR symptoms, with benefits sustained for up to five years post-procedure. Compared with the surgical group, there was no significant difference in mortality, although higher rates of recurrence and reoperation were observed (Figure 9). [16]
Figure 9: Results of the Abbott MitraClip Randomized Controlled Trial EVEREST II. Source: Reference [16], Shengshan Asset Management
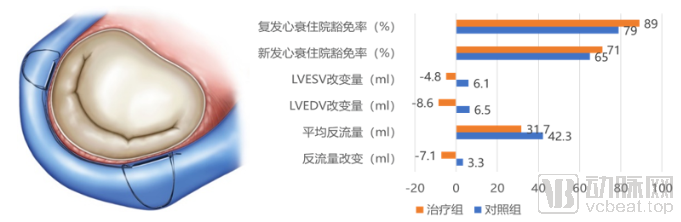
The COAPT trial, conducted after FDA approval, enrolled patients with moderate-to-severe secondary mitral regurgitation (MR) and heart failure who remained symptomatic despite maximally tolerated medical therapy. Compared with medical therapy alone, treatment with MitraClip reduced the annual rate of heart failure hospitalizations by nearly half and all-cause mortality by nearly 40% over 24 months (Figure 10) [17].
Figure 10: Results of the COAPT Clinical Trial for Abbott's MitraClip
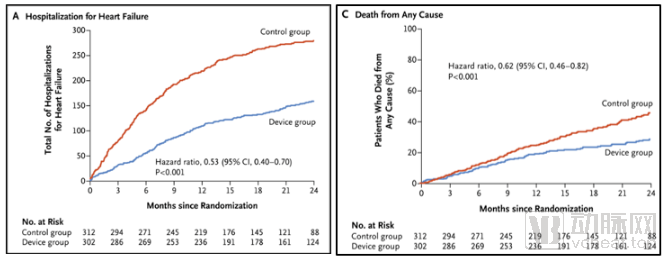
Source: Reference [17]
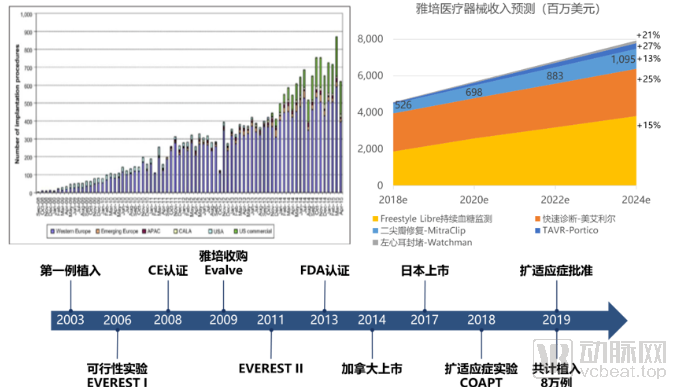
On March 14, 2019, based on the results of the COAPT clinical trial, the FDA approved an expanded indication for MitraClip to include heart failure patients with moderate-to-severe functional mitral regurgitation caused by left ventricular dysfunction. On July 15, 2019, Abbott announced that the fourth-generation MitraClip device, featuring additional size options and enhanced leaflet grasping capability, had received FDA approval. Currently priced at $25,000 per unit, the product achieved global sales of $627 million in 2018 and is experiencing rapid growth at a compound annual growth rate (CAGR) of 13%, making it a significant revenue source for Abbott’s medical device segment. From its initial launch, when the first-generation MitraClip was indicated only for symptomatic patients with severe primary mitral regurgitation who were contraindicated for surgery, to its subsequent expansion to cover patients at intermediate or high surgical risk regardless of whether the regurgitation was primary or secondary, and further to the rapid approval and surging sales of the third- and fourth-generation devices in recent years, MitraClip has demonstrated that transcatheter mitral valve repair (TMVR) products possess a substantial market, broad prospects, and immense application potential (Figure 11).
Notably, in June this year, MitraClip also received NMPA approval for market launch without the need for clinical trials, based on its robust clinical data. We look forward to its development in the Chinese market.
Figure 11: Global trends in MitralClip procedure volume from September 2008 to April 2015 (top left); Abbott Medical Devices revenue (top right); MitraClip product timeline (bottom). Source: Evaluate MedTech, public information, Shengshan Asset Management
Due to the compromise of the effective orifice area of the mitral valve and insufficient long-term efficacy, standalone edge-to-edge repair is rarely employed in surgical practice. However, in the field of interventional procedures, it remains the only method that is sufficiently safe for widespread commercial use. Therefore, although edge-to-edge repair is not the optimal choice from a technical standpoint, devices based on this technique continue to hold a place in the market.
