Breath Testing: From Odor-Based Diagnosis to Standardized Metabolomic Analysis
Author: Patrick/Miracle Light Blue Rainbow
The first use of breath analysis to determine human physiological status dates back to the Hippocratic era (460–370 BC), when ancient Greek physicians recognized that certain diseases could be diagnosed from the characteristic odors of patients’ breath and understood that breath could provide robust information about health status. In later medical practice, physicians were able to readily distinguish the “fruity” (acetone) odor in diabetic patients, the “musty” odor in those with advanced liver disease, the “fishy” odor in patients with renal failure, the “urinous” odor, and the “putrid” odor in individuals with lung abscesses.[1]. Analysis of volatile organic compounds (VOCs) present in exhaled breath can provide valuable information on patients' pathophysiological status, as these compounds serve as potential diagnostic biomarkers for various diseases and metabolic activities.
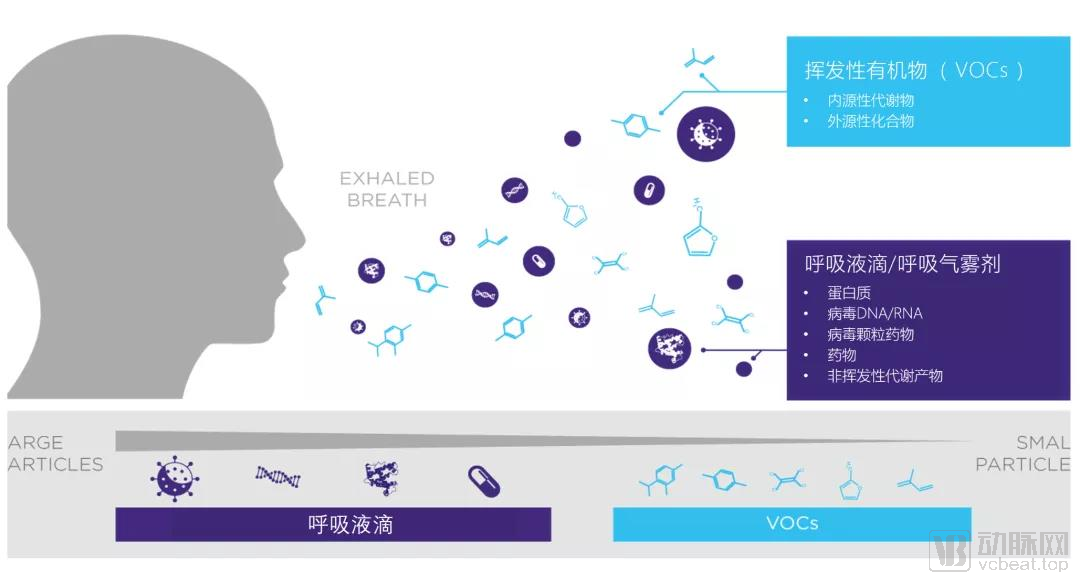
Figure 1. Schematic diagram of exhaled breath components. Source: Owlstonemedical.com
In recent years, the concept of breath metabolomics has been proposed. When the human body transitions from a healthy state to a pathological state, the distribution of volatile organic compounds (VOCs) in exhaled breath is altered, which can be detected and utilized for diagnosis and monitoring. Since the 1970s, when Pauling’s team used gas chromatography (GC) to detect more than 200 VOCs in human breath, an increasing number of research teams have been investigating breath metabolomics.
