Artificial Womb Breakthrough: A Promising Solution for Prematurity and Infertility
Author: Probe Capital
The concept of the artificial uterus was first proposed by British evolutionary biologist J.B.S. Haldane, who predicted that by 2074, approximately 70% of babies would be born through ectogenesis.
Currently, during female pregnancy, the fetus developing in the uterus exchanges substances with the mother through the placenta and umbilical cord to obtain nutrients and oxygen. The disc-shaped placenta has the umbilical cord attached to its fetal side, which connects to the fetus, while its maternal side attaches to the mother’s endometrium. The placenta contains numerous villi, within which capillaries communicate with the blood vessels in the umbilical cord. The fetus produces its own blood, which flows through the umbilical vessels to the placenta. The intervillous spaces are filled with maternal blood. Substance exchange between the fetus and the mother occurs across the placental villi; fetal waste products pass through the trophoblast layer into the maternal bloodstream and are ultimately eliminated from the mother’s body.
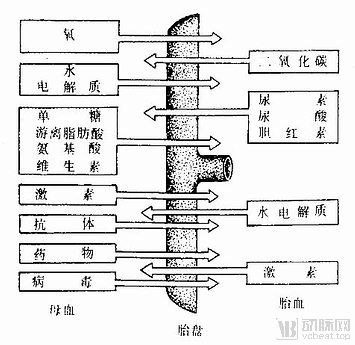
Figure 1. Placental Circulation. Image source: Internet.
Ideally, artificial wombs incubate fetuses in sterile fluid that mimics the intrauterine amniotic environment, featuring a circulatory system for blood flow and gas exchange driven by an innate fetal circulation analogous to the umbilical-placental system, thereby supplying nutrients and oxygen to the fetus while simulating the sterile, warm, and elastic conditions of the natural uterus.
Artificial wombs hold significant implications in the short, medium, and long term.
In the short term, artificial wombs aim to improve the survival rates and quality of life for premature infants by simulating the conditions of a natural uterus. As of 2020, prematurity was the leading cause of neonatal mortality worldwide. Specifically, more than 70% of preterm births occur between 34 and 36 weeks of gestation. Among the remaining preterm infants, those born before 22 weeks of gestation have virtually no chance of survival; infants born at 22–23 weeks have a survival rate of only 0.07%; approximately one-third of infants born at 23 weeks survive; and after 24 weeks, the likelihood of survival doubles, with the survival rate rising to approximately 60%.

Figure 2. Mortality Rate in Preterm Infants
Currently, specialized neonatal intensive care units (NICUs) are available to treat preterm infants through interventions such as pharmacotherapy, mechanical ventilation, fluid and electrolyte management, and surgical procedures, thereby improving outcomes for preterm births; however, success rates remain limited. The respiratory, nervous, and digestive systems of these surviving preterm infants are not yet fully developed.
Further studies have indicated that existing treatment modalities can further impair pulmonary development and may even lead to heart failure. Most survivors experience common complications, particularly among preterm infants born at 22–28 weeks of gestation; complications are virtually inevitable in those born before 26 weeks. Approximately 80% of these preterm infants develop at least one major comorbidity, such as pulmonary disease, cerebral palsy, or hearing and visual impairments.
Furthermore, treatment costs are a significant concern that cannot be overlooked. Neonatal intensive care unit (NICU) stays are expensive; in the United States, for example, the average daily cost per premature infant in the NICU exceeds $3,000, and prolonged stays can surpass $1 million. This places parents of infants born at 23 weeks’ gestation in the position of having to make difficult decisions. The emergence of artificial wombs has the potential to improve outcomes for these premature infants, thereby alleviating the emotional distress experienced by their parents.
In the medium term, artificial wombs can address the reproductive challenges faced by patients with infertility. Globally, approximately 8%–12% of the population of reproductive age is affected by infertility; in China, this figure exceeds 40 million and continues to rise year by year.
