Three Core Objectives of Hospital Lean Management and Implementation Strategies
By Wang Wenxin
Refined management is hardly a novel concept for hospitals. The requirements of the new healthcare reform policies have driven a gradual shift in hospital management models from extensive to refined approaches, while the impact of the COVID-19 pandemic has further underscored the importance of refined management. However, for hospitals—organizations that are simultaneously capital-intensive, labor-intensive, and knowledge-intensive—the implementation of refined management is by no means an easy task. Against the backdrop of refined management in hospitals, this article will explore its practical implementation by examining its objectives and challenges, drawing on exemplary practices from selected hospitals.
In recent years, the new healthcare reform has gained significant momentum, with frequent national policy releases and increasingly stringent requirements for hospitals. Not long ago, the General Office of the National Health Commission issued a Notice on Further Improving the Appointment-Based Diagnosis and Treatment System and Strengthening the Construction of Smart Hospitals, which explicitly stated that “smart management” should be leveraged to further enhance the level of refined hospital management. Secondary and tertiary hospitals should adopt a problem- and demand-oriented approach, design the architectural framework for smart hospital management systems, and establish hospital operation and management platforms capable of supporting business operations, performance evaluation, financial management, cost accounting, logistics and energy consumption monitoring, and integrity risk prevention and control. In response to these policy mandates, hospitals must implement refined management to achieve the goals of “high quality, high efficiency, and low consumption,” establishing a patient-centered “humanistic” service model and a “knowledge-based” refined management model centered on standardized medical quality and technological innovation in healthcare.
On the other hand, affected by the pandemic, the number of non-fever patients in hospitals has dropped significantly. The operational pressure caused by several months of downtime and a decline in patient visits will still take considerable time to absorb. According to the national medical service statistics for March 2020 released by the Statistical Information Center of the National Health Commission, the number of diagnoses and treatments at medical and health institutions across China decreased by 33.1% year-on-year, while the number of discharges dropped by 32.0% year-on-year. It can be said that hospitals will face an extended period of “austerity” this year. Against this backdrop, many hospitals have begun to seek transformation, aiming to improve efficiency through better management and services, with a focus on enhancing efficiency, improving quality, and reducing costs.
Refined management refers to the systematic and detailed implementation of rules, leveraging procedural, standardized, data-driven, and information-based approaches to ensure that all organizational units operate with precision, efficiency, synergy, and sustainability. Compared with other industries, hospitals possess a solid foundation in terms of proceduralization, standardization, and informatization. Therefore, the core of refined hospital management centers on data utilization, aiming to achieve at least three objectives: data-informed decision-making, orderly operations, and high efficiency coupled with high quality. However, given the current state of hospitals, numerous problems and challenges remain.
1. Data-Driven Decision-Making
Data serves as the core foundation for refined management. Under traditional extensive management models, corporate decisions often rely on subjective judgments based on experience. While experience-based decision-making is not entirely devoid of value, it tends to expose enterprises to greater risks. In contrast, data-driven managerial decision-making requires leaders to make decisions based on operational data, thereby enabling control over various organizational processes. This approach offers advantages such as objectivity, universality, and comprehensiveness. Furthermore, post-decision outcomes can feed back into business data, forming a true closed-loop management system.
However, the complex and diverse diagnosis and treatment processes have given rise to a multitude of hospital information systems and data dimensions, increasing the difficulty of data management and utilization. Each data item—such as patients, symptoms, doctors, departments, diagnostic and therapeutic procedures, medical equipment, and billing items—carries a large number of dimensions. Coupled with the distinction between structured and unstructured data, management becomes extremely challenging. Moreover, most hospital information systems operate independently, and the problem of data silos results in very low utilization of these data, failing to support the hospital’s operational management objectives.