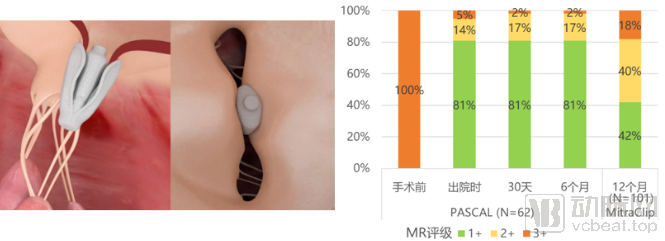
Edwards PASCAL: The PASCAL edge-to-edge repair system is similar to the MitraClip. The delivery catheter crosses the interatrial septum to access the mitral valve, where a central spacer is positioned between the leaflets, and grasping arms are used to reduce the orifice area and mitigate regurgitation. This product received CE Mark approval in February 2019. The latest clinical data from the CLASP trial, released on May 22, 2019, demonstrated a 95% device implantation success rate, a major adverse event rate of 6.5%, no occurrences of stroke or myocardial infarction, and significant improvement in mitral regurgitation (MR) sustained over six months (Figure 12). The FDA has currently approved the initiation of CLASP IIF, a multicenter, randomized, controlled pivotal trial comparing the PASCAL system with the MitraClip for the treatment of patients with moderate-to-severe or severe functional MR accompanied by heart failure symptoms. Although PASCAL and MitraClip belong to the same product category and PASCAL was developed and approved later, it offers advantages through its unique design, including independent leaflet manipulation and an increased effective coaptation area. These features not only enhance procedural success rates but also lay a solid foundation for long-term efficacy. Furthermore, as clinical data for PASCAL continue to accumulate, we believe it will enter the Chinese market in the near future.
Figure 12: Schematic of the Edwards PASCAL Edge-to-Edge Repair System and CLASP Clinical Trial Data Source: Meddevicetracker, Shengshan Capital
2.2.2. Annuloplasty
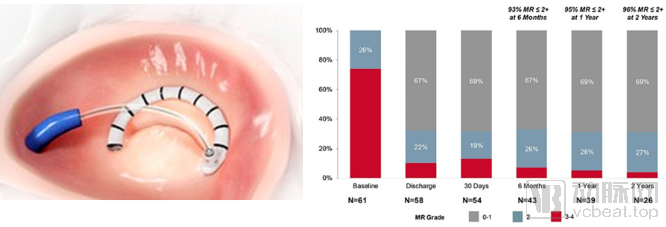
Cardiac Dimensions – Carillon: The Carillon device employs an indirect annuloplasty technique. It consists of proximal and distal anchors connected by a tensioning ribbon, which is delivered via a percutaneous catheter-based system and anchored in the coronary sinus and great cardiac vein. Contraction of the connecting ribbon tightens the mitral annulus. The product received CE marking in January 2009, with 1,000 implants completed by July 1, 2019. According to currently available clinical data, the device significantly improved regurgitation in patients with functional mitral regurgitation (MR). Compared with the control group, there was no significant difference in the incidence of adverse events, while hospitalizations for heart failure were significantly reduced (Figure 13). However, this technique carries a higher risk of compressing the left circumflex coronary artery and offers limited efficacy; thus, its prospects appear constrained amid competition among numerous annuloplasty technologies.
Figure 13: Schematic diagram of the Carillon indirect annuloplasty system (left) and clinical trial data (right))
Sources: Cardiac Dimensions official website, Meddevicetracker, Shengshan Asset
Mitralign, Inc. – Mitralign: The Mitralign annuloplasty system is a form of direct annuloplasty that utilizes a catheter-based delivery system to implant pledgets into the mitral annulus. By cinching the connection between two pledgets, the system reduces annular dimensions, making it primarily suitable for patients with functional mitral regurgitation (MR). The product received CE marking in February 2016, and multiple clinical trials are currently ongoing. Published clinical data demonstrate low 30-day all-cause mortality and adverse event rates, reduced MR severity, and improved cardiac functional class, confirming its safety and efficacy (Figure 14). However, as this system only implants and cinches pledgets at two locations outside the annulus, it cannot provide stable support comparable to an implanted annuloplasty ring. With continuous mitral valve opening and closing motions, there is a significant likelihood of recurrent annular dilation and MR recurrence. Furthermore, the procedure is technically complex and challenging to position accurately, which may hinder its widespread adoption in clinical practice.