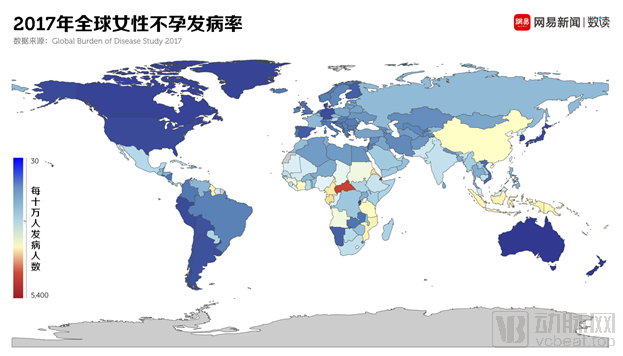
Figure 3. Global Prevalence of Female Infertility in 2017. Source: NetEase News
Currently, 10%–20% of patients seek assistance from assisted reproductive technologies (ART), such as artificial insemination or in vitro fertilization (IVF). In contemporary society, the fertility intentions of women of childbearing age have declined due to life stress and financial costs. By the time some women have accumulated sufficient wealth, they have often missed their optimal childbearing years. In China, the fertility rate among advanced maternal age women has risen significantly.
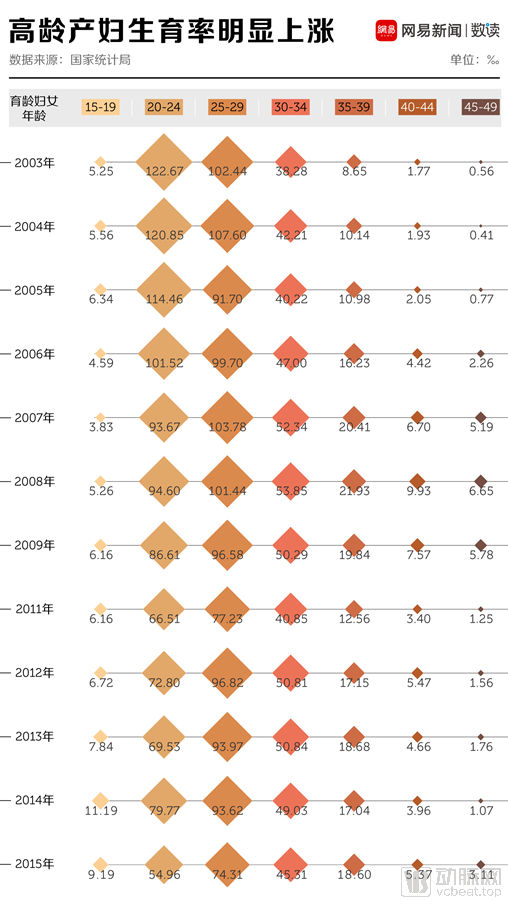
Figure 4. Fertility Rates Among Women of Different Age Groups, 2013–2015. Source: NetEase News
However, the success rates and live birth rates of assisted reproductive technology (ART) in women of advanced maternal age are significantly reduced. Statistics show that ART success is strongly correlated with patient age. Compared to patients under 35 years old, the live birth rate for those aged 38–40 decreases by 50%, while for patients over 44, it drops to just 1%. Therefore, assisted reproductive technology is not a panacea.
Uterine transplantation represents another therapeutic option. Although the uterus exhibits a relatively weaker immune rejection response compared to other organs, donors are predominantly the recipients’ mothers or other relatives, thereby raising significant ethical controversies. From a technical perspective, uterine transplantation presents considerable challenges in the selection, harvesting, and anastomosis of blood vessels. Furthermore, postoperative vascular narrowing may occur, potentially leading to gestational hypertension and fetal growth restriction.
In January 2019, China saw the birth of its first baby conceived through uterine transplantation followed by embryo transfer, indicating that the surgical technique for uterine transplantation has not yet reached full maturity. Furthermore, at the current stage, uneven distribution of medical resources and the lack of insurance coverage make the entire process prohibitively expensive, thereby limiting the clinical application of uterine transplantation in assisted reproduction. The emergence of artificial wombs may potentially address infertility among women of reproductive age and enable childbearing for women beyond their reproductive years.
In the long term, artificial wombs are expected to liberate women to a certain extent and promote gender equality in a broader social sense. The costs of natural pregnancy and semi-natural pregnancy are borne directly by women, and pregnancy has a significantly different impact on women’s lives and employment compared to men. Currently, many modern women choose egg freezing to delay childbearing; however, the success rate of achieving pregnancy after egg freezing is only 12%. Furthermore, both the egg retrieval process associated with cryopreservation and subsequent pregnancy continue to inflict physical harm on women.
