National Tertiary Public Hospital Performance Assessment Unveils Six Healthcare Reform Achievements—What’s Next?
On July 1, 2020, the Bureau of Medical Administration and Medical Services issued the “Circular from the General Office of the National Health Commission on the National Monitoring and Analysis of the 2018 Performance Appraisal of Tertiary Public Hospitals Nationwide,” marking the final release of the unified performance appraisal results for tertiary public hospitals, a matter of significant concern to the healthcare industry.
In terms of significance, this performance assessment is effectively the first “college entrance examination” for tertiary public hospitals since the founding of the People’s Republic of China. The assessment results will serve as a critical basis for public hospital development planning, approval of major projects, fiscal investment, fund allocation, determination of total performance-based wage bills, adjustment of medical insurance policies, and tertiary hospital reaccreditation. They will also constitute an important reference for the selection and appointment of leadership personnel in public hospitals.
By the end of 2018, a total of 2,398 tertiary public hospitals in China (including 1,289 general hospitals, 576 specialized hospitals, and 533 traditional Chinese medicine hospitals) participated in the 2018 annual performance assessment. The big data aggregation, computation, and analysis for this performance assessment even leveraged the Tianhe-2 supercomputer at the National Supercomputing Center in Guangzhou.
The results showed that, among all hospitals participating in the assessment, the National Health Commission conducted collective interviews with 141 tertiary hospitals and deducted corresponding performance evaluation points. In addition, three hospitals did not participate in the annual assessment due to new construction or relocation.
Meanwhile, a new round of performance assessments for public hospitals was launched in June this year, with both secondary and tertiary hospitals included in the new framework. Although the number of assessment indicators for secondary hospitals has been significantly reduced compared to those for tertiary hospitals (28 items for secondary hospitals versus 55 for tertiary hospitals), the new assessment introduces new quantitative metric requirements. Given that these metrics are linked to factors such as hospital funding and total wage bills, secondary hospitals are compelled to accelerate their development. This sufficiently demonstrates the National Health Commission’s determination to promote the development of lower-tier hospitals.
Returning to policy, what signals will be revealed during the transition between the old and new hospital performance evaluation systems? VCBeat raises three considerations:
1. What healthcare reform trends did the 2018 performance evaluation reflect?
2. Driven by numerous informatization policies and new infrastructure initiatives, what trends will the performance appraisal system for the coming year promote?
3. The enhancement of hospitals’ foundational capabilities relies on corporate support; under the new metrics, what kind of market opportunities will emerge for enterprises?
Although the performance rankings released this time are based on 2018 annual data, by combining them with the trends from 2016 and 2017, we can more easily infer the development status of various aspects of China’s hospital system as well as future development trends, thereby facilitating decision-making for the next phase.
First, let us review the six major achievements highlighted in the official performance assessment results released by the National Health Commission: (1) implementation of functional positioning; (2) improvement in medical quality and safety; (3) enhancement of hospital operational efficiency and internal management; (4) gradual strengthening of mechanisms for sustainable development; (5) increased patient satisfaction; and (6) prominent role played by hospitals directly affiliated with or administered by the Commission as the national team. In this regard, VCBeat has conducted a focused extraction and analysis of the data provided by the National Health Commission.
I. Functional Positioning Direction
1. Efficiency of Medical Services: In 2018, the total number of outpatient and emergency visits at tertiary public hospitals across China reached 1.36 billion, representing a 9.93% increase compared to 2016. The average length of stay was 9.1 days, a decrease of 0.4 days from 2016, while the bed occupancy rate stood at 99%, with the time consumption index declining year by year. Compared with 2016, the number of day-surgery patients increased by nearly 740,000, and the proportion of day surgeries among elective surgeries rose by 2.93 percentage points.
2. Tiered Diagnosis and Treatment: In 2018, the cumulative number of patients referred downward to secondary hospitals or primary healthcare institutions within medical consortiums reached 13.0173 million, representing a 45.45% increase compared with 2016, thereby gradually demonstrating the effectiveness of the tiered diagnosis and treatment system.