2. Orderly Operation
Hospital operational management primarily comprises three core modules: personnel, finance, and materials. Based on data-driven decision-making, refined hospital management aims to ensure the orderly operation of these modules. The key to such orderly operation lies in leveraging data flow to track and trace various nodes and processes, thereby standardizing, making visible, and enabling control over the entire spectrum of hospital operations. For instance, in the procurement, approval, and utilization of medical supplies, data tracking of these processes can prevent irregular requisitions and claims, as well as resource wastage. In this way, refined management achieves rapid identification of and timely intervention in critical links by integrating data chains and management chains across all modules, thus safeguarding managerial order.
In terms of operational efficiency, the primary challenge hospitals face is that their data architecture fails to meet actual needs. Many hospitals lack adequate computational power and acceleration capabilities in their data infrastructure, resulting in significantly lagging data retrieval speeds. Reliance on manual collection, aggregation, and statistical analysis consumes substantial human resources and is prone to errors, severely undermining the orderly operation of hospitals.
3. High Efficiency and Quality
The ultimate goal of refined hospital management is to achieve high-efficiency and high-quality operations. To meet the demands of high efficiency and quality, hospitals must align with their development strategies, coordinate efforts, and leverage tools such as goal-oriented leadership, budgetary control, and performance appraisal to mobilize the enthusiasm of the entire institution. This approach aims to minimize inefficient work and resource waste, transform orderly processes into highly efficient and well-organized workflows, elevate decision-making to a level of high efficiency and quality, and ensure that human, financial, and material resources are optimally aligned.
However, issues such as ineffective and redundant communication in hospitals have led to substantial communication costs, while the difficulty in aligning hospital-wide operational management has compromised the quality of hospital operations. First, ineffective communication is a manifestation of low data utilization; without data-driven evidence, communications rely merely on subjective judgments and empty rhetoric, resulting in an inability to reach consensus. Second, although hospitals have established standardized communication systems and processes, the lack of data transparency, tracking, and feedback during implementation leads to redundant communication and consequently increased communication costs. Furthermore, hospitals comprise numerous departments with complex interdependencies; a single data metric often involves multiple departments, and varying levels of understanding of other departments’ operations further exacerbate the challenges of aligning hospital-wide operational management. For hospitals with multiple campuses, the challenge of achieving homogeneous management across sites is even greater.
Refined management that fails to be implemented is merely empty talk. We believe that hospitals can advance refined management by focusing on four key areas: data infrastructure, compliant operations, quality control, and economic efficiency, leveraging digital tools and various analytical models to ensure practical implementation.
1. Build two major data centers and one data platform to standardize refined management of data
Most hospitals have established Clinical Data Repositories (CDR); however, a CDR alone is insufficient for refined management. To ensure that hospitals can grasp the overall status of their economic operations, and in accordance with the hospital’s overall development plan, various functional departments must collaborate effectively to establish a unified Operational Data Repository (ODR). This involves creating standardized basic data dictionaries for departments, personnel information, charge items, charge categories, material names, and other key elements, thereby regulating data exchange and ensuring consistency in accounting subjects and statistical indicators. Such measures provide data support for the effectiveness of refined economic management and the rationality of decision-making.
Building upon the two major data centers, a refined management data integration platform will be established to collect and integrate data from the accounting system, human resources system, budget management system, cost accounting system, logistics management system, performance management system, fixed asset management system, cost management system, electronic medical records (EMR), Hospital Information System (HIS), Picture Archiving and Communication System (PACS), and Laboratory Information System (LIS), thereby achieving a standardized data management model.
As illustrated in the data application architecture diagram, a data center—comprising the Clinical Data Repository (CDR) and Operational Data Repository (ODR), and incorporating regionally shared data—is first established on the foundation of the hospital’s major business systems. Subsequently, a data platform is built upon this data center to develop tailored data applications for different user groups, thereby meeting the hospital’s comprehensive data needs.
