Three Common Pitfalls in Hospital DRG Implementation: A Strategic Guide
Author: Zhang Lehui
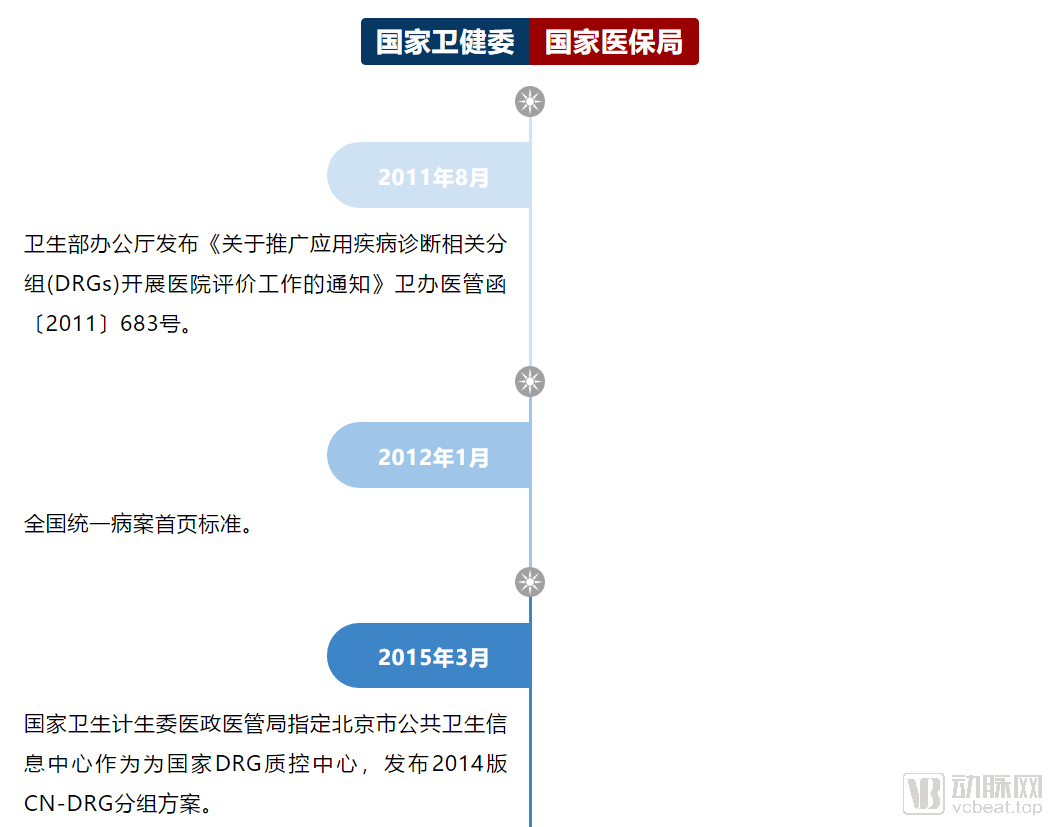
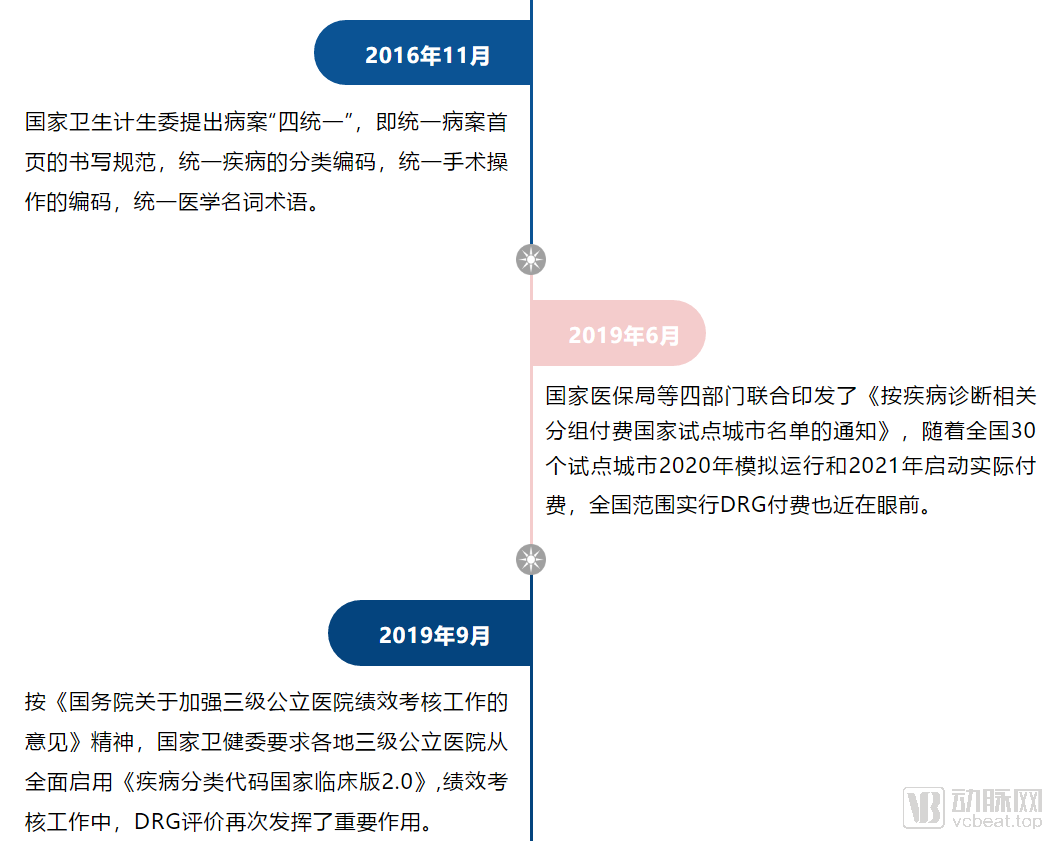
The implementation of Diagnosis-Related Groups (DRG) in China is a process of continuously standardizing national standards. Key milestones are reviewed as follows:
 MDT Management
MDT Management
Pitfall 1: Difficulty in Determining the DRG Implementation Roadmap
As the country gradually standardizes its regulations, many hospitals have not yet initiated DRG implementation; however, numerous departments and clinical units have undergone training on different DRG methodologies at various stages. Consequently, although multiple departments within these hospitals possess knowledge of DRG, it remains difficult to establish a unified understanding of the system.However, the implementation of Diagnosis-Related Groups (DRG) in hospitals requires coordination across multiple departments, constituting a Multidisciplinary Team (MDT) approach to hospital management. In response to the new healthcare reforms, establishing effective “tri-partite linkage” among medical care, health insurance, and pharmaceuticals within the hospital is essential to facilitate its sustainable and sound operation.。
In practice, hospitals are prone to falling into the trap of “indecision,” where differing opinions across multiple departments make it difficult for hospital leadership to reach a decision. For example, should data standardization precede management improvement, or should both be advanced simultaneously? Should DRG information systems be procured first, or should management reforms take the lead? Hospitals are also susceptible to the trap of “arbitrary decision-making,” wherein progress is driven by the perspectives of a few departments without striking an appropriate balance in focus and sequencing. This often results in unnecessary detours and diminished efficiency, yielding half the results with twice the effort.