Figure 14: Schematic diagram of the Mitralign annuloplasty system (top) and clinical trial data (bottom), including improvement in MR (left), improvement in cardiac function (center), and reduction in valve orifice diameter (right)
Source: MDDI Online, medgadget, Meddevicetracker, Shengshan Capital
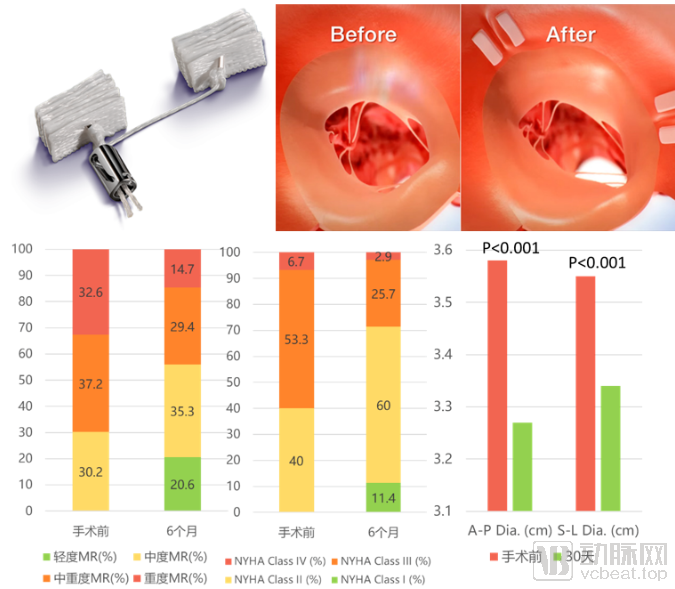
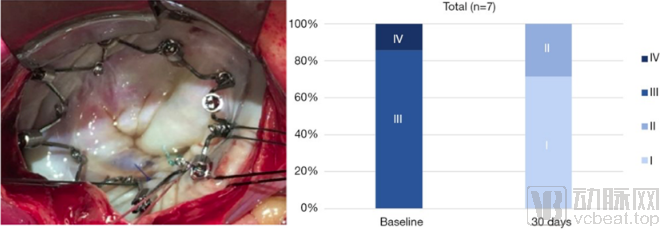
Edwards – Cardioband: The Cardioband is a posterior leaflet annuloplasty band designed for patients with functional mitral regurgitation (MR). The device involves percutaneous femoral access, transseptal puncture, and implantation of a non-closed annuloplasty ring at the mitral valve posterior annulus. Clinical trials have demonstrated an implantation success rate approaching 100%, a 30-day mortality rate below 5%, significant annular contraction, marked reduction in MR, and improved cardiac function sustained over two years (Figure 15). The device received CE marking in 2015 and remains in the phase of multicenter clinical trials. Unlike traditional surgical annuloplasty rings that are secured by sutures, the Cardioband requires fixation via multiple anchors implanted around the annulus, which may potentially cause myocardial injury and affect long-term efficacy.
Figure 15: Schematic Diagram of the Edwards Cardioband Annuloplasty System and Clinical Trial Results
Source: Edwards Official Website, Shengshan Asset
Boston Scientific – IRIS: The IRIS annuloplasty ring, developed by Millipede, Inc., adheres to the gold standard for mitral valve repair. Via femoral venous access and transseptal puncture, a complete semi-rigid nitinol ring is delivered to the mitral valve, where anchors are secured into the annular tissue. Tightening the implanted annuloplasty ring reduces the diameter of the patient’s dilated mitral valve orifice (Figure 16). In December 2018, Boston Scientific acquired Millipede for $325 million based on results from human clinical studies. According to currently published clinical data, the safety and efficacy of IRIS have been preliminarily validated.[18] As the first complete annuloplasty ring implantable via catheter, it may offer a lower rate of mitral regurgitation (MR) recurrence compared with “partial-ring” products (such as Cardioband). Furthermore, it can be used in conjunction with leaflet repair devices (such as MitraClip) to stabilize the annulus and prolong the durability of the repair. Similar to issues associated with Cardioband, implantation of anchors into the annulus carries a risk of myocardial tissue injury.