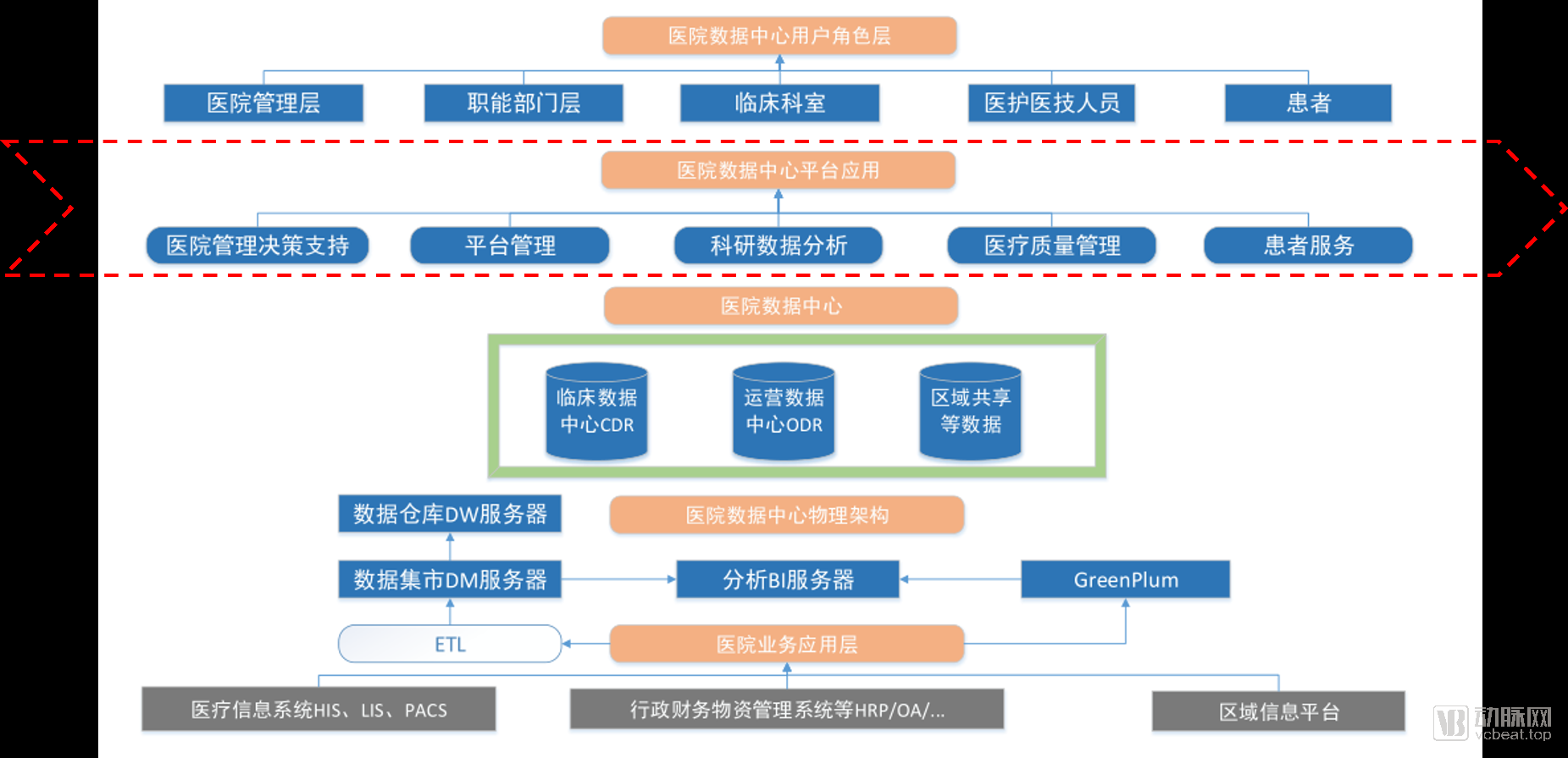 Data Application Architecture of a Hospital
Data Application Architecture of a Hospital
2. Dynamically monitor national regulatory indicators to ensure compliant hospital operations
For hospitals, especially public ones, compliance is always the top priority. To ensure compliant hospital operations, the national government has established a wide range of regulatory indicators based on hospital accreditation standards. Taking the “Accreditation Standards for Tertiary General Hospitals (2011 Edition)” issued by the Ministry of Health as an example, a total of 391 standards and monitoring indicators were established, covering seven major categories of routine statistical evaluation metrics, including hospital operations, antimicrobial drug use, healthcare-associated infection control, single-disease quality control, and infectious disease control, so as to strengthen daily monitoring of medical care quality in hospitals. Meanwhile, to adapt to healthcare reform policies, hospital development needs, and regional differences, national regulatory indicators are in a state of continuous evolution.