Surrogacy is one such solution, but it is inherently a form of egregious class exploitation, directly commodifying the wombs of proletarian women for sale in the market. If fetuses could develop in industrial-scale artificial wombs, the unequal division of labor between men and women in reproduction could be broken, and women would no longer bear the costs of childbearing alone.
Looking back at history, reproductive technologies have continuously advanced, evolving from artificial insemination and gamete intrafallopian transfer to in vitro fertilization (IVF) and embryo transfer. Notably, the field has progressed from first-generation IVF with embryo transfer to third-generation preimplantation genetic testing (PGT), and most recently to the emergence of “three-parent babies.” This latest technique utilizes nuclear DNA from the father’s sperm, nuclear DNA from the mother’s egg, and mitochondrial DNA—which is independent of the nucleus—from the mother’s egg, thereby enabling women with mitochondrial defects to have healthy children. Throughout this process of technological iteration and advancement, public awareness and acceptance have steadily increased, as has confidence in mastering these technologies, laying a solid foundation for the future widespread adoption of artificial wombs.
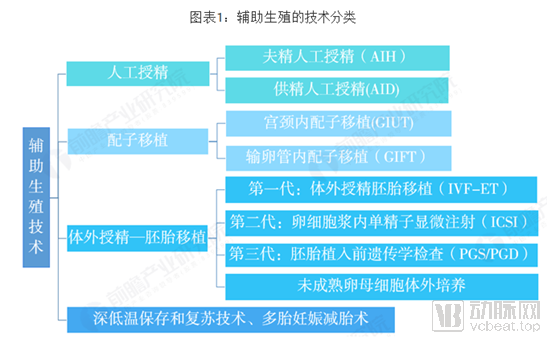
Figure 5. Classification of Assisted Reproductive Technologies (ART). Source: Compiled by Qianzhan Industry Research Institute
The prototype of the artificial uterus can be traced back to 1954, when Emanuel M. Greenberg and colleagues filed a patent for an artificial uterus. The designed device comprised a fetal chamber filled with amniotic fluid, a machine connected to the umbilical cord, a blood pump, an artificial kidney, and a water heater.
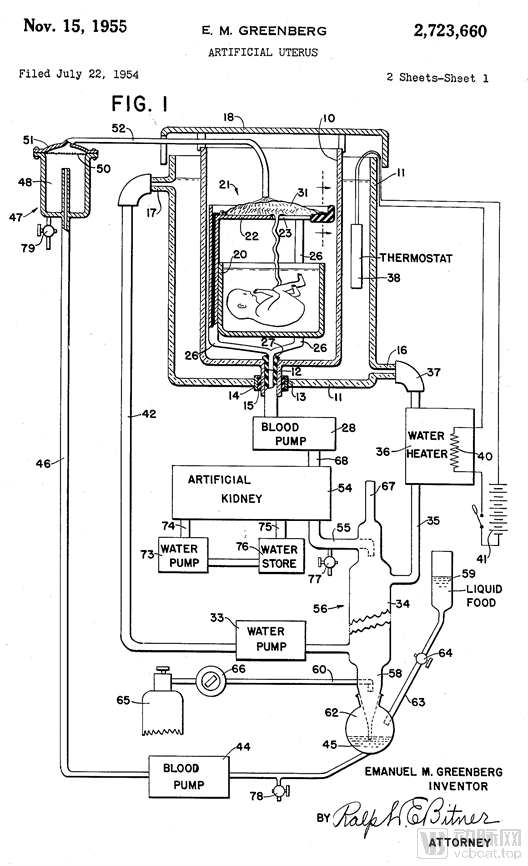
Figure 6. The First Artificial Womb Patent
In 1963, researchers placed aborted goat fetuses into an oxygen chamber filled with a water-like fluid. The fetal lambs were cannulated via the umbilical cord and perfused using a first-generation bubble membrane oxygenator, with total support durations ranging from 40 minutes to two days. These pioneering experiments ultimately proved unsuccessful, being limited by complications such as sepsis, circuit- and oxygenator-related issues, and heart failure.
