Third-Party Evaluation of Medical AI: Insights from CAICT and Seven Leading Enterprises on Standardization and Future Development

DeepWise
Developer of Artificial Intelligence Medical Imaging Diagnosis System

UNITED IMAGING
Artificial Intelligence Medical Product Developer

JIANPEI
Medical Imaging Big Data Analysis Technology Developer
Over the past five years, AI in medical imaging has moved beyond its early development phase—namely, the technology validation stage—but many of the challenges that emerged at the industry’s inception persist to this day.
First, due to the lack of sufficiently rich and effective data for corporate training, many AI products struggle to demonstrate robust diagnostic performance in clinical settings. Underlying this issue are the high costs of data annotation and the significant challenges in data acquisition. To date, ethical concerns surrounding medical data have not been addressed through legislation, making it difficult to standardize how companies obtain training data.
Second, constrained by data and algorithms, only a few enterprises have achieved, to some extent, AI solutions capable of handling multi-disease, multi-threaded tasks in line with clinical practice. While numerous AI products can address single-disease issues, they struggle to fully meet the actual needs of physicians.
Third, there is a lack of unified data standards, testing platforms, and third-party databases for AI products. When presenting product accuracy and sensitivity metrics, companies often cite only the figures without disclosing the methodologies used to obtain them. If the database employed for training is subsequently used for evaluation, it is akin to students taking an exam they themselves designed, casting doubt on the validity of the results.
Finding answers to these challenges requires not only the efforts of enterprises themselves but also policy support. For several years, institutions such as the Center for Medical Device Evaluation of the National Medical Products Administration (NMPA) and the China Academy of Information and Communications Technology (CAICT) have been working tirelessly to standardize medical AI. The results of the evaluation of AI-assisted diagnostic products for pneumonia imaging (hereinafter referred to as the “Pneumonia AI Evaluation”), released at this World Artificial Intelligence Conference, represent the prescription offered by CAICT and other institutions to address the third issue.
The Pneumonia AI Assessment was guided by the Department of Science and Technology of the Ministry of Industry and Information Technology (MIIT) and jointly conducted by the China Academy of Information and Communications Technology (CAICT), the Artificial Intelligence Industry Alliance, and the MIIT Key Laboratory for Research and Verification of Medical Artificial Intelligence.This is an innovative assessment conducted within a fully enclosed, independent sandbox monitoring environment, where all processes—from data collection and annotation to subsequent testing and scoring—are performed independently of the enterprises involved., which ensures the fairness and authority of the evaluation.
A representative from the China Academy of Information and Communications Technology (CAICT) told VCBeat, “A sandbox environment implies a completely isolated state. In previous evaluations, processed data were often handed over to enterprises for testing. However, in this round of testing, enterprises deployed their AI products unidirectionally via VPN. After deployment, we first closed the communication channel before conducting tests with the data. All test data copied from hospitals remained in a cached state and were immediately deleted upon completion of the testing.”
Each data point used in the evaluation underwent rigorous screening and curation to ensure the comparability of the test environment with real-world settings. Ultimately, the database comprised a total of 1,000 test cases collected from seven designated medical institutions for COVID-19 treatment: Shanghai Public Health Clinical Center, Zhongnan Hospital of Wuhan University, Wuhan No. 3 Hospital, Hangzhou First People’s Hospital, The First Affiliated Hospital of Zhejiang University, Beijing Ditan Hospital, and Wenzhou Central Hospital. Among these 1,000 cases, 30.7% were from healthy individuals, 36.2% from patients with COVID-19, and 33.1% from patients with non-COVID-19 conditions.