Under national regulatory requirements, hospitals must, on the one hand, establish standardized and implementable indicator systems centered on national regulatory metrics by clearly defining their meanings, data sources, hierarchical dimensions (including organizational structure, time, and regulatory dimensions), and calculation methods. On the other hand, to accommodate dynamic changes in these indicators, hospitals must also plan for their maintainability and scalability, enabling dynamic adjustments and monitoring to ensure compliant operations.
3. Patient-Centered Care: Comprehensive Control of Medical Quality
Medical quality is the “lifeline” of hospital operations, and medical quality management constitutes a core component of hospital administration. It not only impacts patients’ lives and health but also serves as a primary indicator of a hospital’s strength, competence, and reputation. From the perspective of macro-level hospital management, the control of medical quality can be divided into three stages: foundational quality management, process quality management, and outcome quality management, corresponding to pre-event, in-process, and post-event controls, respectively.
(1) Basic Quality Management
Basic quality constitutes the fundamental elements of medical service quality, primarily encompassing the professional competence of healthcare personnel and foundational safeguards such as medical supplies and equipment. This includes, for example, the medical knowledge, professional ethics, and service attitude of healthcare providers; the adequacy of supply guarantees for pharmaceuticals, reagents, and disposable consumables; the functional coverage of diagnostic and therapeutic equipment and medical devices; and the standardization and accuracy of medical documentation. Basic quality management requires hospitals to leverage data to comprehensively monitor resources such as manpower and materials, thereby ensuring medical quality at its source.
 Pharmacy Management Module of a Hospital
Pharmacy Management Module of a Hospital
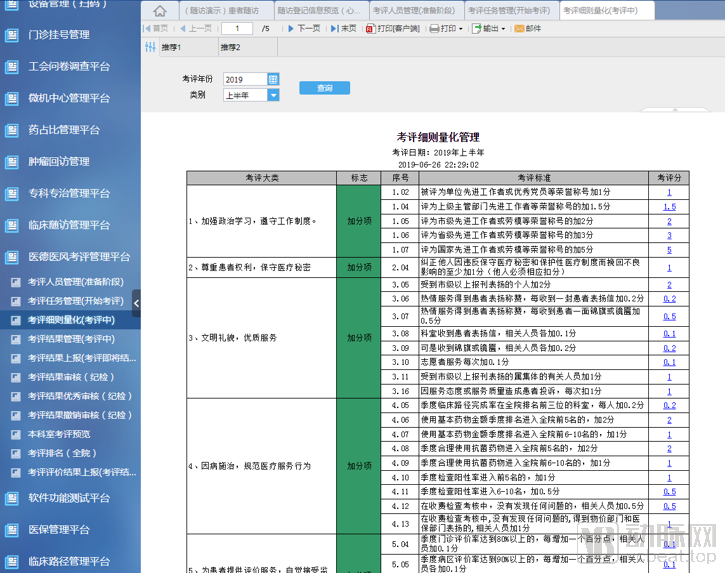
Medical Ethics and Professional Conduct Evaluation Management Platform of a Certain Hospital
(2) Process Quality Management
As the name suggests, process quality refers to the quality of each stage within medical practice, also known as “process quality” or “operational quality.” Process quality directly impacts final healthcare outcomes and represents the most critical component of medical quality control. From the perspective of the entire healthcare service workflow, process quality management can be divided into stages such as consultation, admission, diagnosis, treatment, and discharge.