In 1996, researchers at the University of Tokyo extracted a goat fetus that had developed normally for four months via cesarean section and placed it in an acrylic chamber filled with amniotic fluid. The fetal umbilical cord was connected to an artificial placenta. Most of the fetuses died because the mechanical pump damaged their fragile cardiopulmonary systems. A few survived in the system for three weeks, but all of them suffered from complications, malformations, or lung injury. The experiment ultimately ended in failure.
In recent years, various countries have allocated research funding to support bionics research. Notably, in October 2019, the European Union’s Horizon 2020 programme specifically earmarked €2.9 million (approximately RMB 23.2 million) to fund research on artificial wombs.
The Future of Artificial Wombs Depends on Advances in Bioengineering and Materials Science: Better Mimicking the In Utero Environment Is the Key Direction, with the Following Components Currently Required:
1. Artificial Placenta: The artificial placenta is an extracorporeal membrane oxygenation (ECMO) system more suitable for neonates or preterm infants. It is a novel technology designed to rescue critically endangered fetuses, allowing them to remain in an environment akin to that of the uterus.
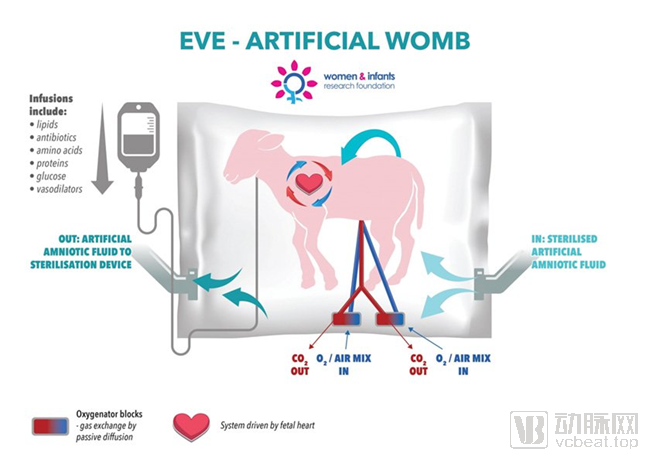
Figure 7. Schematic Diagram of an Artificial Placenta
Earlier oxygenators’ resistance and pump-supported circuits could cause preload or afterload imbalance in the fetal heart, leading to progressive circulatory failure. Current oxygenation technologies have seen substantial improvements, enabling the extension of extrauterine fetal life support to several weeks by employing conventional pump-driven ECMO circuits. However, this approach remains ultimately limited by circulatory overload and heart failure. In artificial womb systems, the ideal gas-exchange interface allows the fetus to maintain circulation similar to that of an intact fetoplacental unit, with oxygenator perfusion determined by fetal cardiac output. Therefore, research focuses on novel circuit designs. Typically, pumpless circuits are combined with low-resistance oxygenators to mimic normal placental circulation as closely as possible. Compared with traditional ECMO technology, simplified, compact pumpless arteriovenous circuits offer several advantages, including reduced priming and distribution volumes, shorter blood exposure time to thrombogenic surfaces, and the potential for more physiological regulation of blood flow and systemic pressure mediated by the fetal heart itself.
Although pumpless systems have been accepted as the ideal technology for preserving fetal physiology, animals in experimental models still develop symptoms such as metabolic acidosis and progressive hypotension. These systems fail to replicate normal fetal pulmonary physiology or maintain normal fetal circulation.
2. Construction of the Biobag: The fetus must survive within a single-use, fully enclosed biobag. Any liquid contamination could lead to fetal pulmonary infection; therefore, the design process must address sterility, dimensional adaptability, and spatial and fluid volume efficiency as much as possible. Typically, the biobag is semi-transparent to facilitate better monitoring of the fetus. Additionally, the biobag features various ports, such as an umbilical cord inlet and an oxygenator circuit inlet. It is also equipped with temperature probes and sterile tubing to enable continuous amniotic fluid exchange and provide all necessary water and nutrients. Cannulas serve as the “umbilical cord,” delivering required nutrients and oxygen into the fetal bloodstream. This mimics normal placental circulation, ensuring adequate oxygenation and safe blood pressure. After cannulation, the biobag is sealed and transferred to a mobile support platform equipped with temperature and pressure regulation, padding, reservoirs, and fluid exchange circuits.