Figure 16: Schematic Diagram of the Boston Scientific IRIS Annuloplasty Ring and Clinical Trial Results
Source: Reference [18]
VALCARE, Inc. – AMEND: The AMEND transcatheter mitral valve repair system, developed by an Israeli medical device company, also mimics the annuloplasty rings most commonly used in current surgical procedures. It delivers a D-shaped ring to the supra-annular position via a transapical approach, securing it first to the posterior leaflet using a row of anchors, and then drawing the anterior leaflet closer to complete the fixation with the annuloplasty ring (Figure 17, left). In 2016, the company announced the completion of its initial first-in-human trials in Europe and Israel. The product remains in the research and development phase.
Figure 17: Schematic diagrams of the AMEND Annuloplasty System (left) and the AccuCinch Left Ventricular Restoration System (right)
Source: VALCARE, Ancora Heart Official Website, Shengshan Capital
Ancora Heart – AccuCinch Transcatheter Left Ventricular Repair System: Ancora Heart, a medical device company based in California, USA, has developed the AccuCinch system, the first transcatheter ventricular repair device designed to treat heart failure caused by left ventricular dysfunction and functional mitral regurgitation. The catheter is introduced via femoral artery puncture, advanced retrograde across the aortic valve into the left ventricle, where a pre-shaped guidewire is anchored to the left ventricular wall using rivets to directly inhibit left ventricular dilation (Figure 17, right). Unlike existing mitral valve annuloplasty systems, this subannular approach preserves the native mitral valve anatomy, leaving options open for potential future surgical interventions. Early feasibility studies are currently underway in the United States and Europe.
Given that most current surgical repair procedures involve suturing an annuloplasty ring onto the annulus, achieving high standards of safety and efficacy, interventional therapies are striving to mimic surgical repair to attain comparable or even superior outcomes. The key design considerations for annuloplasty systems primarily include shape (semi-ring or complete D-shaped ring), fixation location (supra-annular or sub-annular), and fixation method (anchors or other devices). Some experts believe that a complete D-shaped ring offers greater stability than a semi-ring; however, current interventional fixation methods predominantly rely on anchors, which can easily cause myocardial injury. Furthermore, the continuous opening and closing motion of the mitral valve exerts traction, thereby compromising long-term efficacy.
2.2.3. Artificial Chordae Tendineae Implantation
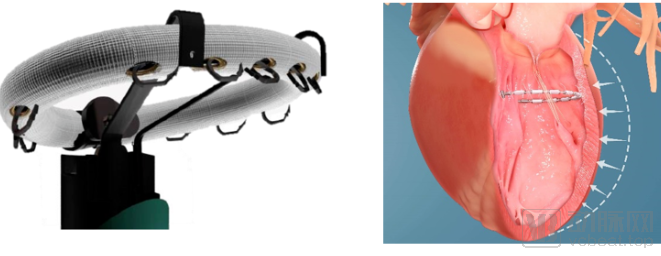
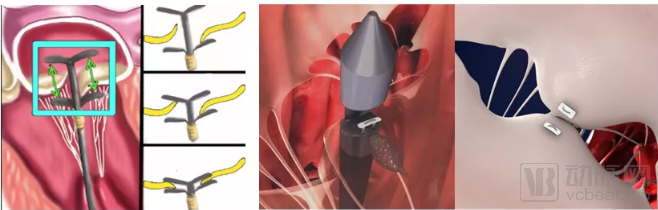
NeoChord Inc. – NeoChord: The NeoChord artificial chordae tendineae implantation system accesses the left ventricle via apical puncture, attaches artificial chordae to the prolapsed leaflet, and anchors them at the apex. It is indicated for patients with primary mitral regurgitation (MR) due to isolated posterior leaflet prolapse. According to currently published clinical results, the procedural success rate was 96.7%, the one-year overall survival rate was 98%, and patients experienced significant improvement in MR severity that was maintained at one year (Figure 18).[19] The system received CE marking in 2012 and remains in the clinical trial phase.
