How WangHaiKangXin Empowers Hospitals to Rapidly Respond to DIP Implementation
On October 19, 2020, the National Healthcare Security Administration (hereinafter referred to as the “National HSA”) issued the Notice on the Work Plan for Pilot Programs of Regional Point-Based Global Budgeting and Diagnosis-Intervention Packet Payment (hereinafter referred to as the “Pilot Work Plan”), proposing to implement pilot programs for diversified composite payment methods in selected cities, combining regional healthcare insurance global budgets with Big Data-based Diagnosis-Intervention Packet (DIP) payment.
The Pilot Work Plan also announced seven pilot initiatives, to be implemented in phases: regional global budget management, full coverage of inpatient cases, development of supporting settlement methods, establishment of a data center, strengthening of supporting regulatory measures, improvement of agreement management, and enhancement of professional technical capacity.
The release of the Pilot Work Plan has created a significant stir, drawing considerable attention due to its introduction of Big Data-based Diagnosis-Intervention Packet (DIP) payment. Prior to the National Healthcare Security Administration’s “Expert Forum on Big Data-based Diagnosis-Intervention Packet (DIP) Payment” held this July, the term DIP was largely unknown.
What Exactly Is DIP? How Does It Differ From DRG? How Should Hospitals Leverage Informatics to Address DIP? In Response to These Questions, Chen Xianli, Vice President of Beijing Dongruan Wanghai Technology Co., Ltd., Shared Her Insights in an Interview with VCBeat.
DIP (Big Data Diagnosis-Intervention Packet) is the abbreviation for a big data-based payment system by disease-specific point values. It is a method that expands disease group analysis through big data technology. This approach leverages comprehensive datasets to objectively reflect real-world clinical variations in diseases, performs exhaustive enumeration and clustering of diagnoses and treatment modalities within the data to rapidly form groups, and mines data insights to understand the objective patterns linking disease combinations with healthcare costs. It establishes quantitative standards for diseases and treatments, and defines pricing mechanisms based on stochastic means, health insurance payment methods, and fund supervision models.
DIP and DRG are identical in essence and principle, as both involve grouping cases according to specific principles. Simply put, the primary difference between DIP and DRG lies in their grouping methodologies. DRG classifies cases into several related groups based on comprehensive factors such as patient age, gender, length of stay, clinical diagnosis, surgical procedures, comorbidities, and complications, a process that requires substantial involvement from clinical experts. In contrast, DIP is based on full-sample, massive data to categorize all diseases and medical technologies, placing less emphasis on clinical factors and eliminating reliance on clinical experts.
DIP grouping is primarily based on anatomy and etiology, establishing a master catalog index for disease categories using major diseases and health issues reflected in the data, currently comprising approximately 129 groups.
Level 1 categories are grouped by similar disease diagnoses, totaling 1,194 groups; on this basis, different treatment modality groups are superimposed to form combinations of “disease diagnosis classification + treatment modality,” resulting in a Level 2 directory with approximately 3,000 groups.
Finally, building on the secondary directory, big data analytics are used to combine each diagnosis with various treatment modalities, generating a combined directory of disease diagnoses and treatment approaches. Statistical methods and clinical expertise are then applied to denoise the data. Currently, there are approximately 16,000 core disease–treatment combinations (out of roughly 500,000 total groups).
The greatest advantage of the Big Data Diagnosis-Intervention Packet (DIP) is its efficiency, as grouping results can be obtained immediately through big data computation. Due to the highly granular combination of "diagnosis + treatment" categories, DIP achieves an exceptionally high case-mix index coverage rate. In 2018, Shanghai implemented 763 Diagnosis-Related Group (DRG) categories with a coverage rate of 83.27%; in contrast, DIP utilized 12,248 groups, achieving a coverage rate as high as 97.41%. This indicates that DIP encompasses nearly all hospital cases. Meanwhile, the average coefficient of variation within DIP groups was only 0.834, significantly lower than the 1.012155 observed for DRGs during the same period. This implies that the intra-group heterogeneity in DIP is substantially lower than that in DRGs.