3. Construction of Subphysiological Circulatory Flow: Normal placental blood flow is 150–200 mL/kg/min. However, when carotid artery cannulation is employed, inherent limitations of carotid blood flow restrict us to achieving only 70–100 mL/kg/min. This necessitates numerous non-physiological compensations to match oxygen delivery with oxygen consumption. These measures include transfusing adult blood to achieve higher hemoglobin levels, maintaining elevated post-membrane PaO2, and administering sedatives to reduce fetal oxygen consumption. Furthermore, surgical procedures in the fetus for cannula placement and removal, secondary ligation of the common carotid artery, and their potential impacts on cerebral blood flow and brain development may also pose risks of impaired angiogenesis.
If umbilical vessels are used, they may undergo vasospasm, vascular erosion, or aneurysmal degeneration. Furthermore, entry into the central circulatory system via the umbilical vessels increases circuit resistance, thereby impeding physiological flow within the circuit. Additionally, due to the tortuosity of human umbilical arteries, it is not feasible to advance a large-bore catheter into the aorta without significant risk. Recent advances involve maintaining a certain length of the natural umbilical cord between the catheter tip and the abdominal wall. This approach minimizes the likelihood of umbilical cord occlusion caused by kinking or angulation, prevents any deterioration of the umbilical vessels, and, most importantly, allows for true physiological “placental” blood flow. Umbilical cord cannulation can provide stable support for extremely preterm lambs (at 105–110 days of gestation) for up to four weeks. These animals exhibit circulatory flows equivalent to normal physiological placental flow, grow within expected standard ranges, and receive adequate oxygen delivery to support organ maturation. Daily echocardiography confirms well-maintained fetal cardiac circulation, with good myocardial contractility and function.
In recent years, scientists have been continuously attempting to construct artificial wombs, with the main progress achieved being:
In 2001, Dr. Hongqing Liu, a Chinese-American professor at Cornell University, pioneered research on artificial wombs. She cultured single-layer human tissue using human endometrial cells to initially construct an artificial womb model: a uterus-shaped scaffold was fabricated from biodegradable collagen and chondroitin, onto which endometrial cells were seeded. After a period of culture, the scaffold naturally degraded, allowing the endometrial tissue to develop into a simplified artificial womb. This artificial womb supported the implantation of human fertilized eggs; however, due to ethical concerns, Professor Liu terminated the experiment on the sixth day after implantation. Subsequent mouse studies confirmed that while this simplified artificial womb could facilitate embryo implantation, it was far insufficient to sustain normal subsequent embryonic development.
In April 2017, the Children's Hospital of Philadelphia (CHOP) in the United States utilized an external artificial womb system with goat fetuses. The fetuses were placed in sealed bags filled with synthetic amniotic fluid, with their umbilical cords connected to machines outside the bags via three cannulas to promote growth and prevent infection. This device featured a pumpless arteriovenous circuit; during the trials, an extracorporeal membrane oxygenation (ECMO) system was employed to provide circulatory support, fully simulating the intrauterine environment and allowing the fetal lamb’s own heartbeat to drive blood circulation. By relying on a closed fluid environment with continuous fluid exchange and umbilical venous vascular access rather than mechanical pumps to facilitate fetal blood circulation, the system supported premature lamb fetuses ex utero for 28 days, setting a new record for extrauterine survival of fetuses. If such devices can be applied clinically, they will significantly improve the survival rates of premature infants.
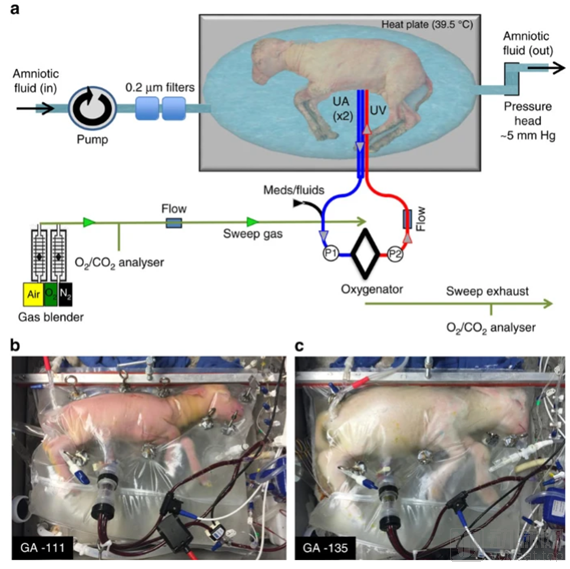
Figure 8. Preterm Lambs in an Artificial Womb
In 2019, Usuda et al. leveraged the Extra-uterine Environment (EVE) system to implement four improvements upon their 2017 biobag study, aiming to push the boundaries of survival for preterm infants:
(1) The circuit volume was reduced from 70 mL to 50 mL, and gas exchange was enhanced by incorporating a high-performance membrane oxygenator;
(2) A semi-closed system was adopted, featuring a small-volume synthetic amniotic fluid bath (reduced from approximately 35 L to 6 L);
(3) Frequently replace the bath components of synthetic amniotic fluid sterilized with ultraviolet light (every 6 hours);
(4) Discontinue the carotid artery and jugular vein catheters to alleviate pressure on the fetus.