Figure 18: Schematic Diagram of the NeoChord Artificial Chordae Tendineae Implantation System and Clinical Trial Results
Source: Reference [19], Shengshan Asset
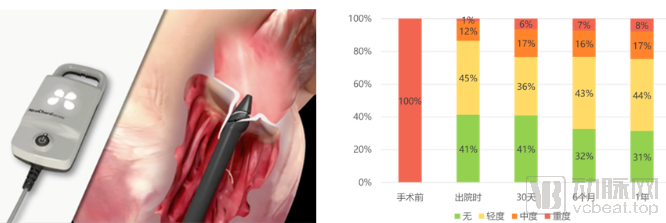
Edwards – Harpoon: The Harpoon artificial chordae tendineae implantation system was developed by Harpoon Medical and acquired by Edwards in December 2017 for $100 million. This system requires a small incision in the left thoracic wall to access the anterior wall of the left ventricle. Using a delivery system, the artificial chordae are positioned at the site of the prolapsed mitral valve. Guided by transesophageal echocardiography, the chordae are implanted and anchored at the apex while the heart is still beating. Clinical trials have demonstrated that this system can significantly improve mitral regurgitation (MR) (Figure 19).[20] Currently, this product remains in the clinical trial phase. While artificial chordae implantation technology offers a high safety profile, its indications are relatively limited; it yields favorable outcomes primarily for P2 segment prolapse of the posterior leaflet. Furthermore, data supporting its safety, efficacy, and long-term outcomes are still needed.
Figure 19: Schematic Diagram of the Harpoon Artificial Chordae Tendineae Implantation System and Clinical Trial Results
Source: Reference [20]
CardioMech – CardioMech Transcatheter Artificial Chordae Tendineae Implantation System: CardioMech is a medical device company based in Oslo, Norway, dedicated to the development of transcatheter artificial chordae tendineae replacement systems. The company’s transcatheter artificial chordae tendineae implantation system is designed to treat high-risk patients with severe, symptomatic degenerative mitral valve disease (caused by leaflet prolapse or flail). The target patient population in the United States and Europe is estimated at 440,000, representing a market size of up to $6 billion. Mr. Rick Nehm, Chairman and CEO of CardioMech, brings 20 years of commercial experience in medical devices for structural heart disease, having held leadership positions at Boston Scientific, Tendyne Holdings Inc. (acquired by Abbott), and ATS Medical (acquired by Medtronic). On August 12, 2019, CardioMech announced a $5 million financing round from MedTech, underscoring that the chordae repair device market is thriving and continues to attract investor attention.
2.2.4. Transcatheter Mitral Valve Implantation System
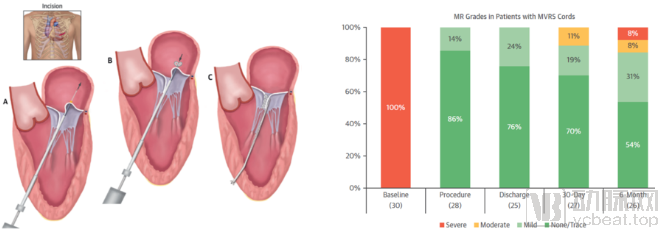
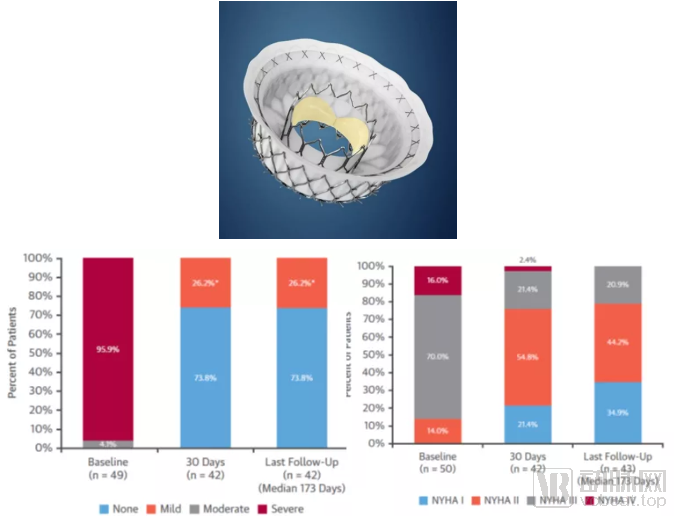
Abbott – Tendyne: The Tendyne TMVI system was initially developed by the medical device company Tendyne Holdings and was acquired by Abbott in September 2015 for $250 million. The system comprises a trileaflet valve, a self-expanding circular inner stent, a D-shaped outer stent, tethers, and an apical pad. In the latest published clinical trial data, the implantation success rate was 96%, the 30-day mortality rate was 6%, and the one-year all-cause mortality rate was 26%, with safety profiles within acceptable limits. Patients’ mitral regurgitation (MR) status improved significantly and was sustained for one year, cardiac function also showed marked improvement, indicating high device efficacy (Figure 20).[21] Tendyne currently appears to be a product with favorable clinical performance; its unique D-shaped design helps avoid left ventricular outflow tract obstruction; its retrievability facilitates adjustment of the implantation position; and fixation via apical tethers prevents displacement without damaging the leaflets or annulus. Although it has received CE marking, further clinical data are needed to evaluate and optimize its long-term efficacy.