3. Capacity for the treatment of complex and critically ill patients; in 2018, the proportion of surgical procedures among discharged patients in tertiary public hospitals nationwide was 27.4%, with minimally invasive surgeries accounting for 15.9% and Level 4 surgeries comprising 16.4%, all representing increases compared to 2016, thereby demonstrating the continuous enhancement of comprehensive diagnostic and therapeutic technical capabilities in tertiary public hospitals.
Functional positioning primarily reflects the basic medical care capabilities of China’s tertiary public hospitals. As the data show, improvements in economic capacity and medical efficiency have driven an increase in total patient visits, while a decline in the average length of stay indicates advancements in the nation’s healthcare standards. Furthermore, the functional differentiation among various medical institutions and clinical departments has become increasingly clear. The tiered diagnosis and treatment system had already shown initial results by 2018, and with the ongoing improvement in primary care services, this system is poised for further advancement.
II. Medical Quality and Safety
1. Patient Safety: In 2018, the incidence of complications among surgical patients in tertiary public hospitals across China was 0.48%, and the rate of surgical site infections in Class I incisions was 0.71%, both showing a decline compared to 2016.
2. Medical Service Capacity: Over the past three years, the technical complexity of medical services provided by tertiary public hospitals across China has shown a steady increase. The Case Mix Index (CMI) for general hospitals rose from 1.015 in 2016 to 1.016 in 2018. The coverage of diagnosed and treated conditions in tertiary public hospitals nationwide has expanded year by year, with the median number of Diagnosis-Related Group (DRG) categories increasing from 530 in 2016 to 563 in 2018. Among these, the median number of DRG categories for general hospitals reached 617, an increase of 28 groups compared to 2016.
3. Comparability of Clinical Laboratory Tests: Over the past three years, the number of tertiary public hospitals participating in external quality assessment (EQA) has increased from 1,394 to 1,527. In 2018, the median participation rate for national EQA programs was 75%, representing a 3.4 percentage point increase compared with 2016, while the median pass rate remained stable at approximately 96%. These findings indicate improved comparability of laboratory test results among healthcare institutions of the same level, laying the foundation for mutual recognition of test results.
4. Rationality of Clinical Medication: In 2018, the intensity of antimicrobial use in tertiary public hospitals nationwide was approximately 37.78 DDDs, surpassing the national requirement of 40 DDDs. The proportion of reviewed prescriptions out of the total number of prescriptions, the review rate of ward (area) medication orders (prescriptions), and the number and proportion of essential medicines procured have increased year by year. The proportion of outpatient prescriptions for essential medicines reached 52.25%, the utilization rate of essential medicines among inpatients reached 95.38%, and the usage proportion of drugs awarded in the national centralized drug procurement reached 92.21%.
With the iteration of medical technology, patients will inevitably benefit from safer diagnostic and therapeutic capabilities, the ability to perform more complex surgical procedures, and more rational clinical medication practices. Notably, as significant reforms emerge in the field of Diagnosis-Related Groups (DRG), the China Healthcare Security DRG (CHS-DRG) system is trending toward standardization, with 618 core groups delineated. This will further enhance the controllability of patients’ treatment costs and healthcare insurance expenditures.
Also addressing the payment issue is the implementation of the 2018 centralized procurement policy. As centralized procurement expands to cover more areas, the proportion of winning bids from the national organized drug centralized procurement announced in 2018 will further increase.
III. Hospital Operations and Internal Management Level
1. Internal Management Capabilities: In 2018, the outpatient appointment rate for tertiary public hospitals nationwide reached 42.02%, an increase of 12.36% compared to 2016. Over the three-year period, the number of tertiary public hospitals participating in the Electronic Medical Record (EMR) functional grading evaluation rose from 994 to 1,764, with a participation rate of 94.58%. The national average EMR grade increased from 2.22 to 2.72. In 2018, the positive rate for examinations using large-scale medical equipment reached 83.26%, representing a 2.25 percentage point increase from 2016.