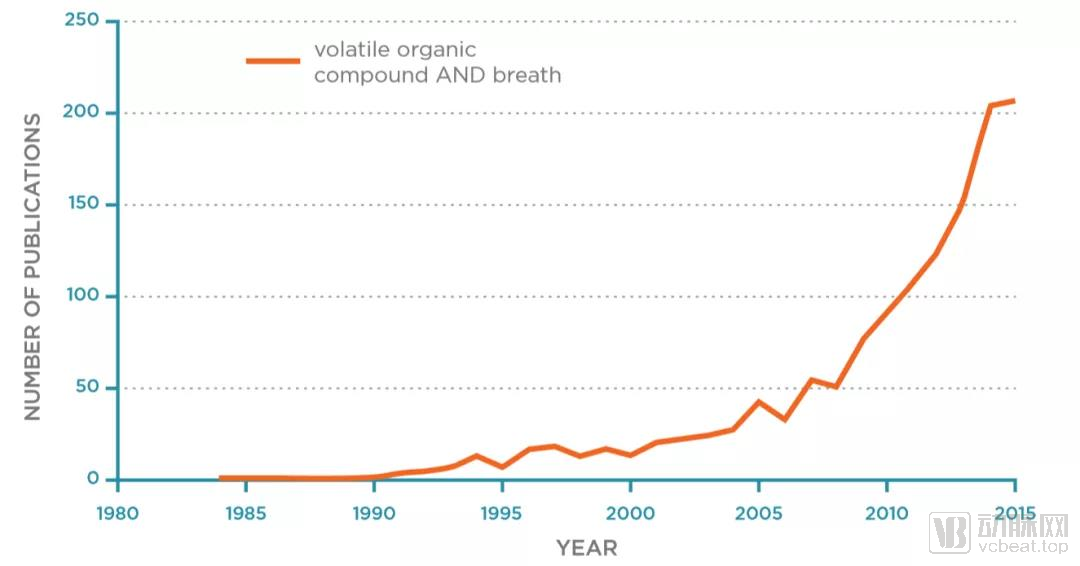
Figure 2. Statistics on the number of published articles on exhaled VOCs from 1980 to 2015. Source: Breath Biopsy Complete Guide
Sources of volatile organic compounds (VOCs) in exhaled breath include environmental factors (termed exogenous), the host (endogenous), and the microbiome (microorganisms residing in the oral cavity, lungs, and gastrointestinal tract). Among these, host-derived VOCs have been the most extensively studied in relation to clinical diseases. Exhaled VOCs used for diagnostic purposes primarily include:
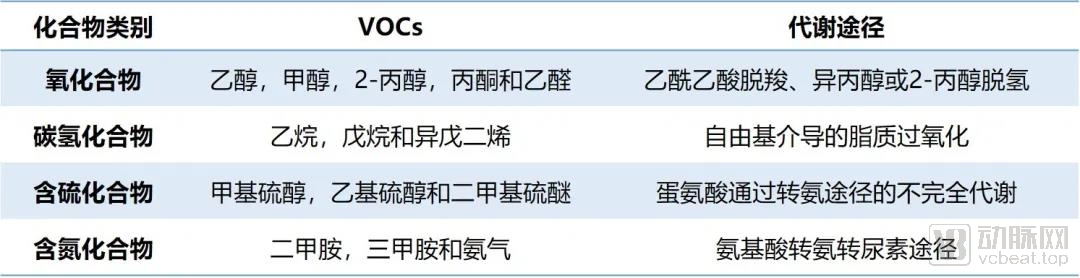
Table 1. Classification of Exhaled VOC Compounds[2]
Several breath tests utilizing volatile biomarkers have been established in clinical practice. However, due to the lack of reproducibility across studies aimed at identifying disease biomarkers, the application of VOC testing remains underdeveloped in clinical settings.

Table 2. Breath Tests Currently in Clinical Use. Source: Johns Hopkins Medicine; compiled by Miracle Light
During pathophysiological processes, alterations in cellular metabolism lead to changes in volatile organic compounds (VOCs), which are byproducts of biochemical reactions. Conditions such as hypoxia, excessive cell proliferation, heightened inflammation, reactive oxygen species activity, and other cancer-related pathological mechanisms can cause significant changes in the profiles and concentrations of both local and systemic VOCs. Biologists have proposed several potential biochemical pathway mechanisms. For instance, oxidative stress within the tumor microenvironment, driven by hypoxia or inflammatory diseases, contributes to the formation of alkanes and methylated alkanes. Overactivation of cytochrome P450 enzymes in cancer patients may elevate alcohol levels. Excessive cell proliferation induced by local hypoxia leads to anaerobic respiration, wherein the glycolytic pathway for energy production releases ketones and alcohols.