Figure 20: Schematic Diagram of the Abbott Tendyne TMVI System (Top) and Clinical Trial Results (Bottom)
Source: Reference [21], Shengshan Asset
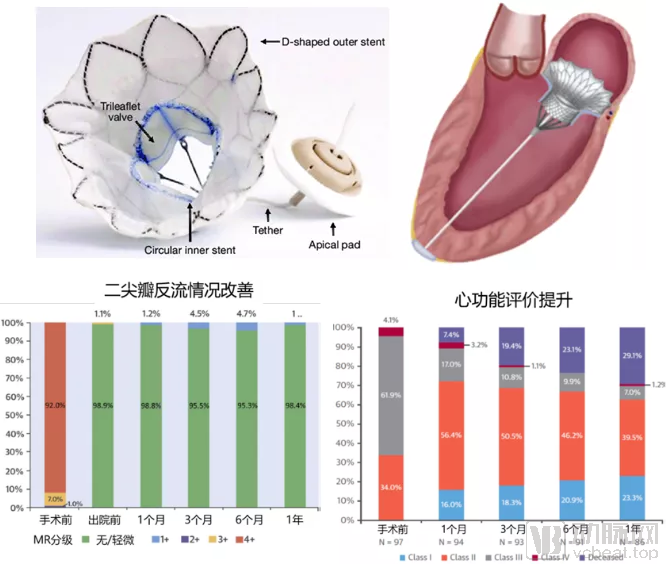
Medtronic – Intrepid: Developed by Twelve, a medical device company based in California, USA, the Intrepid is a transcatheter mitral valve replacement system delivered via transapical access. It features a circular design and self-expanding technology but is not retrievable. In October 2015, Medtronic acquired Twelve for $458 million. According to published results from early feasibility studies, the implantation success rate was 98%, with no device failures or thrombosis observed. The 30-day mortality rate was 14%, and the one-year survival rate was 76.5%. All patients achieved either no mitral regurgitation (MR) or mild MR post-procedure, with significant improvement in cardiac function (Figure 21).[22] Currently, Medtronic plans to conduct larger-scale clinical trials to further validate its safety and efficacy.
Figure 21: Schematic Diagram of the Medtronic Intrepid TMVI System (Top) and Clinical Trial Results (Bottom)
Source: Reference [22], Shengshan Assets
Edwards – CardiAQ: The CardiAQ, developed by CardiAQ Valve Technologies, is a circular, self-expanding mitral valve implantation system that is delivered transapically to the mitral valve and anchored below the annulus. In August 2015, Edwards acquired CardiAQ for $400 million and integrated its own TMVI product, FORTIS, with CardiAQ’s technology to develop a next-generation TMVI device. Early experimental results with CardiAQ were suboptimal, with a mortality rate as high as 50%. From March 2016 to February 2017, Edwards voluntarily suspended multiple clinical trials of CardiAQ. On February 21, 2017, the company announced that it had completed design verification testing and would resume patient screening and enrollment.
In addition to the three main products mentioned above, other TMVI devices are under development or in clinical trials, including Caisson (acquired by LivaNova for $160 million in May 2017) and Cephea (acquired by Abbott for $102 million in March 2019), among others (Figure 22). In recent years, major medical device companies such as Abbott, Medtronic, and Edwards Lifesciences have competed to acquire companies developing TMVR and TMVI technologies, further underscoring that the transcatheter mitral valve intervention market remains active and continues to attract significant attention.