Among these, the primary objectives of stages such as outpatient visits, hospital admission, and discharge are to leverage data to monitor the overall status of each stage and optimize operational processes, thereby enhancing patient satisfaction. For instance, during the outpatient visit stage, hospitals can reasonably schedule physician shifts by monitoring and predicting outpatient traffic data, and optimize the floor locations of outpatient and medical technology departments based on inter-departmental correlations and foot traffic data, thus shortening patient waiting times and improving consultation efficiency. Additionally, outpatient management departments can track real-time outpatient conditions via monitoring dashboards to enable timely interventions. The same principles apply to the hospital admission and discharge stages.
 Outpatient Monitoring Dashboard of a Hospital
Outpatient Monitoring Dashboard of a Hospital
Diagnosis and treatment are the top priorities in process quality management. During the diagnostic phase, the core focus is on the quality of clinical processes, including consultations and the management of critically ill patients. Among these, the accurate identification and assessment of critical conditions are the primary responsibilities of clinical nursing, while the treatment outcomes for critically ill patients also reflect the overall competence of the hospital. For instance, one hospital designed information reports specifically for critically ill patients, allowing detailed patient and treatment information to be viewed by simply clicking on the admission number, thereby ensuring medical quality control and preventing medical errors. Similarly, for patients requiring consultations, clicking on the admission number enables access to their historical medical records, facilitating information retrieval and collaborative care. During the treatment phase, hospitals must also prioritize medical safety issues throughout the treatment process, such as common adverse events like pressure ulcers.
(3) Terminal Quality Management
Terminal quality refers to the final outcomes achieved by patients after undergoing the entire healthcare service process, serving as a concrete manifestation of medical quality and effectiveness. The key aspects of terminal quality management lie in conducting scientific analyses based on case records and disease units, integrating statistical indicators such as the concordance rate between admission and discharge diagnoses, average length of stay, cure rate, mortality rate, and infection rate, along with patient feedback. This approach facilitates the continuous summarization of lessons learned from the care process, identification of issues for improvement, optimization of workflows, and promotion of a cyclical enhancement in medical quality.
4. Leveraging Medical Insurance DRGs to Enhance Hospital Economic Efficiency
Building on the foundation of medical quality management, hospitals’ refined management should also focus on operational aspects. By leveraging the Diagnosis-Related Groups (DRGs) tool and centering on human resources, financial capital, and material assets, hospitals can establish a refined operational model to reduce costs, improve efficiency, and enhance economic performance.
(1) Human
Human resources are the core assets of a hospital. Refined management of personnel can be approached through organizational structure analysis, performance analysis, and efficiency and effectiveness analysis.
Organizational composition analysis can reflect the number and proportional structure of hospital staff, authorized versus actually occupied beds, and the workload of clinical and medical technology departments, thereby measuring the scale of resource input in hospitals.
Performance analysis can be approached through the Resource-Based Relative Value Scale (RBRVS). RBRVS is a method for compensating physicians’ professional services based on resource consumption and measured by relative value, enabling an objective assessment of costs according to the resource expenses incurred by physicians in delivering medical services. Guided by the principles of RBRVS, performance analysis is built upon financial management, reflecting the overall outcomes of refined hospital economic operations through the establishment of financial and performance evaluation indicators, thereby embodying an information-driven decision-making mechanism for hospital economic management. Specifically, performance analysis can be designed from the perspectives of managerial decision-making and performance orientation, encompassing performance management, financial reporting, performance ranking, key performance indicators (KPIs), and break-even analysis.
Finally, an efficiency and benefit analysis is presented, focusing on per capita workload, as well as the revenue contribution from inpatient and outpatient/emergency services. This reflects the operational efficiency and revenue-generating capacity of hospital personnel and assets (equipment and beds), while also demonstrating the overall economic efficiency and effectiveness of hospital operations.
(2) Wealth
Hospital financial management is divided into two aspects: revenue and costs.
From a revenue perspective, medical insurance reimbursements constitute a major source of income for hospitals; however, the reimbursement model has long been a challenging issue for both hospitals and healthcare administrative authorities. To better control medical costs and enhance the quality and efficiency of hospital services, China has begun promoting the Diagnosis-Related Groups (DRGs) payment model.