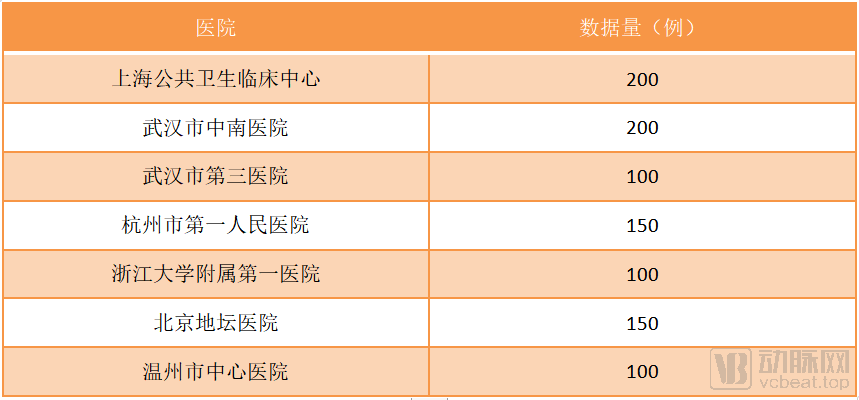
Data Sources for the Evaluation of Intelligent CT Imaging Diagnostic Technology Applications (Data sourced from CAICT)
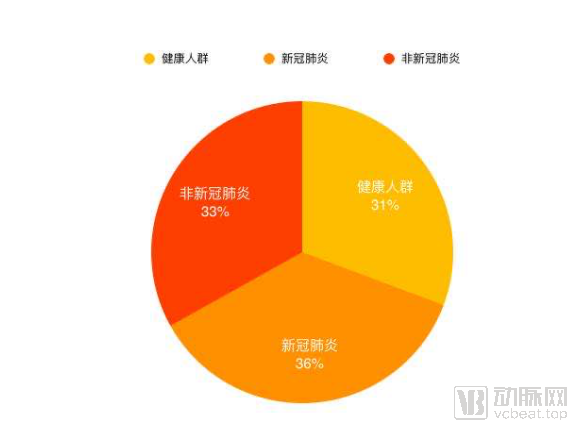
Data Distribution (Source: CAICT)
To ensure the database aligns as closely as possible with real-world scenarios, the working group fully considered three dimensional indicators during data collection: acquisition equipment and configurations, data diversity, and case distribution. Specifically, the non-COVID-19 database includes various conditions such as pulmonary edema and common pneumonia. Furthermore, to account for robustness and anti-interference capabilities, 70 cases of non-standard imaging data, frequently encountered in actual clinical practice, were incorporated into this evaluation.
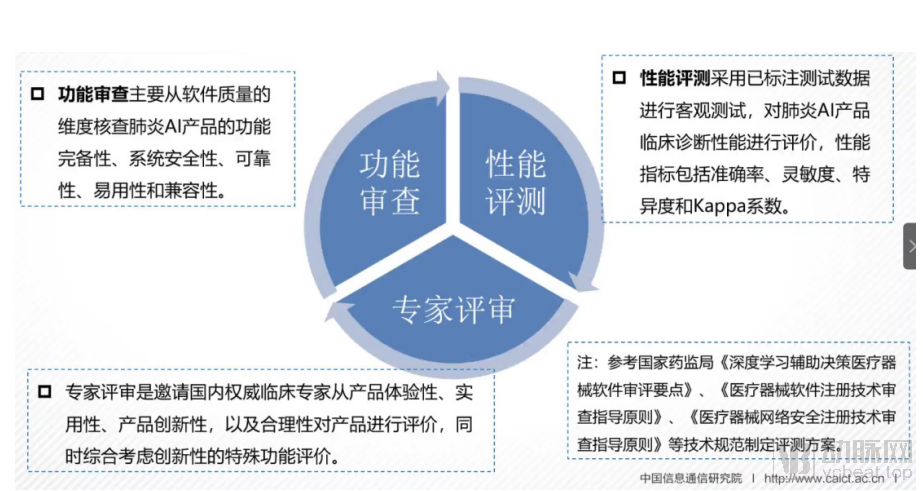
The subsequent evaluation process has also been thoroughly deliberated. The entire evaluation framework is conducted from three perspectives: functional review, performance assessment, and expert review. The functional review primarily focuses on software quality, examining the pneumonia AI product'sReliability, Ease of Use, Compatibility, Functional Completeness, and System SecurityFive Dimensions. Performance evaluation employs observable testing using annotated test data to assess the clinical diagnostic performance of AI products for pneumonia, with metrics includingAccuracy, Sensitivity, Specificity, and Kappa CoefficientFour Dimensions. Expert review involves inviting authoritative domestic experts to evaluate products based on user experience, practicality, innovation, and rationality, while also comprehensively considering the evaluation of special features related to innovation.