Figure 22: Edwards CardiAQ (left), LivaNova Caisson (center), Abbott Cephea (right)

Sources: Edwards, LivaNova, public information, Shengshan Asset
2.3. Preliminary Success of Interventional Therapy Devices Independently Developed in China
Compared with North America and Europe, the research and development (R&D) of mitral valve interventional devices in China started relatively late. However, the R&D efforts have benefited from the close involvement of senior cardiology experts and have drawn on the experience gained from the development and clinical trials of various international products. It is believed that this field will experience rapid growth over the next decade. In the realm of repair, R&D and clinical trials are already underway for edge-to-edge repair and artificial chordae tendineae implantation devices. In the replacement sector, the unique structure and anatomical position of the mitral valve pose greater R&D challenges than those associated with transcatheter aortic valve implantation (TAVI) products. Drawing parallels with China’s TAVI industry, where products from Venus Medtech, Jiecheng Medical, and MicroPort CardioFlow have only recently been launched, the entire sector remains in its nascent stage. More market feedback and real-world data are needed to validate the performance of domestically developed valve replacement products. The clinical outcomes and sales performance of TAVI products will significantly influence market confidence in transcatheter mitral valve replacement (TMVR) products. Compared with foreign counterparts, Chinese-made valves still lag behind in terms of pericardial tissue quality and shelf life, which will also impact market preferences between imported and domestic products.
Shanghai Hanyu Medical – Edge-to-Edge Repair System ValveClamp: Established in December 2016, Shanghai Hanyu Medical is a medical device company focused on the field of valve repair. Its core product, ValveClamp (Figure 23, left), is the first domestically developed interventional device for mitral valves to achieve successful batch animal testing. It holds fully independent domestic patent rights and has applied for international PCT patents. The device was jointly developed by Academician Ge Junbo’s team from Zhongshan Hospital affiliated with Fudan University and Hanyu Medical. It represents an innovative and more user-friendly device system developed based on experience with the MitraClip. In July 2018, Academician Ge Junbo’s team performed the first repair procedure, followed by 12 cases of exploratory human clinical trials completed in October 2018, achieving a 100% success rate and 100% efficacy rate with no serious complications reported. The product was expected to be launched in 2021, becoming the first such minimally invasive interventional medical device for treating mitral regurgitation to be widely marketed in China and the second worldwide.
Hangzhou Dejin Medical – Artificial Chordae Tendineae Implantation plus Edge-to-Edge Repair System MitralStitch: Hangzhou Dejin Medical Technology Co., Ltd., established on August 3, 2015, is a brand under Deno Medical. Its developed MitralStitch repair system is the first transcatheter mitral valve repair product applied clinically in China (Figure 23, right). It can perform both isolated artificial chordae tendineae repair and edge-to-edge repair, making it suitable for both primary and secondary mitral regurgitation (MR). On January 19, 2018, Professor Pan Xiangbin’s team from Fuwai Hospital, Chinese Academy of Medical Sciences, together with Professor Meng Xu from Beijing Anzhen Hospital, successfully completed the world’s first clinical case. Ten clinical cases were completed in the first half of 2018. The product won the Second Prize in the 2018 China Medical Device Innovation and Entrepreneurship Competition and is expected to launch the MIRACLE II international multicenter clinical trial in 2019.
Figure 23: Schematic diagrams of ValveClamp (left) and MitralStitch (right)
Shanghai Nuomai Medical – Mi-thos Transcatheter Mitral Valve Implantation System: Shanghai Nuomai Medical Technology Co., Ltd. was established in March 2015 at MedValley PLUS in Pudong New Area, Shanghai. The company is positioned to develop and industrialize interventional artificial heart valve systems at an internationally advanced level. Its founder, Yu Qifeng, previously worked at MicroPort Medical and has many years of experience in the research and development of interventional heart valve products. Co-founder Qin Tao also served for many years as a cardiologist and Clinical Director at MicroPort Medical. The Mi-thos system is a transcatheter mitral valve implantation system delivered via the transapical approach. In May 2019, Professor Wang Chunsheng’s cardiac surgery team at Zhongshan Hospital Fudan University performed the first clinical procedure. The system is currently still in the clinical trial phase.
2.4. Imaging Devices for Interventional Therapy
An indispensable piece of equipment during mitral valve interventional procedures is the ultrasound diagnostic system, which generates two-dimensional color echocardiograms and real-time three-dimensional transesophageal echocardiograms to assist physicians in observing the morphology of the patient’s mitral valve, the severity of regurgitation, the delivery of interventional devices, and the procedural outcomes. One of the challenges in mitral valve interventional therapy is the inability to directly visualize the heart, as is possible in open-heart surgery. This limitation hinders the implementation of surgical techniques that yield favorable results in conventional surgery, such as suturing an annuloplasty ring onto the annulus (necessitating the use of anchors instead) and accurately suturing artificial chordae tendineae to the papillary muscles. These challenges demand that ultrasound diagnostic systems offer higher imaging quality and more specialized capabilities for rendering three-dimensional cardiac structures.
