Imvax Announces $112 Million Series C Financing to Advance IGV-001, an Autologous Cell Vaccine for Newly Diagnosed Glioblastoma

Imvax
Developer of Novel Vaccines and Immunotherapies
Recently,Biotechnology company Imvax announces the completion of a $112 million Series C financing round. The round was led by HP WILD Holding AG, with participation from Invus, Ziff Capital Partners, Magnetar Capital, and TLP Investment Partners.The proceeds from this financing round will be primarily used by the company to advance the clinical development of its lead candidate, IGV-001, for the treatment of glioblastoma (GBM). Interim results from the Phase 1b trial were presented at the 2019 American Association for Cancer Research (AACR) Annual Meeting, demonstrating that IGV-001 achieved superior efficacy compared to standard of care in patients with newly diagnosed GBM, with prolonged overall survival (OS) and progression-free survival (PFS).
Additionally, Imvax raised $14.7 million in Series A financing and $40 million in Series B financing in 2017 and 2019, respectively. The Series B round was jointly participated in by WILD Group Management, Magnetar Capital, and Ziff Capital Partners. Imvax has raised a total of $166.7 million across three rounds of financing.

Experienced Founding Team: Three members with medical backgrounds and one with operational experience
Imvax, founded in 2015 and headquartered in Philadelphia, USA, is a company dedicated to researching novel vaccines and immunotherapies for the treatment of glioblastoma and other cancers. Imvax was established byDavid W. Andrews, Craig Hooper, Arthur W. Howe, and Peter B. CorrFounded in Philadelphia in 2015. Among the four co-founders of Imvax,David W. Andrews, Craig Hooper, Peter B. Corr IIIThe founders have a background in medical research,Arthur W.HowePossesses extensive experience in media operations.
David W.AndrewsHe is the Co-Founder and Chief Medical Officer of Imvax, Inc. Dr. Andrews has 30 years of experience as an academic neurosurgeon specializing in brain tumors. He was awarded the prestigious NIH (National Institutes of Health) Physician Scientist Award for his research on brain tumors and is dedicated to finding better treatments for glioblastoma.
Craig HooperHe is the Co-founder and Chief Scientist of Imvax, Inc. Hooper works closely with his colleague Andrew; together, they raised $7 million in charitable funding to advance the development of immunotherapies for glioblastoma multiforme (GBM).
Peter B.CorrHe is the co-founder and chairman of the board of Imvax, Inc. Dr. Corr earned his Ph.D. from the Georgetown University School of Medicine and conducted research in molecular biology and pharmacology at Washington University for 18 years.
Arthur W. Howe is the Co-Founder and Chief Financial Officer of Imvax, Inc. Mr. Howe holds a bachelor’s degree and an MBA from the University of Pennsylvania. Mr. Howe oversees the company’s financial affairs, including financial planning, financial risk management, recordkeeping, and financial reporting. He also serves as the Chief Business Officer, responsible for operations, strategy, and development.
In 2005, Howe co-founded a mobile location technology platform. Prior to joining Verve, Howe served as a news reporter, marketing director, and chief financial officer at a large newspaper company, and also held the positions of CEO and President at several major traditional newspapers. Howe has received numerous accolades in journalism and public service, including the Pulitzer Prize, the Scripps Howard Award for Public Service, and the inaugural Benjamin Franklin Award. Two alternative weekly publications under his management, The Village Voice and LA Weekly, have won Pulitzer Prizes.
IGV-001 Vaccine Developed Based on the Patient’s Own Cancer Cells
Glioblastoma multiforme (GBM) is a grade IV malignant tumor, nourished by an abundant and abnormal tumor vasculature. The tumor consists primarily of abnormal astrocytes but also contains other components such as blood vessels and necrotic cells. Glioblastomas infiltrate and invade adjacent brain regions. They can sometimes spread to the contralateral hemisphere of the brain via connecting fibers (corpus callosum).
Glioblastoma multiforme (GBM) poses a severe threat to patients’ survival. Imvax’s lead candidate, IGV-001, is an autologous tumor cell vaccine currently in early-stage clinical trials as a potential treatment for glioblastoma. IGV-001 leverages the patient’s own immune system as a defense mechanism to target tumor cells, delivering a multi-pronged therapeutic effect.