Ultimately, the AI-assisted diagnostic imaging products for pneumonia developed by seven medical AI companies—Beijing BioMind Technology Co., Ltd., United Imaging Intelligence Co., Ltd., Shanghai Yitu Healthcare Technology Co., Ltd., DeepWise (Shanghai) Medical Technology Co., Ltd., Ping An Technology (Shenzhen) Co., Ltd., Hangzhou Jianpei Technology Co., Ltd., and Shanghai Haohua Information Technology Co., Ltd.—stood out among the 17 participating medical AI firms.
Overall, this evaluation can be said to have broken the previous situation in the medical AI industry where companies were talking to themselves and fighting their own battles. This is not only the first time that official organizations have held a competition for medical AI imaging-assisted diagnostic products, but it is also an evaluation of "AI anti-epidemic products" at a special historical moment, making its significance extraordinary.
“Overall, AI products for pneumonia developed by some domestic artificial intelligence enterprises have reached a high level, with relatively mature and comprehensive functionalities. Nearly one-third of these products achieve accuracy, sensitivity, and specificity exceeding 90% in pneumonia detection. On the basis of perfecting core functionalities, certain products are gradually developing distinctive innovative features that provide significant assistance to physicians, such as AI-based early warning systems for infectious pneumonia and intelligent teaching tools, which have also gained recognition from authoritative medical experts.” After analyzing the results of the entire evaluation, the China Academy of Information and Communications Technology (CAICT) drew the above conclusion.
However, based on the actual scores of the 17 companies, there are still significant disparities in the product performance of AI enterprises. Furthermore, only a small fraction of products have achieved recognition capabilities for COVID-19, and the precision of lesion localization requires further improvement. A minority of products failed to effectively classify pneumonia; enhancing product functionality and performance necessitates training with more extensively annotated data.
“Performance testing is the primary factor driving the divergence in results.” A relevant official from the China Academy of Information and Communications Technology (CAICT) stated that performance testing includes assessing “pneumonia presence,” “COVID-19 presence,” and “lesion location.” According to the evaluation results, while most enterprise products demonstrated effective screening for “pneumonia presence,” only three companies achieved accuracy, sensitivity, and specificity rates above 80% in the “differential diagnosis of COVID-19 pneumonia,” with some metrics exceeding 90%.
“The reasons for this outcome are multifaceted. As this was our first time deploying a sandbox environment for testing, some enterprises were unfamiliar with our data formats and testing infrastructure, leading to certain operational errors. Some companies encountered technical glitches during the testing process—such as sudden software crashes—which prevented subsequent data from being evaluated. By the time supplementary testing was conducted, the model might have already undergone some degree of drift. In such cases, we typically granted the affected companies an opportunity for re-evaluation. However, the more critical factor ultimately lies in the quality of training data and accumulated technical expertise.”
“From a temporal perspective, the approximately three-month epidemic period was not long enough for enterprises to acquire sufficient data or conduct adequate model training. Coupled with potential issues in subsequent annotation processes, these factors contributed to suboptimal evaluation results for many companies. In contrast, enterprises with richer technical accumulations and larger training datasets achieved better evaluation outcomes, which is an objective factor.”
“From a broader perspective, many companies make adjustments to product features to expedite commercialization, enabling them to secure medical device regulatory approval and bring products to market as quickly as possible.” Under this incentive mechanism, companies may have simplified their AI products to some extent. However, evaluation is not equivalent to regulatory approval; the key to an artificial intelligence company’s success lies in developing products that meet physicians’ actual clinical needs.
To gain deeper insights into the actual outcomes of this assessment and distill valuable lessons, VCBeat interviewed the top seven AI companies that achieved outstanding results, aiming to explore the future development trajectory of artificial intelligence through these conversations.
About This Assessment
Q: From an enterprise perspective, what essential measures must be taken to ensure AI performance and effectively pass testing?
Zhan Yiqiang, United Imaging Intelligence:Since the data for this test includes both COVID-19 and non-COVID-19 cases, our approach is to augment existing AI-powered pneumonia products with auxiliary diagnostic capabilities for COVID-19.
The limited availability of data on COVID-19 has imposed new requirements on the annotation process. To address this, we adopted a "human-in-the-loop" annotation approach, wherein physicians and expert teams annotated a small subset of COVID-19 data. The algorithm was then trained on this annotated portion to develop an initial model. Although the performance of this initial model was suboptimal, it gradually matured as new data were incrementally incorporated.