The hospital did not implement the DRG project in its early stages. Although it avoided the process of gradual standardization under national guidelines, it also failed to gain a first-mover advantage. We recommend that the hospital should no longer hesitate,Align the varying levels of understanding and differing schools of thought regarding DRGs across departments, in accordance with national standards and leveraging the expertise of a mature team., shift from a department-centric project management model to a DRG-based project management model, and take immediate action.
Trap 2: DRGs Make Hospital Management Increasingly Complex
Objectively speaking, the implementation of DRG does indeed require an enhancement in the capabilities of hospital management departments, particularly in datain terms of data-driven management capabilities and hospital operational quality control capabilities. The implementation of DRG has prompted hospital management to transition from the "liberal arts" era driven by processes, towardThe Data-Driven Shift to the “Mathematics” Era, which is often referred to as “letting the data speak,” but ““How to use data” and “what to say” actually require enhanced capabilities.
In practice, hospitals are prone to falling into the trap of “increasing complexity.” When administrative departments lack the capacity for improvement and integration, they hastily impose fragmented demands on clinical staff from multiple angles, leaving clinicians unsure of how to proceed. Moreover, DRG-related knowledge is often dumped onto clinical teams without screening or prioritization, causing significant confusion.
Although implementing Diagnosis-Related Groups (DRG) is no simple task, this phase of complicating the straightforward should ideally be confined within functional departments. Much like transitioning from riding a bicycle to driving a car, one must clarify each step and cultivate good driving habits in a controlled training environment. We recommend that hospital functional departments achieve thorough mastery beforeManagement embodies both “li” (order and rationale) and “guan” (oversight and control), fostering a unified team with a single voice. Together, we engage with clinical practice, simplifying complexity to help streamline operational management while enhancing service quality and care standards.. Just as we have learned to drive cars, we all consider driving to be efficient, and no one would think that driving a car is more strenuous than riding a bicycle.
Trap 3: New Cars, New Books, Long Journeys
DRG Payment and Evaluation: Essentially Triggering Stock Reform of Hospital Development Resources. In the face of this pressing situation, many large hospitals have made substantial investments in purchasing DRG information systems and mastered their operation; nevertheless, they still feel inadequate and uneasy when confronting the imminent implementation of DRG-based payment and evaluation.
In practice, hospitals are prone to falling into the trap of “buying a new car and getting a new driver’s license only to embark on a long journey.” This means that while hospitals recognize that Diagnosis-Related Groups (DRG) are critical to their survival and development, they tend to focus on “tools” rather than “capabilities,” thereby lacking control over “outcomes.” In fact, “tools” that can be acquired simply by spending money are clearly not core competencies, although they constitute basic prerequisites; it is the “capabilities” cultivated through time and effort that represent true core competencies. This aspect requires “coaching and navigation.”
Implementing DRGs requires cultivating three teams, namelyStandardization teams (medical records, information technology, and pricing), management teams (medical affairs, health insurance, quality control, performance management, nursing, hospital infection control, pharmacy, biomedical engineering, etc.), and clinical teams have distinct priorities: standardization teams focus on ICD, management teams on DRG, and clinical teams on clinical classifications that are more granular than ICD. Therefore, we recommend that standardization teams adopt localized DRG information systems compliant with national standards; management teams utilize flexibly configurable, data-driven management tools; and clinical teams employ internet-enabled information systems that integrate medical practice, education, research, and prevention while supporting academic exchange.。
The author of this article has assisted dozens of hospitals in implementing DRG projects and has observed that hospitals are prone to falling into the three major pitfalls mentioned above. In summary, it is recommended that hospitals prioritize the following when implementing DRG projects:Management Empowerment, particularly the capability for data-driven quality control management of hospital operations, the ability to manage multidisciplinary teams (MDTs), and the capacity to align personnel with information systems; secondly, it is essential to clearly recognizeThe Implementation of DRG Facilitates the Efficient Allocation of Medical Resources, the process of implementing DRG is also a form of management resource allocation; third,Act Now, Management First, with DRG group management as the core and clinical teams’ mastery of DRG as the gold standard for successful implementation.
In the DRG era, does our team master the construction of mathematical models?