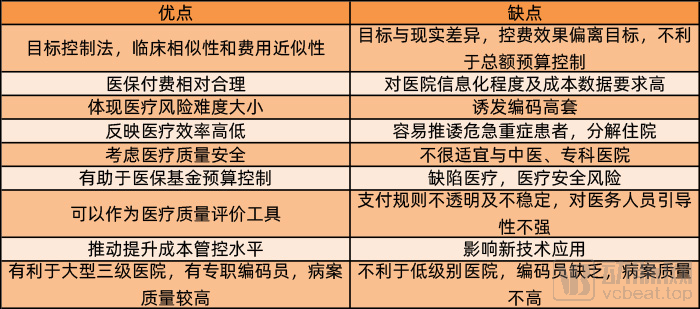
Pros and Cons of DRG
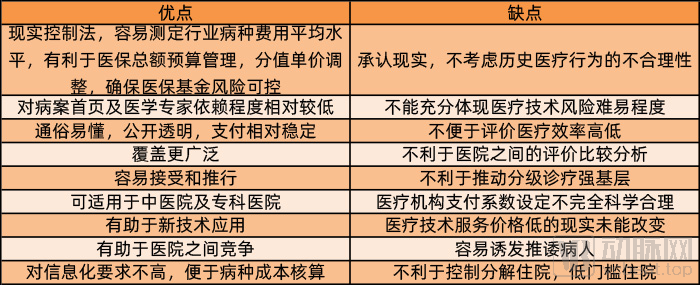
Pros and Cons of DIP
Payment by disease-specific point values is not a novel concept. It was implemented in China even earlier than Diagnosis-Related Groups (DRGs). The concept of disease-specific point values was first introduced during the healthcare reform pilot in Mudanjiang, Heilongjiang Province, in 2002.
Building on this foundation, cities such as Huai’an, Xiamen, and Zhongshan have also conducted their own explorations and practical applications of diagnosis-based point-value payment systems. However, Guangzhou was likely the first to apply big data technology to point-value payment. In early 2017, Guangzhou’s medical insurance payment system transitioned from single-disease payment to Diagnosis-Related Groups (DRG). That same year, Guangzhou launched a pilot program for Big Data Diagnosis-Intervention Packet (DIP), analyzing more than 8.5 million discharge summary records from 331 hospitals in the city. In early 2018, Guangzhou fully shifted from DRG to DIP. Shanghai subsequently implemented partial DIP trials in 2019.
From 2013 to 2015, Shanghai utilized the first four digits of ICD-10 codes to group diagnosis and treatment categories based on the face sheet information and case records of over 7 million inpatient cases across medical institutions at all levels and of various types, resulting in 6,139 disease groups. Furthermore, each disease group was classified according to the primary technologies employed, forming more than 180,000 disease-technology combinations.
“Overall, while DIP and DRG differ in grouping methodologies, data processing, and the extent of manual involvement, I personally believe that they share the same underlying philosophy and connotation regarding payment mechanisms. Both reflect the rational pricing and refined management of medical services by health insurance providers, shifting the payment model from a volume-based, fee-for-service approach to a value-oriented bundled payment system based on disease types or diagnosis-related groups.” This is how Chen Xianli summarized the similarities and differences between DIP and DRG.
Chen Xianli believes that, whether under the Diagnosis-Related Groups (DRG) or Big Data Diagnosis-Intervention Packet (DIP) system, the core concept is to implement bundled payment based on a complete clinical case or a disease group. This approach reflects the value-based purchasing of medical insurance funds and the behavioral orientation of medical insurance payment reform, which will have a significant impact on all stakeholders involved in medical practices.
First, hospitals will strengthen lean management. In the provision of medical services, diagnostic and treatment plans constitute the expenses and costs of care. Under a fee-for-service payment model, various services generate revenue for hospitals, leading to varying degrees of over-treatment. In contrast, under Diagnosis-Intervention Packet (DIP) or Diagnosis-Related Group (DRG) payment systems, where payments are bundled by disease category, materials, pharmaceuticals, and medical services all become costs borne by the hospital. Consequently, hospitals will inevitably strive to minimize resource consumption while ensuring the quality of medical care.
On the one hand, a series of measures gradually introduced by the National Healthcare Security Administration, such as the elimination of markups on drugs and consumables and volume-based centralized procurement, have led to a significant decline in the previously high prices of pharmaceuticals and medical consumables. This has reduced hospitals’ procurement costs for drugs and consumables, thereby substantially alleviating the operational pressure on hospitals under the Diagnosis-Intervention Packet (DIP) bundled payment system.