2. Growth in Medical Expenses: Compared with 2016, the average outpatient and inpatient costs per visit at tertiary public hospitals nationwide increased in 2018 (by 9.36% and 6.03%, respectively). The growth rate slowed down and was lower than the GDP growth rate for the same year. Meanwhile, the average pharmaceutical costs per inpatient stay and per outpatient visit decreased (by 15.25% and 3.38%, respectively), reflecting an overall stable trend in the growth of medical expenses at tertiary public hospitals and effective control over unreasonable cost increases.
3. Revenue and Expenditure Structure: The revenue and expenditure structure of tertiary public hospitals has shown a trend of “three increases and three decreases.” On the one hand, the proportion of medical service income (excluding income from drugs, consumables, and examination and testing) in total medical income, the proportion of personnel expenditures in operational expenditures, and the balance of revenue and expenditure have steadily increased (see Figures 1 to 3 for specific data). The revenue structure has been continuously optimized, the value of medical staff’s labor has been further reflected, their income has gradually improved, and the overall operational efficiency of hospitals has steadily enhanced, indicating that the structural adjustment strategy of “replacing old with new” has begun to yield results. On the other hand, energy consumption expenditure per ten thousand yuan of income (see Figure 4), the asset-liability ratio (see Figure 5), and the proportion of income from adjuvant medications have steadily decreased.