The segmentation phase utilized the self-developed segmentation engine of United Imaging Intelligence. This AI engine is capable of segmenting lesions themselves, as well as pulmonary segments and lobes. This segmentation process effectively accomplishes two tasks: first, it determines the presence of lesions; second, it generates extensive quantitative data through lesion segmentation, enabling the calculation of the infection proportion within each pulmonary segment’s lesion area to assess disease severity. During the period of strained medical resources in Wuhan, this capability effectively facilitated the optimal allocation of resources.
Therefore, to ensure the quality of AI products for COVID-19, it is essential to employ efficient annotation methods, develop innovative AI algorithms, and engage in in-depth communication with physicians.
BioMind's Li Jingjue:There is significant overlap between the CT imaging features of COVID-19 and non-COVID-19 pneumonia, yet distinct specificities also exist. During the AI’s learning process, it is essential to clearly define the etiological context of the data and determine whether the patient has COVID-19. If not, we must further confirm whether the condition is bacterial pneumonia, influenza A, or influenza B. Therefore, for such a database with broad data dimensions, our training methodology provides us with a substantial advantage.
Haohua Technology Zhou Ying:Long-term accumulation of experience is essential. For instance, while physicians often face challenges in differentiating between influenza A and influenza B during routine diagnosis, we can address these issues through AI solutions validated by multi-center clinical trials. Following the COVID-19 pandemic, we were fortunate to access substantial COVID-19 data, which further enhanced our products. This may constitute a competitive advantage over some other enterprises.
Shi Lei from Yitu Healthcare:Product design, R&D, internal testing, external validation, data annotation, in-house expert training on the product, and experts’ domain understanding—AI performance is the result of multiple factors working in concert. The pandemic has tested enterprises, requiring them to rapidly develop products using small-sample datasets while ensuring generalizability across multiple hospitals. This demands comprehensive corporate capabilities built on years of accumulated experience. It also explains why only a subset of companies passed the tests, with noticeable performance gaps among them; this is merely the tip of the iceberg, while the submerged portion reflects the true strength of these enterprises.
Q: How much data was used to train the AI algorithm for COVID-19?
DeepWise's Li Yiming:Pneumonia data comprises tens of thousands of cases.
BioMind's Li Jingjue:There are approximately 10,000 cases with nucleic acid testing as the gold standard, and approximately 20,000 cases without nucleic acid testing as the gold standard.
Zhou Ying, Haohua Technology:5,000 cases of non-COVID-19 data and 1,000 cases of COVID-19 data.
Q: The China Academy of Information and Communications Technology (CAICT) has stated that during material review, enterprises with larger volumes of training data for COVID-19 often achieve relatively better outcomes. How should the relationship between data volume and AI performance be viewed?
DeepWise's Li Yiming:While the volume of data is important, it is not the decisive factor. The development of an AI product involves not only training data but also core algorithmic models, as well as testing and clinical validation. Furthermore, in training AI for COVID-19, we were primarily enhancing existing products. From a purely radiological sign perspective, the differences between COVID-19 pneumonia and traditional pneumonia are not substantial; however, there are other ancillary information points that require attention, which constituted the focus of our model adjustments.
United Imaging's Zhan Yiqiang:Data volume is critical for training AI algorithms for COVID-19, with data sources being the next most important factor. As the outbreak in Wuhan was particularly severe, relying exclusively on training data from Wuhan could bias the resulting AI model toward severe cases. Therefore, we incorporate data collection from diverse geographic regions to effectively enhance the reliability of our AI products.
Shi Lei, Yitu Healthcare:Data volume is one of the factors affecting performance. Data quality, annotation quality, model design, and training are all critical influencing factors. Excellence in every stage is essential to achieve superior performance. Therefore, while the accuracy of AI products is related to data volume, it should not be oversimplified to mean that possessing large amounts of data alone guarantees excellent AI outcomes.