This novel EVE platform can sustain lamb fetuses for longer durations with lower morbidity and mortality. By sealing prematurely born lambs (equivalent to 24 weeks of human gestation) in a warm amniotic fluid bath within sterile plastic bags and facilitating gas exchange via membrane oxygenators connected to umbilical vessels, the system maintained viability for up to 120 hours, demonstrating the feasibility of extro utero environment therapy in prolonging survival for late-preterm infants.
Although the EVE study reported a survival rate of 87.5%, limitations and uncertainties remain. For instance, autopsy findings revealed hydronephrosis with bladder distension and brain injury, and several subjects exhibited early signs of hepatic dysfunction.
In 2020, the Wake Forest Institute for Regenerative Medicine (WFIRM) in the United States announced that uterine tissue engineered using bioengineering techniques successfully repaired rabbit uteri, enabling them to give birth to live offspring. The researchers developed a biodegradable polymer scaffold to construct the uterus and seeded it with autologous cells for in vitro culture. Cells were harvested from the uterine structure of each rabbit to cultivate regenerative uterine tissue and seed the scaffolds. Six months after scaffold implantation surgery, the rabbits naturally mated with fertile male rabbits. Experiments demonstrated that six months post-implantation, the tissue-engineered uteri developed structures similar to native tissue, including luminal and glandular epithelium, vascularized mucosa, and a bilayered myometrium. Although the endometrial thickness of the artificial uterus was less than that of a normal uterus, the density of endometrial glands and the number of newly formed blood vessels were comparable to those in normal uteri. Among the three experimental groups, only the rabbits implanted with cell-seeded scaffolds successfully achieved pregnancy, carried to term, and delivered live offspring.
However, there is still a long way to go before artificial wombs can be used for human infants, as significant technical challenges remain.
First, the current state-of-the-art EVE platform for artificial wombs uses lambs as test subjects. Given the significant physiological differences between lambs and humans, it is essential to conduct physiological testing on primates and other species before proceeding to human trials.
Secondly, there are significant differences in the size and development of fetuses at different gestational weeks. Size differences are critical because a smaller infant has a lower blood volume. If insufficient blood flows through the artificial womb’s circuitry, thrombosis will occur. Even if the device could support lower blood flow rates, it would still be impossible to connect it to such a small infant. The cannulae of the artificial womb must be connected to the infant’s blood vessels; however, the smaller the infant, the smaller their vessels. If the vessels are not large enough, stable cannulation cannot be achieved. Overall, the diameter of infant blood vessels limits the development of artificial wombs. For neonates born at 22–24 weeks of gestation, who currently have low survival rates, existing technology may still be unable to utilize artificial wombs. For infants born after 24 weeks, whose natural survival rate already reaches 60%, it remains uncertain whether artificial wombs would provide any additional benefit.
With further technological development and application, the cost of artificial wombs has decreased, transforming them into industrial-grade production equipment. This makes them accessible to a growing number of people, thereby alleviating parental responsibilities to some extent. Modern societal standards for childbearing and rearing impose higher demands on parents, bringing greater social and economic pressure. The reproductive and parenting practices of agrarian societies are not necessarily suitable for modern times, making socially supported reproduction a viable option worth considering. However, this may attract public criticism, with concerns that industrial-scale artificial wombs represent an erosion of family rights by the collective, driven by technological advancement.