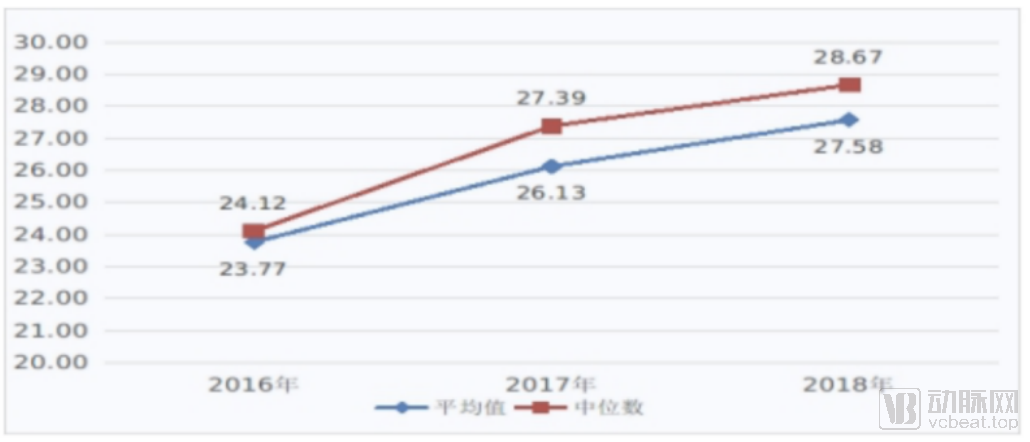
Figure 1: Proportion (%) of Medical Service Revenue (Excluding Revenue from Drugs, Consumables, and Laboratory Tests) in Total Medical Revenue, 2016–2018
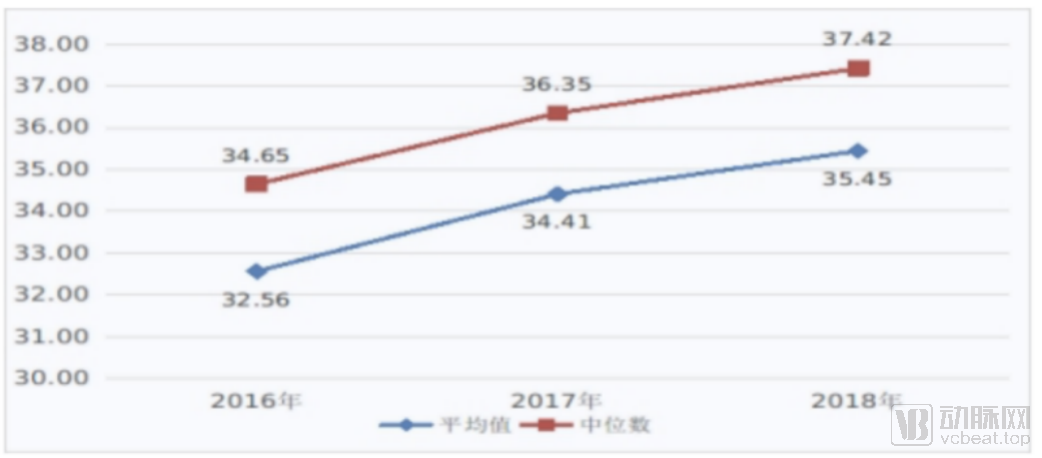
Figure 2 Proportion of Personnel Expenditures in Operating Expenditures, 2016–2018 (%) Figure 3 Surplus of Operating Revenues over Expenditures, 2016–2018 (RMB 10,000)
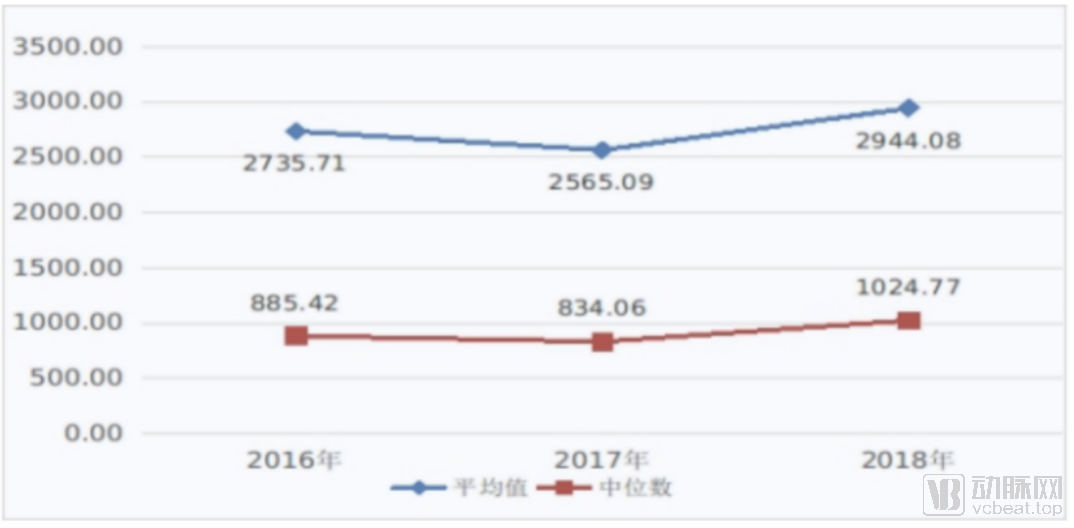
Figure 3. Business Income and Expenditure Balance (2016–2018) (in 10,000 Yuan)
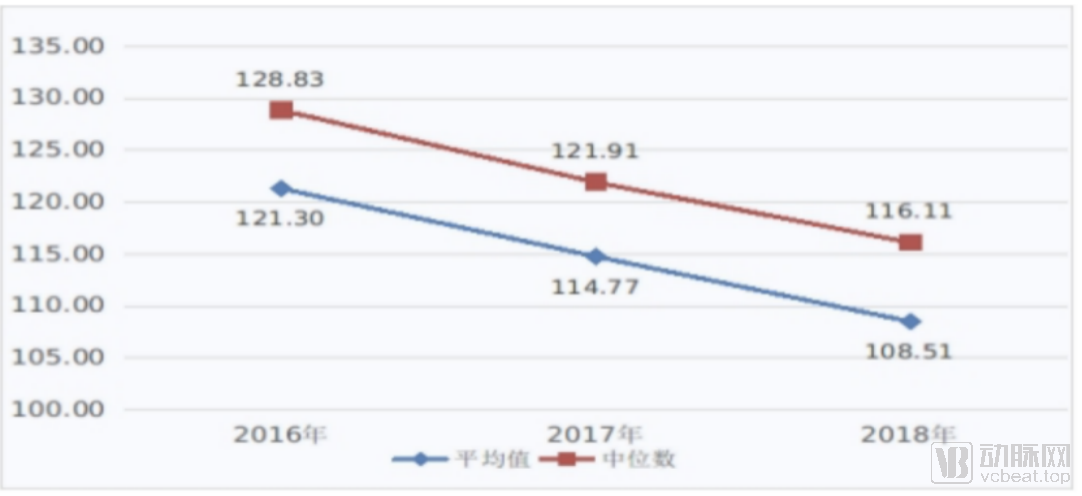 Figure 4 Energy Consumption Expenditure per 10,000 Yuan of Revenue (Yuan), 2016–2018
Figure 4 Energy Consumption Expenditure per 10,000 Yuan of Revenue (Yuan), 2016–2018
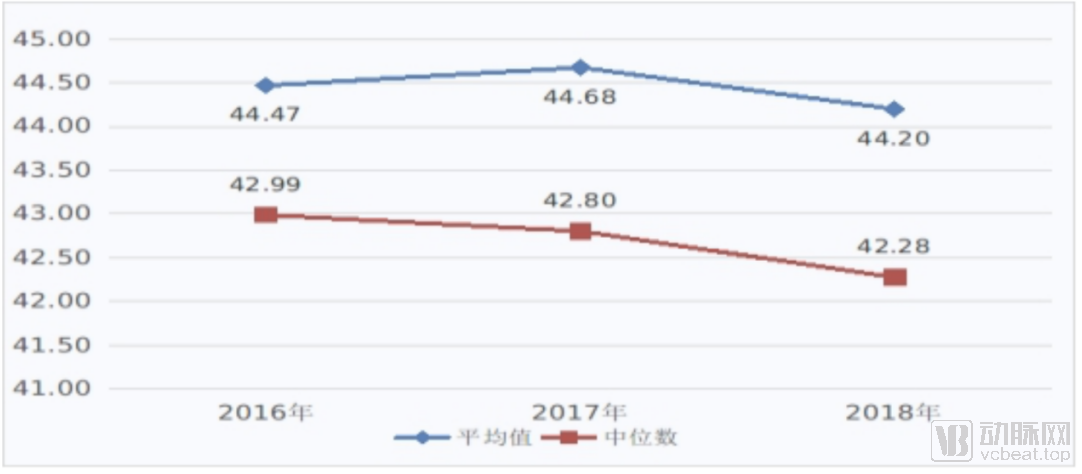
Figure 5 Asset-liability ratio (%), 2016–2018
Let us first discuss the level of informatization. Since the data were collected in 2018, and given that electronic medical record (EMR) grading and interoperability certification became mandatory performance indicators for public hospitals in 2019, it is inevitable that more hospitals have participated in EMR grading assessments. Therefore, based on the 94.58% participation rate in 2018, this figure is now approaching 1.
In terms of revenue structure, we observe that hospital medical service revenue, income of medical service personnel, and GDP growth have increased in the same direction at roughly proportional rates. This indicates that while the hospital’s revenue structure has undergone certain changes, the income model for medical service personnel remains unchanged. However, with the advancement of policies over the past two years—such as centralized drug procurement, prescription outflow, and restrictions on the drug-to-revenue ratio—the compensation structure for medical service personnel is poised to undergo significant structural changes in the coming years.
IV. Sustainable Development Mechanism
1. Personnel Structure: In 2018, the nurse-to-physician ratio in tertiary public hospitals across China was 1:1.58, surpassing the target of 1:1.25 by 2020 as outlined in the National Health and Healthcare Service System Development Plan. The average daily inpatient workload per licensed physician has been steadily decreasing, while the number of pharmacists per 100 hospital beds has remained stable at approximately 0.82. The proportion of health technical personnel holding senior professional titles (associate senior level or above) was 16.44%, representing an increase of 0.97 percentage points compared to 2016.
2. Personnel Training Capability: In 2018, 92.23% of hospitals had candidates meeting statistical requirements participating in the National Medical Licensing Examination, with an average pass rate of 77.47%, representing a 1.99 percentage point increase from 2017.