On the other hand, strengthening hospitals’ own lean management capabilities can effectively reduce resource consumption. Beijing Dongruan Wanghai Technology Co., Ltd. has long been dedicated to lean management in hospitals. With the release of new policies, the company will focus its research and efforts on helping hospitals implement lean disease management. In Chen Xianli’s view, payment reforms such as DRG (Diagnosis-Related Groups) and DIP (Big Data Diagnosis-Intervention Packet) require hospitals to adopt lean management at the institutional, departmental, and disease-specific levels, rather than merely improving medical record quality control.

Beijing Dongruan Wanghai Technology Co., Ltd. Provides Cost-Optimization Solutions Based on Diseases
Regarding lean management at the disease-specific level, Chen Xianli cited an example: Beijing Dongruan Wanghai Technology Co., Ltd. assisted a hospital in optimizing its diagnosis and treatment protocols for thyroid tumors by analyzing data from over 500 thyroid tumor cases treated within a six-month period. The analysis revealed that the average cost per case exceeded RMB 20,000, resulting in total expenditures of more than RMB 10 million.
Through systematic analysis, Beijing Dongruan Wanghai Technology Co., Ltd. proposed optimized diagnostic and treatment protocols for hospitals. These protocols extensively applied statistical methods and mathematical models, while incorporating insights from clinical experts in relevant disease areas. Under the premise of ensuring medical quality and enhancing patient care experience, the solutions achieved rational adjustments in resource utilization and treatment plans.
“When Beijing Dongruan Wanghai Technology Co., Ltd. assists hospitals in implementing lean management for primary disease categories, it systematically analyzes each disease type. This process not only breaks down the analysis to evaluate diagnostic and treatment quality, expenses, and costs at the disease level, but also examines individual physicians’ clinical practice patterns, as well as the quality and cost structure of the cases they manage. By integrating patient characteristics, applying health economic analytical methods, leveraging big data processing technologies, and referencing disease-specific resource consumption models, we cluster and optimize diagnostic and treatment protocols. The optimized protocols are then refined through consultation with clinical experts, ultimately forming disease-specific diagnostic and treatment plans that meet quality standards and ensure rational resource utilization, which are subsequently implemented in clinical practice.” Chen Xianli expresses strong confidence in Beijing Dongruan Wanghai’s specialized disease lean management solution.
This confidence stems from the significant impact of the protocol’s implementation. In cases of thyroid tumors, the optimized diagnosis and treatment protocol first lists the essential medications, consumables, and medical services required for the clinical pathway to ensure quality and safety. Meanwhile, it also provides optional alternatives for medications, consumables, and medical services that can reduce expenses and costs, thereby helping hospitals control expenditures and lower out-of-pocket costs for patients. According to calculations, if more than 500 thyroid tumor cases at the hospital were managed using the optimized protocol, total savings would exceed RMB 1.8 million, representing a cost-saving rate of 16.9%!
“DRG and DIP define bundled payment standards, and DIP also assists hospitals in conducting variance analysis of cost consumption across different disease categories. However, when costs exceed budgets, it is up to the hospitals themselves to determine how to optimize clinical pathways and achieve more rational resource utilization,” explained Chen Xianli. “Beijing Dongruan Wanghai Technology Co., Ltd. has long focused on hospital cost management, accumulating extensive models for resource consumption by disease category. Furthermore, we have developed a range of supporting tools and service cases to help healthcare institutions optimize disease-specific treatment protocols through rational resource utilization.”
Pharmaceutical and medical consumable manufacturers, as well as intermediaries—including those providing supporting services and logistics—will be significantly impacted by changes in hospital practices. On one hand, volume-based centralized procurement has drastically squeezed the profit margins of pharmaceutical and medical consumable companies. For firms that fail to secure bids in these procurements, survival itself may be at stake.
On the other hand, under the pressure of bundled payment systems, hospitals will re-evaluate pharmaceuticals and medical consumables to clearly distinguish between those that are essential and those that are optional. For the latter category, hospitals will inevitably adjust their utilization patterns based on health economic considerations, either replacing them with more cost-effective alternatives or designating them as backup options.