Diagnosis-Related Groups (DRGs) constitute a management system that categorizes patients into distinct diagnostic groups (DRG groups) based on factors such as age, disease diagnosis, comorbidities, complications, treatment modalities, severity of illness, and clinical outcomes. For hospitals, DRGs enhance operational efficiency, increase revenue for both institutions and physicians, and serve as a strategic entry point for refined hospital management. Fixed reimbursement standards for specific conditions compel hospitals to continuously optimize diagnostic and therapeutic protocols within cost constraints, thereby improving medical efficiency and reducing the average length of stay for patients.
As a result, medical resources have been utilized more fully, leading to an increase in revenue for hospitals and physicians. According to data from VCBeat, the number of discharged patients at a certain hospital increased from 25,000 before the implementation of Diagnosis-Related Groups (DRGs) to 31,000 after implementation. The annual revenue from medical services rose rapidly from RMB 92 million prior to DRG implementation to RMB 159 million thereafter, significantly higher than that of control group hospitals that had not implemented DRGs.
Therefore, supported by national policies and validated by practical outcomes, DRG-based payment will become an effective approach for hospitals to increase revenue and implement refined operational management. On this basis, hospitals can leverage models such as activity-based costing (ABC) analysis to reflect their operational performance. First, hospital economic data should be consolidated to generate the required financial statements. Second, based on this consolidation and reporting, an analysis of the hospital’s current status should be conducted, with drill-down traceability to identify the root causes of operational challenges. Comparative analyses should be performed across departments of similar types and characteristics to foster a mechanism of healthy competition among them.
From the perspective of hospital costs, this primarily includes budget management, cost analysis, and analysis of cost management capabilities.
First, the foundation for strict cost control lies in reasonable budget formulation. For instance, a private hospital group replaced its traditional, coarse-grained cost accounting method—which allocated costs solely based on headcount and revenue ratios—with a refined approach to cost accounting and budget management. By leveraging actual departmental costs, more than 20 allocation factors, and multiple dimensions, the group established a multi-level, precise cost allocation model capable of breaking down costs to the department and project levels. Furthermore, by conducting budget execution analysis to monitor progress and identify causes of variances, the group was able to strictly control overall costs and reduce controllable expenses.
Additionally, cost analysis involves the statistical categorization of hospital costs and expenses by department, reflecting the scale of hospital expenditures, growth trends, and the composition of medical technology spending. It also enables the prediction of cost scale and structure based on revenue matching, thereby providing a basis for decision-making to control the total scale of hospital expenditures.
Finally, the analysis of cost management capability is used to reflect the cost level incurred per unit of outpatient and inpatient revenue in hospitals.
(3) Objects
Regarding material management, the primary focus includes fixed asset analysis, benefit analysis of large-scale equipment, and analyses related to material requisition.
Fixed Asset Analysis reflects the hospital's asset utilization efficiency, asset procurement distribution, and disposal status. It includes analysis of total assets, asset distribution, asset disposal, asset procurement, and accounts payable.
Benefit Analysis of Large-Scale EquipmentThe benefit analysis of large-scale equipment implements classified management and analysis of state-owned assets in accordance with the configuration standard system, categorizing fixed assets into Class A large medical equipment, Class B large medical equipment, buildings and structures, intangible assets, and other categories. This approach fulfills regulatory functions—including approval and feasibility demonstration, assessment and testing, risk monitoring, and benefit analysis—thereby ensuring the preservation and appreciation of state-owned assets.
Material Requisition Analysis involves the classified statistical analysis of all materials within the hospital’s operational scope, providing a multi-dimensional, visualized assessment of hospital material management and supply chain management. This process identifies areas for improvement and offers recommendations, while integrating financial analysis and economic operation analysis to propose strategies for enhancing the rational consumption and utilization efficiency of administrative and management departments. Specific components include inventory material analysis, material consumption analysis, specialized analysis, high-value consumables analysis, material procurement analysis, and accounts payable analysis.