BioMind's Li Jingjue:Robust AI relies on generalizability and big data support. Discrepancies between laboratory results and real-world performance indicate insufficient AI generalizability. This issue is akin to a stubborn skin condition for artificial intelligence—difficult to resolve, yet imperative to address. The solution is not overly complex: AI companies must use training data derived from devices of different manufacturers, various models, and CT scans with varying slice thicknesses. This process requires substantial time investment. Furthermore, regarding big data support, the lack thereof is the fundamental reason why many enterprises fail to achieve satisfactory AI outcomes. Artificial intelligence stems from big data; without integration with effective big data, favorable results are virtually unattainable. Both the volume and quality of data must be strictly controlled.
Q: Enterprises often face a new environment when deploying their solutions in hospitals, and the same applies to validation in this sandbox environment. To ensure that AI products demonstrate high accuracy, sensitivity, and specificity from the outset of deployment, how should enterprises respond?
DeepWise's Li Yiming:This is essentially a matter of experience. Upon entering hospitals, we encounter diverse PACS systems and imaging equipment, a challenge that indeed existed during the early deployment of DeepWise’s products. However, through practical implementation in hundreds of hospitals, we have now accumulated more than ten integration solutions for PACS connectivity. All these solutions are supported by our AI imaging platform and can be enabled simply by selecting the appropriate configuration options. If the imaging equipment adheres to more standardized protocols, integration becomes even easier, as we have already prepared for such standard protocols during our AI development phase.
Shi Lei, Yitu Healthcare:For AI products to deliver tangible value in hospital settings, they must undergo rigorous validation across multiple dimensions. The primary challenge lies in achieving stable integration with existing hospital information systems. Given the complexity of these systems, companies lacking relevant experience may encounter significant difficulties even at this initial stage. Furthermore, AI products must be compatible with data generated by diverse medical devices. Insufficient generalization capability means that subtle variations arising from different imaging conditions can adversely affect AI performance. Therefore, during AI research and development, enterprises must thoroughly consider data training methodologies and the diversity of data sources, while implementing targeted design and training for specific edge cases.
The second challenge arises when AI is integrated into the system: insufficient control over subtle variations in imaging conditions across data generated by different devices and from diverse geographic regions can lead to suboptimal diagnostic performance. Therefore, during algorithm training, enterprises must fully consider training methodologies and the diversity of data sources, while incorporating robustness designs to address certain edge cases.
Huang Lingyun, Ping An Technology:Our understanding of this issue can be summarized in three key points: first, we must start from actual clinical needs, business process scenarios, and existing technological capabilities to help healthcare professionals and medical institutions achieve the "Three Improvements and Two Reductions"—improving efficiency, effectiveness, and experience, while reducing costs and risks.
Second, innovation: We must have the courage to pursue technological innovation, addressing challenges such as the segmentation of diseased lungs and pathological lobes in COVID-19 cases, as well as the limitations of insufficient data volume and precise annotations under initial conditions. We implemented new segmentation networks that had proven effective for pathological abdominal organs in CT scans, along with novel approaches such as transfer learning and human-in-the-loop semi-automatic annotation, resulting in significant improvements in performance metrics.
Third, effective project management is essential. Functional and performance evaluations target the entire pneumonia system architecture, requiring close collaboration among professionals across various domains—from algorithms to product design and user interaction—to form an integrated whole and deliver optimal product outcomes.
Q: The CAICT’s conclusions mention that “system reliability needs to be further improved.” How should enterprises enhance the reliability of their products?
JIANPEI’s Zhou Binbo:System reliability is categorized into two types: first, the inherent reliability of the software itself, specifically its ability to operate fault-free over extended periods; second, the reliability of diagnostic results, which entails maintaining high accuracy during prolonged use and ensuring consistency of results across different devices. During software development, enterprises must implement quality control measures in accordance with their quality management systems throughout the requirements, development, and testing phases.
Ping An Technology's Huang Lingyun:There are two levels of consideration. First, from the perspective of algorithm performance, to enhance system reliability, we should conduct training using multi-center, multi-modal, and multi-brand data, and adopt effective algorithms from research fields such as domain adaptation to improve system robustness. Second, from the perspective of system operation, we need to design a sound software system architecture. Starting from the product design phase, we should properly plan for concurrency, pending data sorting, and parallel computing stability, and strictly adhere to standardized software development processes.
Q: How to view the option of a lower innovation score?