Chen Xianli believes that the impact of DRG and DIP on pharmaceutical and medical device companies may vary. DRG payment systems typically establish certain exceptions or compensation mechanisms to mitigate the impact of DRG on the adoption of new technologies, including drugs and consumables. In contrast, DIP adheres to the principle that "historical data is rational," calculating reimbursements based on historical data from periods before the emergence of new technologies. Therefore, to some extent, DIP may have a greater impact on the management of complex cases and the utilization of new technologies.
Chen Xianli believes that, whether under DRG or DIP, hospitals need to prepare for the following three aspects: medical record data quality, hospital- and department-level lean management, and disease-specific lean management.
First, hospitals need to strengthen the quality of medical record data and ensure accurate coding that truly reflects medical practices, as the information for DRG or DIP payment compensation and case grouping results is derived from the front page of the medical record. Meanwhile, 15 indicators in the performance assessment of public hospitals are directly sourced from the front page of the medical record; therefore, the quality of the front page of the medical record serves as a crucial data foundation.
Second, hospitals need to strengthen lean management at the departmental level and enhance cost control. Hospitals should accurately calculate costs by department, medical service item, and disease type, and incorporate cost control targets into their comprehensive budget management system. In conjunction with the hospital’s performance management scheme, this approach involves setting targets and standards in advance, implementing monitoring and control during operations, and conducting assessments and evaluations afterward.
Third, after achieving departmental cost control targets, hospitals should further advance to disease-level lean management. By integrating clinical pathways, they should optimize diagnosis and treatment protocols for specific diseases, including the optimization of pharmaceuticals, medical consumables, and medical service items. Furthermore, hospitals should coordinate internal resources and achieve interconnectivity of internal data, thereby implementing lean management at the source.
Chen Xianli stated that Wanghai Kangxin can assist hospitals in three areas. In the first area, the company helps hospitals achieve more accurate coding through tools and services such as intelligent coding and medical record quality control, thereby ensuring that cases—whether classified under DRG or DIP grouping systems—accurately reflect actual medical practices.
“Wanghai Kangxin’s intelligent coding tool is embedded within the electronic medical record (EMR) system. Leveraging big data and AI technologies, it provides intelligent coding recommendations during the diagnosis and treatment process based on patient characteristics, diagnoses, procedures, and other factors, while automatically generating information for the medical record face sheet. Upon confirmation by the medical records department and clinical departments, the final medical record face sheet is formed.” Chen Xianli stated that Wanghai Kangxin’s intelligent coding system is currently well-implemented in hospitals. It not only enables smarter and more precise coding, thereby improving the quality of medical records, but also enhances the operational efficiency of the medical records department.
In the second and third domains of lean management, Beijing Dongruan Wanghai Technology Co., Ltd. has been deeply engaged for many years and is an undisputed industry leader. Its research on disease-level lean management is both the earliest and most in-depth. “We have accumulated numerous models based on extensive prior experience, including clinical diagnosis and treatment models, resource consumption models, and others. These tools can help healthcare institutions achieve lean management at both the departmental and disease levels.”
The ultimate goal of healthcare insurance payment method reform is to achieve a balance among healthcare providers, patients, and insurers while controlling costs. Whether through Diagnosis-Related Groups (DRG) or Big Data Diagnosis-Intervention Packet (DIP), the core objective lies in transforming payment mechanisms to enhance cost containment. Despite any transitional challenges, hospitals’ immediate priority must be to strengthen their corresponding capabilities to effectively adapt to future healthcare insurance reforms.
Of course, this will pose new challenges to the current hospital management and operational models, while also raising higher demands for lean hospital management. Information technology vendors represented by Beijing Dongruan Wanghai Technology Co., Ltd. can leverage their expertise to assist hospitals through IT solutions, thereby empowering lean operations in China’s healthcare sector, promoting multi-party win-win outcomes, and jointly fostering the integrated development of the healthcare industry ecosystem, thus truly realizing the vision of serving healthcare and embracing forward-looking perspectives.
References
Xu Su: Big Data and the Reform of Healthcare Insurance Payment Methods
VBInsight: Saving Guangzhou’s Medical Insurance Fund RMB 1.1 Billion Annually—What Benefits Does Big Data-Driven DRGs Bring Beyond Cost Savings?