Successful Practice Seminar on DRG Payment Reform Pilot in Meishan City: Achievements and Insights
2019 marked the tenth year since the launch of China’s new healthcare reform. While internet-enabled tiered diagnosis and treatment progressed steadily, the burden of medical insurance payment remained an unavoidable challenge. In October of that year, the National Healthcare Security Administration issued the technical standard “National Healthcare Security DRG (CHS-DRG) Grouping Scheme.” This official template brought uniformity to the previously fragmented landscape of Diagnosis-Related Group (DRG) classifications, cementing DRG as the definitive basis for medical insurance reimbursement.
Against this backdrop, Meishan City actively responded to the call and partnered with Shanghai Kingstar Winning Software Science and Technology Co., Ltd. (hereinafter referred to as “Winning Health”) to launch a Sichuan provincial pilot project. Starting in the second half of 2018, simulated DRG grouping and settlement were conducted for 15 medical institutions in 2018. In 2019, Meishan City adopted its own DRG grouping scheme, under which year-end settlements for secondary-level medical institutions across the city were based on monthly DRG prepayments. In 2020, it took the lead in adopting the CHS-DRG grouping scheme issued by the National Healthcare Security Administration, achieving monthly DRG prepayments for all secondary-level medical institutions citywide by May. Now that more than a year has passed, it is time to summarize the implementation outcomes. On August 28, 2020, the Seminar on DRG Payment Reform Pilot Practice (Meishan City), combined with the Leadership Training Session for DRG Pilot Hospitals in Luzhou City and the 2020 Annual Academic Conference of the DRG Expert Committee of the Sichuan Hospital Management and Development Research Center, was successfully held at the Dongpo International Hotel in Meishan, Sichuan Province, aiming to evaluate the phased effectiveness of the DRG pilot implementation.
At the event, more than 100 participants from healthcare security administrations and hospitals in Southwest China, along with representatives from Winning Health Technology Group, attended the seminar. During the conference, multiple experts exchanged insights on their respective hospitals’ DRG system implementation, discussed various challenges encountered in current DRG practice, and effectively facilitated the pilot rollout of DRG in Southwest China, including hospitals in Meishan City.
Peng Meihua, Associate Professor and Director of the Medical Insurance Teaching and Research Section at the School of Management/Health Sichuan Research Institute of Chengdu University of Traditional Chinese Medicine, kicked off the conference with a presentation titled “Analysis of the Effectiveness Rating of DRG Payment Reform in Meishan.” He stated that since the state comprehensively promoted the establishment of a diversified and composite medical insurance payment system dominated by diagnosis-related group (DRG)-based payments in 2017, DRG has officially moved from the background to the forefront. Meishan City closely followed national policies to implement DRG payment reform. Taking the 2019 DRG grouping scheme as an example, Meishan City had established 1,280 DRG groups. The grouping results showed that 1,169 refined DRG subgroups had a coefficient of variation (CV) of less than 1, accounting for 97.03% of the total number of groups, while DRG groups with a CV of less than 0.5 accounted for 51.78%. This demonstrates that the localized DRG grouping scheme in Meishan is scientifically sound.
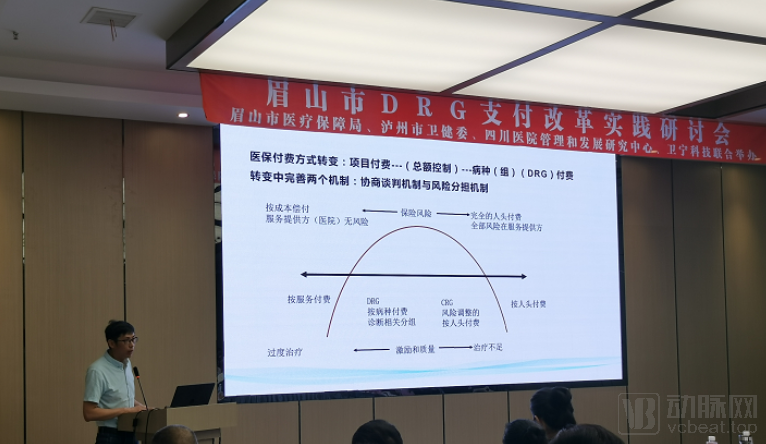
Mao Yuchen, Deputy General Manager of Shanghai Kingstar Winning Software Science and Technology Co., Ltd., discussed how diversified health insurance payment methods facilitate refined hospital management. He stated that to meet the demands of payment reform across hospitals in various regions, Winning Health Tech provides multi-payment support—including DRG—built upon its existing fee-for-service billing infrastructure. Regarding DRG, the product currently supports case grouping tools, refined processing of historical data and data quality, fund and budget simulation calculations, integrated settlement and fund management, dynamic fund simulation forecasting, as well as functions for healthcare service performance evaluation and medical quality management under various payment models.