3. Disciplinary Development Capacity: In 2018, 80.34% of tertiary public hospitals received research funding support, with 5.64% of hospitals allocating more than RMB 2 million in research funds per 100 health technical personnel. The top five hospitals nationwide in terms of total research funding were West China Hospital of Sichuan University, Zhongshan Hospital Affiliated to Fudan University, Peking Union Medical College Hospital of the Chinese Academy of Medical Sciences, Beijing Children’s Hospital Affiliated to Capital Medical University, and Huashan Hospital Affiliated to Fudan University. The revenue generated from the translation of scientific and technological achievements per 100 health technical personnel reached RMB 13.0593 million, representing a 165.96% increase compared to 2016.
4. The “Two Permits” Policy: The proportion of personnel expenditures to total operational expenditures rose from 32.56% in 2016 to 35.45%, reflecting the principles of rewarding superior performance and compensating based on workload, thereby continuously enhancing the value of technical and labor services.
V. Patient Satisfaction
In 2018, the satisfaction scores for outpatient and inpatient services at tertiary public hospitals across China were 84 and 90, respectively. The five provinces with the highest outpatient satisfaction were Hunan, Jiangsu, Shandong, Jiangxi, and Zhejiang, in descending order. The five regions with the highest inpatient satisfaction were Jiangsu, Shanghai, Shandong, Hunan, and Henan, in descending order. Notably, Hunan, Shandong, and Jiangsu demonstrated relatively high satisfaction levels among both outpatients and inpatients. Outpatients reported the highest satisfaction with nurse communication, physician communication, and medical staff responsiveness, while their satisfaction was lower regarding registration experience, facility environment and signage, and privacy protection. Inpatients expressed the highest satisfaction with medical staff’s attitude toward patients’ families, medical staff responsiveness, and pain management, whereas they reported the lowest satisfaction with admission and discharge information and procedures, physician communication, and hospital meals.
VI. The National Team Role of Hospitals Affiliated with and Administered by the Commission
In 2018, the average length of stay at the 44 hospitals directly affiliated with or administered by the National Health Commission was 7.7 days, with a bed occupancy rate of 105%, indicating operational efficiency higher than the national average for tertiary public hospitals. Eighty percent of these general hospitals demonstrated outstanding performance across various dimensions, with 21 of them securing total research funding exceeding RMB 50 million, thereby underscoring the leading role of these hospitals in scientific research and innovation.
Overall, the capabilities of healthcare institutions in China are on the rise, and this trend is expected to continue. With advancements in informatization and an increase in medical talent, the service quality of China’s healthcare institutions will further improve.
However, returning to the process itself, as this is the first unified performance assessment for tertiary public hospitals, there are inevitably unreasonable aspects in the assessment process. For example, since a large amount of data is collected from the front page of medical records, but due to differences in medical informatization and diagnosis and treatment levels across regions, the quality of the front page of medical records will also vary. Therefore, there is still room for improvement in this assessment method.
However, Sun Jianbo, Project Director at Dashu Yida, stated: “The National Health Commission initiated these reforms in 2018 with the ultimate goal of advancing the development of the entire public hospital system. These efforts aim to familiarize hospitals with assessment procedures, enhance interoperability across various interfaces, and gradually improve hospital data quality. As grassroots informatization capabilities continue to mature, the next phase of assessments will provide the National Health Commission with more comprehensive and reference-worthy big data on public healthcare.”
As we bid farewell to the old and welcome the new, while the achievements of 2018 are indeed gratifying, we must now set our sights on the next round of assessments.
The data and materials required for the assessment are derived from four dimensions: medical quality, operational efficiency, sustainable development, and satisfaction evaluation. These are broken down into 55 indicators (further subdivided into 282 sub-indicators), along with supporting documentation and self-assessment reports from multiple departments. The process involves a wide range of data, including medical record-related information and data from numerous departments such as the Finance Department, Science and Education Department, Pharmacy Department, Outpatient Department, Medical Equipment Department, Customer Service Center, Information Center, Human Resources Department, Medical Affairs Department, and Nursing Department.