This cell-based vaccine is derived by modifying the patient’s own tumor cells. The modified vaccine can target residual tumor cells that cannot be surgically resected. Imvax employs a three-step process to develop the IGV-001 vaccine for cancer treatment:
Step 1: Collection, treatment, and implantation of patient cells;
Step 2: Immunogenic cell death, patient-specific antigens, and innate immune system activation;
Step 3: Long-term adaptive immune activation and response.
Live cells are extracted from the patient and immediately treated with IMV-001, an IGF-1R antisense oligodeoxynucleotide that induces a stress state; the resulting cell death is controllable. Additionally, excess IMV-001 is released in an adjuvant manner from the chamber at the implantation site. The treated samples are encapsulated within bio-diffusion chambers equipped with subcellular exclusion limits, which trap tumor cells inside. These bio-diffusion chambers are irradiated and implanted into the patient’s abdomen on the second day after surgery. Serving as a controllable reservoir of antigens, they release their contents 48 hours after implantation.
Vertebrate cell death occurs via two mechanisms: accidental cell death and regulated cell death. Accidental cell death is a biologically uncontrolled process, whereas regulated cell death involves tightly structured signaling cascades and molecularly defined effector mechanisms. Due to varying exposures to drugs, radiation, and stressors, regulated cell death can manifest in multiple forms.
IGV-001 performs multiple functions simultaneously in recruiting the innate immune system to the implantation site. First, the surgical wound triggers an immune response, which is amplified by the presence of the vaccine. The vaccine is implanted into the patient’s abdomen; as its contents disseminate throughout the body, the immune system is reprogrammed to kill cancer cells. Due to the addition of excess IMV-001, antigen release occurs alongside free, unbound IMV-001. IMV-001 contains intrinsic CpG dinucleotide motifs that act as adjuvants to further stimulate the innate immune response. Specifically, IMV-001 promotes antigen uptake and stimulates pro-inflammatory responses in plasmacytoid dendritic cells (pDCs). Upon maturation, these pDCs migrate via lymphatic vessels to activate the nearest lymph nodes.
When these cells migrate to nearby lymph nodes, they continue to produce signals that optimize the surface for T cell activation. By the time dendritic cells (DCs) reach their destination (approximately one day later), their cell surfaces are laden with tumor antigens and stimulatory molecules ready to activate T cells. Each T cell population is specific to one of the various potential antigens generated by autologous tumor cell preparations. The T cells proliferate and promote a long-lasting adaptive immune response, seeking out and destroying tumor antigen-bearing cells elsewhere in the body, while maintaining tolerance to non-tumor “self” antigens.
In cases of glioblastoma, the blood-brain barrier remains open within one week after surgery, allowing sufficient time for the first wave of adaptive immune responses to infiltrate and attack residual tumor tissue. As a therapeutic vaccine, IMV-001 currently appears to be safe, with no evidence suggesting that it induces systemic inflammatory responses.