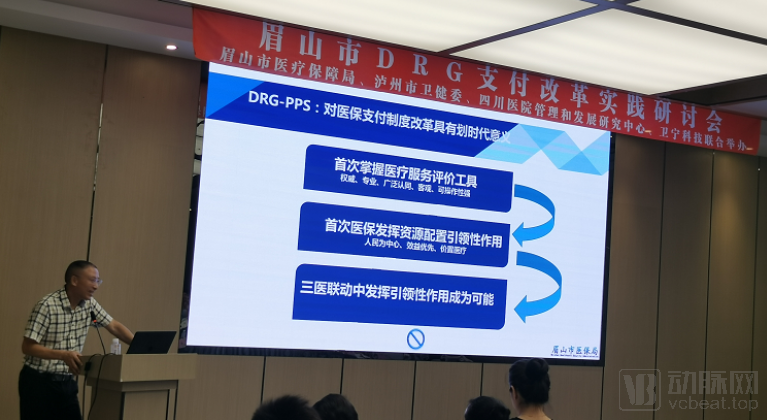
Chen Jianming, Director of the Meishan Medical Security Affairs Center and Member of the Sichuan Province Diagnosis-Related Groups (DRG) Payment Expert Group, discussed DRG-PPS and the construction of a medical insurance governance capability system, summarizing the phased work on DRG-PPS in Meishan. He stated that hospitals must pursue refined management and promote the development of DRG; if DRG is implemented effectively, future payment methods will no longer pose challenges. However, during the DRG implementation process, he observed that DRG payment reform is a systematic project. Reforms should be deepened, rather than relying long-term on temporarily assembled teams or outsourced services. It requires the concerted efforts of numerous professionals in medical insurance, clinical practice, medical statistics, medical records, and hospital management. Therefore, he proposed three key recommendations: first, information system construction must adhere to standards; second, talent team development must have clear qualifications and planning; and third, supporting reforms must be advanced synchronously.
Xie Xiaolong, President of Meishan Traditional Chinese Medicine Hospital, delivered a speech titled “Hospital Transformation in Response to New DRG Challenges.” He outlined the hospital’s one-year journey in implementing Diagnosis-Related Groups (DRG), demonstrating how healthcare administrators can identify operational issues at both the departmental and individual physician levels by comparing key metrics such as pharmaceutical cost proportion, consumable cost proportion, and Case Mix Index (CMI). He emphasized that “cost accounting for day surgery must be precise down to each medication and each consumable item.” Under this incentive mechanism, the hospital has achieved year-on-year reductions in average cost per visit, average consumable cost proportion, and average pharmaceutical cost proportion, alongside a rapid increase in CMI. Notably, the average length of stay decreased from 10.62 days in 2018 to 9.14 days currently. Through internal DRG-based performance management, Meishan Traditional Chinese Medicine Hospital has significantly improved its operational efficiency.

Li Liyong, Director of the Department of Medical Information at the Hospital Management Research Institute of West China Hospital, Sichuan University, began with the U.S. DRG model and subsequently discussed DRG reforms in Germany, Australia, and the Taiwan region. The successful implementation of DRG-based payment systems worldwide offers valuable insights for China’s current explorations, while their underlying connotations warrant further joint exploration by experts and scholars.
Wang Xiaodong, Director of the Management Consulting Department at the Hospital Management Research Institute of West China Hospital, Sichuan University, highlighted the hospital’s transition from technology-led to management-led development by elucidating its new management model, emphasizing that refined management is now essential to meet the demands of the new era.
At the conclusion of the conference, Chen Bo, Director of the Big Data Center at the First Affiliated Hospital of Chongqing Medical University, delivered the closing remarks, addressing hospital performance appraisal and compensation under the DRG-based payment system. Currently, the First Affiliated Hospital of Chongqing Medical University adopts a performance appraisal and distribution model based on RBRVS and DRGs, which adheres to four core principles: separate evaluation by job categories, quantitative assessment of workload, key performance indicators (KPIs), and disease-mix structure orientation. He stated, “The introduction of DRGs will significantly impact hospital management philosophies; however, this transition is gradual, and it will take time for physicians and nurses to adapt.” Furthermore, he emphasized that DRG-based assessments should not rely solely on relative weights; the primary focus must remain on medical quality, with an unwavering commitment to ensuring patient safety.