As demand for non-invasive diagnostics continues to rise, the ultrasound diagnostic market is experiencing rapid growth. In 2019, the global market size for medical ultrasound diagnostic equipment reached $7.4 billion, with a compound annual growth rate (CAGR) of 3.6%. In the same year, China’s ultrasound diagnostic equipment market reached RMB 9.1 billion. Driven by the release of pent-up demand, product upgrades, and continued policy support, the Chinese market has been growing at a faster pace than the global average.[23] Currently, the high-end ultrasound market in China remains dominated by foreign giants; however, domestic brands have been shifting from the low-to-mid-end segment toward the mid-to-high-end segment in recent years. We believe that with the increasing demand for transcatheter heart valve interventions, there remains significant room for growth in the high-end ultrasound market—particularly for cardiac-specific ultrasound systems—and domestic brands that achieve breakthroughs in key technologies will hold substantial potential.
Epidemiological statistics from both domestic and international sources reveal a large patient population with mitral regurgitation, accompanied by low diagnosis and treatment rates. With the aging of the population, the market potential for mitral regurgitation treatment is projected to reach hundreds of billions of yuan, far exceeding that of the aortic valve disease treatment market. Additionally, following the launch of MitraClip in China, conservative estimates suggest that terminal market sales could reach RMB 1 billion by 2025.
The etiology of mitral regurgitation is complex and heterogeneous, with a prolonged disease course. Extensive screening, timely diagnosis, and early intervention hold promise for preventing disease progression and deterioration, thereby improving the quality of life and extending life expectancy in patients with mild regurgitation. For patients with severe regurgitation, surgical repair or replacement should be pursued as much as possible, provided safety is assured, to reduce the incidence of acute cardiovascular events such as myocardial infarction and stroke, and to lower mortality rates. Currently, patients undergoing mitral valve surgery remain primarily a small subset of those with severe, symptomatic disease who are suitable for open-heart surgery. The large number of untreated patients also indicates significant market potential.
Currently, surgical repair and replacement remain central to the treatment of mitral valve disease. Mitral valve repair offers relatively high safety and efficacy; however, traditional open-heart surgery imposes stringent requirements on patients’ physical condition, resulting in low penetration rates for mitral valve procedures. The promotion of minimally invasive techniques is expected to improve patient acceptance of mitral valve surgery, while interventional therapies with broader indications and less invasiveness will become the future trend.
Transcatheter repair techniques have significant room for development. They offer higher efficacy than pharmacological therapy, less invasiveness than surgical intervention, and lower risk compared to valve replacement. Mitral valve repair is not a “one-size-fits-all” approach; different types of repairs are required for different patient profiles. Artificial chordae tendineae implantation is indicated only for patients with primary posterior leaflet prolapse and chordal rupture, thus having limited indications. Edge-to-edge repair is effective for bileaflet prolapse, applicable to both primary and secondary cases, and offers high safety but limited long-term durability. Annuloplasty is primarily used for secondary mitral regurgitation (MR) but can also be combined with leaflet repair to stabilize the annulus. Therefore, combined repair techniques (Transcatheter COMBO MV therapies) may represent a new breakthrough in future mitral valve repair technologies.
Furthermore, while focusing on interventional devices for the mitral valve, attention should also be paid to technological breakthroughs and advancements in related equipment such as ultrasound systems. Compared with high-value consumables that are dedicated to specific organs, specific pathologies, and patient populations with specific indications, imaging medical devices offer broader applicability, as they can be used for diagnosis, prevention, and interventional procedures.
Not long ago, on June 15, Abbott’s MitraClip received approval from the National Medical Products Administration (NMPA) without the requirement for additional clinical trials, leveraging its robust overseas clinical data, and was officially launched in the Chinese market. This demonstrates that not only are technology and products advancing, but China’s regulatory review system is also becoming increasingly standardized, progressive, and aligned with international standards. In recent years, through the continuous efforts of clinical experts and engineers in China and around the world, challenges in the field of mitral valve intervention have been gradually overcome. Just as the famous “two clouds” hanging over the edifice of classical physics led to the development of the globally renowned theories of relativity and quantum mechanics, we believe that the cloud currently hovering over the field of interventional medicine will soon dissipate, giving rise to a series of exceptional technologies and products that benefit patients.
Appendix 1: Products Currently Certified by CE and FDA
Appendix Table 2: Mitral Valve Repair and Implantation Products in China

Appendix Table 3: M&A Transactions in the Field of Mitral Valve Repair and Replacement