Compared with the Performance Appraisal Manual proposed in 2019, the new 2020 edition shows minimal overall changes; however, it adds a new assessment indicator: “proportion of revenue from high-value medical consumables under key monitoring.” This indicator requires calculating the ratio of revenue generated from the 18 types of medical consumables listed in the first batch of the National Key Governance List for High-Value Medical Consumables to the total revenue from sanitary materials during the same period.

Formula for Calculating the Proportion of Revenue from High-Value Medical Consumables Under Key Monitoring
Jiang Songyi, Chief Medical Quality Officer at Huimei Technology, told VCBeat: “The introduction of this indicator primarily aims to address two issues: artificially inflated prices for certain high-value medical consumables and their overuse. Overall, it seeks to alleviate the financial burden on patients and reduce healthcare insurance expenditures, while curbing improper benefit transfers in the sales process of high-value medical consumables. Essentially, this policy is designed to safeguard the public’s health and economic interests, while promoting cost containment within the healthcare insurance system.”
Ye Xin, Deputy Director of the Beijing Research Institute at Yilianzhong, discussed the impact of performance assessments on HIT (Health Information Technology) enterprises: “As the assessment system continues to mature, IT vendors must adjust their business operations and products in accordance with the assessment metrics. This means we must rethink product positioning and planning, standardize and enhance functionalities, and improve both product quality and data quality. Meanwhile, since these assessments involve multiple systems, we must strengthen data interoperability with other vendors, adhere to and jointly establish common standards, and provide hospitals with better health information connectivity. Consequently, a new model of competition and collaboration will gradually emerge among HIT enterprises.”
Performance evaluation in public hospitals serves not only as a beacon guiding the development of the public hospital system but also as a driving force propelling the growth of healthcare-related enterprises. Therefore, the advancement of hospital performance assessments cannot be achieved without corporate support. VCBeat believes that healthcare-related companies can engage from three perspectives to help hospitals better build their medical systems.
Supporting Hospitals in Advancing Assessment Processes
As mentioned above, the process for hospitals to submit materials required for assessment is extremely complex. “When submitting materials in 2019, nearly 30% of hospitals manually entered data to present their plans, failing to achieve automated integration between their internal information systems and the national reporting platform; meanwhile, many hospitals submitted data with quality issues, necessitating secondary submissions,” said Sun Jianbo, Project Director at Dashu Yida, in an interview with VCBeat.
Sun Jianbo stated, “The prevailing solution to this issue is the development of a data platform. Taking Dashu Yida as an example, we can build an intelligent big-data application platform for hospitals, starting from performance assessment indicators. Leveraging intelligent data collection methods, our solution aggregates all intra-hospital data from multiple disparate information systems and diverse data sources without requiring any development work from vendors of hospital business systems. It extracts both historical and incremental data—including electronic medical records and human resources management data—into a data center as required. Furthermore, by applying artificial intelligence and deep learning technologies to structure heterogeneous data, we can perform standardized data conversion in compliance with national health information standards and specifications, thereby constructing a high-quality data warehouse.”
Thus, the performance assessment reporting system based on the big data application platform can achieve automatic extraction and monitoring of performance assessment reporting indicators for secondary and tertiary public hospitals, ensuring the speed and accuracy of indicator extraction.
In this way, enterprises can help hospitals obtain their evaluation results under the existing system in advance. This means that hospitals can improve their weak indicators before the assessment. Fundamentally, such services help hospitals promptly identify potential operational issues and achieve scientific management, thereby promoting the development of the hospitals themselves. On the other hand, given that physicians already engage in high-intensity labor, the availability of third-party agencies to handle related administrative tasks on behalf of hospitals naturally creates corresponding market demand.
Meanwhile, if hospitals can all complete information reporting through automated means, the assessment cycle for hospitals may increase from once a year to once a month. At that time, the state could formulate more precise healthcare reform plans based on data support.
Assisting Hospitals in Addressing “Specialization Imbalances”
Whether hospitals identify their own weaknesses through third-party assessments or proactively seek to strengthen specific areas, the performance metrics involved largely require support from enterprises. Taking healthcare informatization as an example, we can gain insights into the latent market opportunities within this sector.