Ping An Technology's Huang Lingyun:Innovation scores in this assessment were generally low. From my perspective, most companies’ products focus on pneumonia lesion segmentation and quantitative measurement, leading clinicians to perceive these functionalities as largely homogeneous; there is a clear desire for more breakthrough innovations. However, clinical breakthroughs require time. As we continue to systematically organize and structure COVID-19 data, and leverage artificial intelligence to deeply explore new capabilities such as disease outcome prediction, we are confident that these advancements will provide greater support to clinical practice.
Furthermore, enterprises must prioritize innovation and avoid adhering to conventional practices. While medical AI addresses entrenched inefficiencies in healthcare workflows, it requires novel perspectives and innovative algorithmic frameworks for implementation. Moreover, it is overly simplistic to assume that large-scale annotated deep learning alone can resolve training challenges; such an approach hinders scalability. A comprehensive consideration of R&D timelines, human resource costs, and system performance is essential. Fundamental methodological innovations should be employed to optimize the learning process, thereby enhancing the accuracy and generalization capabilities of the final AI system.
# Future Development
Q: How do you view the future development of regulatory approvals?
DeepWise's Li Yiming:At this juncture, the state has provided substantial policy and financial support for the approval of AI products. However, given the current severe homogenization of products, the first-of-its-kind product to seek approval will inevitably face more stringent scrutiny. As certifications for this category of products gradually emerge, the next challenge to address will be the regulatory approval process for iterative updates of innovative software; after all, it is unreasonable to subject a single product to repeated reviews seven or eight times.
From my perspective, the future approval process for AI products will feature a more scientific and applicable testing framework that ensures product updates and iterations while guaranteeing safety and efficacy, thereby saving significant costs and effort for both enterprises and regulatory bodies.
JIANPEI’s Zhou Binbo:From a regulatory perspective, the most pressing challenge we face is the excessively long approval timeline. Since we began preparing for Class III registration, more than two years have passed, during which the core of our AI product has undergone numerous iterations. The traditional medical device approval process is truly ill-suited for innovative enterprises.
However, starting two years ago, the intervention of institutions such as the Center for Medical Device Evaluation (CMDE) and the China Academy of Information and Communications Technology (CAICT) has been establishing third-party evaluation platforms and databases. If these evaluation results gain widespread recognition, they could save enterprises a significant amount of time. Requiring companies to design clinical trials for every update would entail an excessively long timeframe.
Q: Medical artificial intelligence has been developing for many years. Why have third-party evaluation standards and third-party evaluation databases only begun to be established this year?
Yitu Healthcare’s Shi Lei:The current wave of development in the medical AI industry has been underway for several years. However, in absolute terms, three to four years is a relatively short period for AI, as an emerging technology, to penetrate and mature within the established healthcare sector. Even today, AI products continue to integrate with the existing medical ecosystem through rapidly evolving forms, diverse categories, and varied implementation models, underscoring the industry’s strong innovative capacity and boundless vitality.
However, this also means that the maturation of industry awareness and the establishment of industry standards cannot be achieved overnight; they require a gradual process. In recent years, institutions such as the National Institutes for Food and Drug Control (NIFDC) and the China Academy of Information and Communications Technology (CAICT) have taken the lead in establishing data standards and third-party databases, which contributes to the long-term development of the industry. The medical AI sector is gradually becoming standardized, and from a temporal perspective, it is not too late.
Cheng Guohua, JIANPEI:In 2016, AlphaGo’s matches against Go masters sparked a public frenzy over AI, and it was precisely at this time that a large number of companies established their foothold in the field.
Subsequently, medical AI underwent a period of diverse competition, followed by a gradual convergence of understanding. For an emerging technology, four years is not a long time.
During this period, many enterprises and institutions sought to become standard-setters. However, prior to reaching consensus, such standards garnered little recognition from others. Stakeholders held divergent views on key issues, including what types of databases and standards should be established, and which should be prioritized over others. Each party had its own considerations.
Therefore, the recent involvement of institutions such as the China Academy of Information and Communications Technology (CAICT) and Peking Union Medical College Hospital in establishing data standards and third-party databases is actually the result of long-term considerations. It also signifies that previously fragmented perceptions are being unified, and a new consensus on ecosystem awareness and understanding is emerging. This is a reassuring development, as the AI field is gradually becoming more standardized due to these efforts, and it is not too late at this juncture. Furthermore, with the gradual approval of Class III medical device registrations, the timing has matured.