Phase Ib Clinical Trial Results
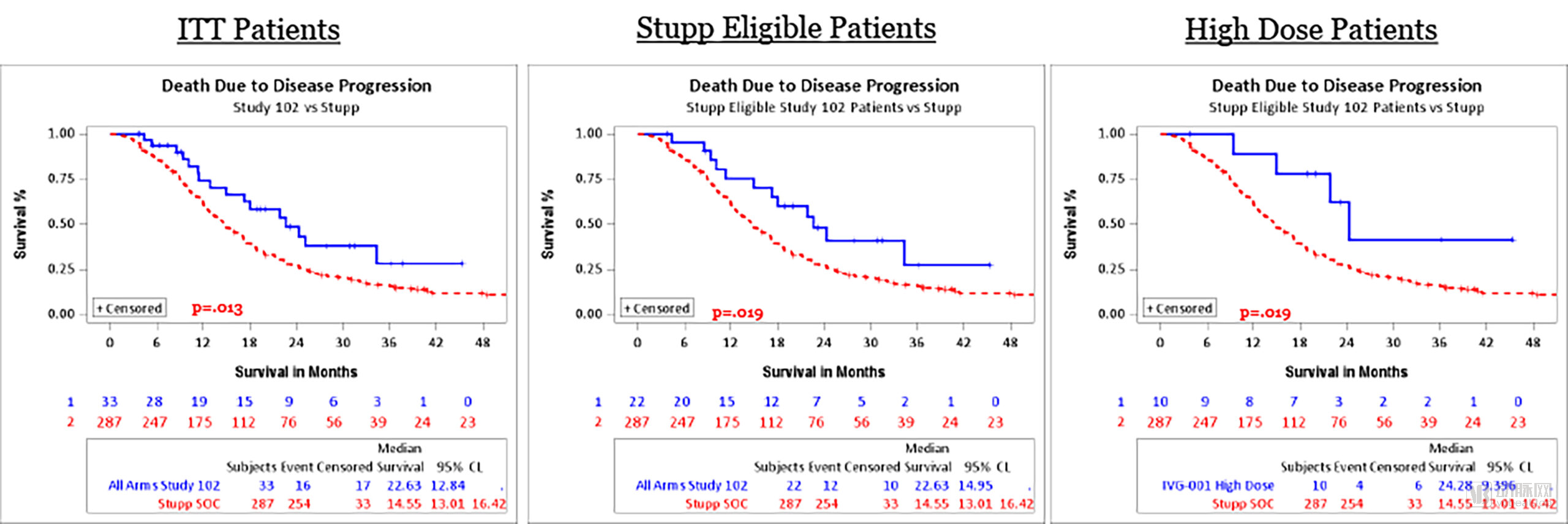
Imvax has completed its Phase Ib clinical trial and obtained compelling data. In the Phase Ib clinical trial, four doses of the vaccine were tested in 33 patients with newly diagnosed glioblastoma.Following vaccination, the patient received standard treatment, namely radiotherapy and chemotherapy (with the drug temozolomide).
The study found that in 33 patients, nearly half experienced halted tumor growth. Patients receiving higher doses had a median overall survival seven months longer than that of historical controls (22 months vs. 15 months) and more than three months longer than that of the control group without cancer progression (compared to seven months).
The most striking figures came from a cohort of patients with specific mutations predictive of a better response to temozolomide. In the historical control group, survival among these patients was three times longer than that of patients with such mutations, and their cancer did not progress.
Current Research Status at Home and Abroad
Traditional treatment for glioblastoma involves surgical resection to remove as many tumor cells as possible; however, the diffuse nature of glioblastoma makes complete eradication difficult, particularly when the tumor is located near critical brain regions responsible for functions such as language, motor control, or coordination. Although postoperative radiotherapy and chemotherapy can reduce residual tumor burden and address inoperable lesions, they remain curative insufficient. Mortality rates remain high, with a median survival time of 12–15 months.
Both domestic and international companies and researchers are conducting studies on glioblastoma, with some vaccines still in the clinical trial phase. For example,Results from a Phase I/Ib trial published in Nature in 2018 demonstrated that treated patients generated circulating, multifunctional neoantigen-specific CD4+ and CD8+ T-cell responses.This is a neoantigen generated by tumor-specific protein-coding mutations. Such antigens do not induce central tolerance, can elicit potent immune responses, and function as genuine antigens that promote tumor rejection.
The Mayo Clinic in the United States has developed a dendritic cell vaccine, whichDendritic Cell Vaccines Yield Satisfactory Results in Preliminary Clinical Trials for Newly Diagnosed Glioblastoma. Mayo Clinic is currently conducting a Phase II clinical trial.
The world’s first tumor treating fields device, Optune®, has officially been launched in mainland China for use in combination with temozolomide to treat patients with newly diagnosed glioblastoma, and as a monotherapy for patients with recurrent glioblastoma.
From the current perspective, research on glioblastoma is ongoing. After announcing its Phase Ib clinical trial data, Imvax secured Series B financing in the same year and has raised $112 million this year to accelerate its research progress. Based on Imvax’s funding activities, investors have begun to pay attention to the development of glioblastoma vaccines.