As is well known, healthcare informatization serves as a key lever for the performance evaluation of public hospitals, with rating systems such as Electronic Medical Records (EMR), Interconnectivity, and Smart Hospital Services imposing corresponding requirements on hospitals.
In the analysis of this assessment, key focal points include the efficiency and quality of medical services, rational drug use, and the graded evaluation of electronic medical record (EMR) systems. Therefore, the implementation of a Clinical Decision Support System (CDSS) can effectively enhance the efficiency and quality of medical services, promote rational drug use, and improve the maturity level of EMR systems.
Taking Peking University Third Hospital’s CDSS as an example, in 2018, the hospital collaborated with Beijing Jiahe Haisen Health Technology Co., Ltd. (hereinafter referred to as “Haisen Health”) to launch a new generation of intelligent CDSS powered by big data and artificial intelligence technologies.
Chen Lianzhong, co-founder of Beijing Jiahe Haisen Health Technology Co., Ltd., stated: “Built upon nearly a decade of accumulated real-world clinical data—comprising over 30 million electronic medical records—from Peking University Third Hospital, this system leverages artificial intelligence to construct a decision-support model covering the entire care continuum, including pre-consultation, intra-consultation, and post-consultation phases. It enables diverse applications such as search functionality, patient profiling, clinical decision support, treatment outcome prediction, and early warning alerts for key indicators.”
It is reported that the CDSS model at Peking University Third Hospital achieves a maximum diagnostic recommendation accuracy of 91.7% in routine disease diagnosis and treatment, reducing the average time to confirmed diagnosis by 0.98 days and shortening the average length of hospital stay by 2.02 days.
Of course, the construction of a Clinical Decision Support System (CDSS) is only one factor contributing to a hospital’s performance evaluation score. In reality, if enterprises can provide hospitals with efficient equipment maintenance solutions, effective appointment scheduling systems for diagnosis and treatment, and more accurate medical record quality control systems, they can similarly support hospitals’ performance evaluations by optimizing service processes, enhancing patient satisfaction, and controlling costs.
Participate in Designing a Superior Assessment Framework
In addition to the two aforementioned types of enterprises that can directly assist hospitals in completing performance evaluations, there are other companies developing higher-quality assessment indicators for the National Health Commission.
For example, in terms of CMI and DRG calculations, Wanghai Kangxin has closely followed the release of the CHS-DRG grouping scheme and took the lead in launching a comprehensive solution supporting CHS-DRG. By leveraging organizational design, lean management, and IT support, it helps hospitals address the impact of DRG-based payment on the healthcare industry and achieve upgrades in their own lean management practices.
However, due to the significant variations in DRG implementation across different regions at this stage, it will take some time to establish a unified version. Therefore, even in the 2019 assessments, there may not be substantial adjustments to the DRG-related evaluation criteria.
During the interview, a healthcare IT professional discussed the situation in Fujian: “The National Health Commission requires tertiary hospitals across China to achieve Level 4 Electronic Medical Record (EMR) implementation and secondary hospitals to reach Level 3. In Fujian, however, tertiary hospitals are required to attain Level 5 EMR implementation, while secondary hospitals must reach Level 4.”
In other words, performance assessments essentially serve as a driving force for lower-ranked hospitals to proactively enhance their capabilities. Under the guidance of central government policies, hospital development can actually accelerate.
Jiang Songyi, Chief Medical Quality Officer at Huimei Technology, also highlighted the same issue: “Among hospitalized patients, one-third experience complications related to venous thromboembolism (VTE), making it the leading cause of preventable in-hospital deaths. However, since medical record data do not adequately reflect performance on this metric, VTE is not included in the assessment indicators for the new year. Nevertheless, this has not prevented top-tier hospitals such as China-Japan Friendship Hospital from implementing corresponding AI-based prevention and control systems, as these systems can effectively address the VTE challenges present within hospitals.”
Therefore, we are pleased to observe the progress of “underperforming hospitals” through unified performance assessments. It is our hope that, as the healthcare system continues to advance, more hospitals will prioritize service-oriented development over assessment-driven metrics in their institutional improvement efforts.