Q: Where is the future of AI in medical imaging headed?
Zhan Yiqiang, United Imaging Intelligence:It is difficult to describe what future AI will specifically look like, but the development path of UNITED IMAGING is at least moving toward its idealized future. Here are two perspectives for consideration.
First, we address issues within individual departments by focusing on specific disease types. Taking stroke as an example, the initial step is to determine whether the patient is experiencing hemorrhagic or ischemic stroke. In the case of hemorrhage, the next step is to assess whether midline shift has occurred. Subsequently, the patient should be guided to undergo CT perfusion imaging to evaluate the actual scoring indices. In summary, while there is a wide variety of diseases, AI is currently capable of handling only a limited number of conditions. We are systematically tackling the most critical and worthwhile disease challenges one by one.
Second, by adopting an anatomical approach, a single chest CT scan can leverage AI-assisted screening to detect multiple conditions, including pulmonary nodules, pneumonia, rib fractures, esophageal cancer, and lymphadenopathy. In radiology, there is a concept known as “incidental findings.” For example, an orthopedic surgeon reviewing a patient’s chest CT might notice a suspicious lesion, which upon further confirmation is identified as a tumor. This is an incidental finding, which is why United Imaging Intelligence integrates functions such as fracture detection and tumor detection into a unified platform.
When processing cases, individuals often exhibit subjective bias. For instance, an orthopedic surgeon attending to a patient may focus primarily on whether a fracture has occurred, thereby potentially overlooking pulmonary lesions. This is where AI demonstrates its advantage: free from psychological preconceptions, it can promptly identify incidental findings and extract more information from a single image. From this perspective, we can uncover the more profound value of AI.
BioMind's Li Jingjue:Public health prevention and control represent a key direction for the future development of AI in medical imaging. For radiologists, identifying pneumonia is a fundamental professional competency; however, the situation differs with COVID-19. While physicians at major hospitals in Wuhan might recognize COVID-19 on CT scans at a glance, those in cities less severely affected by the epidemic may not be able to do so immediately. This constitutes the first step in the application of AI: distinguishing between COVID-19 and non-COVID-19 cases.
Furthermore, after distinguishing between COVID-19 and non-COVID-19 cases, physicians must further identify the specific type of pneumonia. This poses a greater challenge for clinicians and represents the core value of AI. Particularly at the primary care level, if AI can assist physicians in making preliminary assessments, thereby enabling targeted etiological testing for suspected patients, it would significantly strengthen the epidemic prevention and control system.
This is also one of the key reasons why medical AI is highlighted in the development of new infrastructure. When a novel epidemic virus emerges, although AI cannot directly identify the specific type of the new virus, it can generate outputs distinct from those of previously trained categories—such as flagging cases as “other pneumonia”—based on its prior learning. This serves as an alert to draw the attention of monitors. Therefore, AI will be a crucial force in building future public health prevention and control systems.
Acknowledgments: We thank the following experts for their strong support of this article.
Min Dong, Director of the Smart Health Department, Cloud Computing and Big Data Research Institute, China Academy of Information and Communications Technology
Wang Xiumei, Deputy Director of the Smart Health Department, Cloud Computing and Big Data Research Institute, China Academy of Information and Communications Technology
Wang Daoyang, Senior Consultant, Smart Healthcare Center, East China Branch of the China Academy of Information and Communications Technology
Huang Lingyun, Senior Technical Expert, Medical Imaging Technology Group, Intelligent Vision Technology Team, Ping An Technology
Zhan Yiqiang, Chief Operating Officer of United Imaging Intelligence Co., Ltd.
Li Jingjue, CEO of Greater China at BioMind
Vice President of Hangzhou Yitu Healthcare Technology Co., Ltd. Shi Lei
DeepWise, Li Yiming
Cheng Guohua, Chairman of Hangzhou Jianpei Technology Co., Ltd.
Zhou Binbo, Product Director of Hangzhou Jianpei Technology Co., Ltd.
Zhou Ying, General Manager of Shanghai Haohua Technology Co., Ltd.
(The above list is in no particular order.)