Numerous studies have also found a partial overlap between exhaled volatile organic compounds (VOCs) in lung cancer patients and VOCs from in vitro cell lines. This suggests that, in addition to VOCs directly released by cancer cells, secondary and/or systemic mechanisms associated with the disease itself also contribute to VOC production. This implies that VOCs, as biomarkers, can provide a more comprehensive assessment of the human body’s physiological and pathological status.[3]。
It is now known that 253 types of VOCs are associated with cancer diagnosis at different tumor sites. In most cases, these volatile organic compounds are primarily hydrocarbons (aromatic and aliphatic) and oxygen-containing compounds (i.e., aldehydes, alcohols, phenols, carboxylic acids, ethers, and furans), while compounds containing nitrogen, sulfur, and halogens are less common. Among them, the most commonly cancer-related VOCs include 2-butanone, 1-propanol, nonanal, isoprene, ethylbenzene, 4-methyloctane, 3-hydroxy-2-butanone, acetone, toluene, ethanol, pentanal, heptanal, and pentane.[4]。
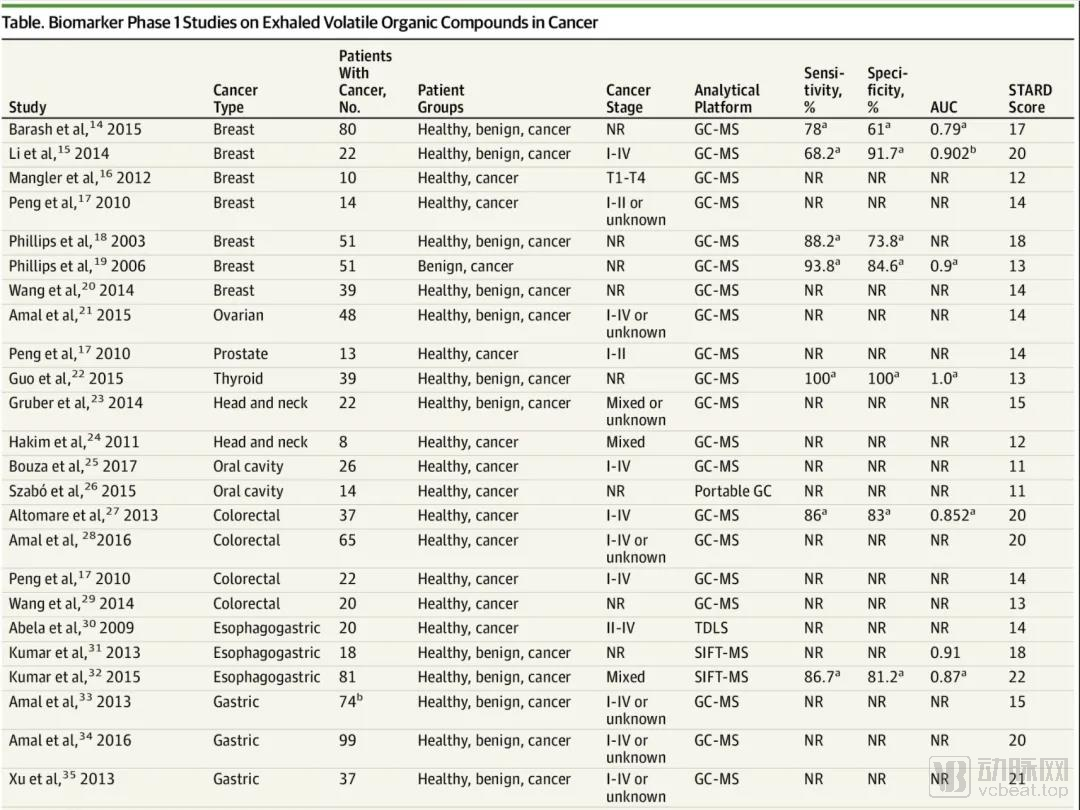
Table 3. Clinical Phase I Studies on Exhaled VOCs in Cancer Patients (Incomplete Statistics)[4]
Multiple studies have shown that detecting VOC fingerprint patterns or chemical groups in breath can distinguish individuals with microbial infections from healthy controls.[5]. Since unique metabolic products of bacteria cannot be produced by the human body, bacteria-specific volatile organic compounds (VOCs) can serve as biomarkers for diagnosis. For instance, six common pathogens associated with sepsis—Staphylococcus aureus, Streptococcus pneumoniae, Enterococcus faecalis, Pseudomonas aeruginosa, Klebsiella pneumoniae, and Escherichia coli—all produce isopentyl alcohol, formaldehyde, methanethiol, and trimethylamine. Furthermore, each of these bacterial strains produces its own specific VOCs: isovaleric acid and 2-methylbutyraldehyde for S. aureus; 1-undecene and 2-butanone for P. aeruginosa; and methanol, pentanol, ethyl acetate, and indole for E. coli.[6]。
There are currently many detection methods for pathogenic infections, each with its own advantages and disadvantages. Commonly used protein biomarkers for acute infection include C-reactive protein (CRP), procalcitonin (PCT), and serum amyloid A (SAA). The advantages of these tests are their speed and low cost; however, they cannot accurately identify the specific types of infecting pathogens. In contrast, emerging nucleic acid testing technologies, such as polymerase chain reaction (PCR) and metagenomic next-generation sequencing (mNGS), offer the benefit of accurate pathogen typing and analysis of antimicrobial resistance profiles, thereby providing better guidance for medication and prognosis. Nevertheless, factors such as longer turnaround times, complex and variable requirements for sampling and sample types across different infection categories, and higher costs significantly limit their comprehensive clinical adoption. Therefore, a breath test that is convenient, rapid, affordable, and capable of pathogen typing and identification possesses unique clinical advantages.
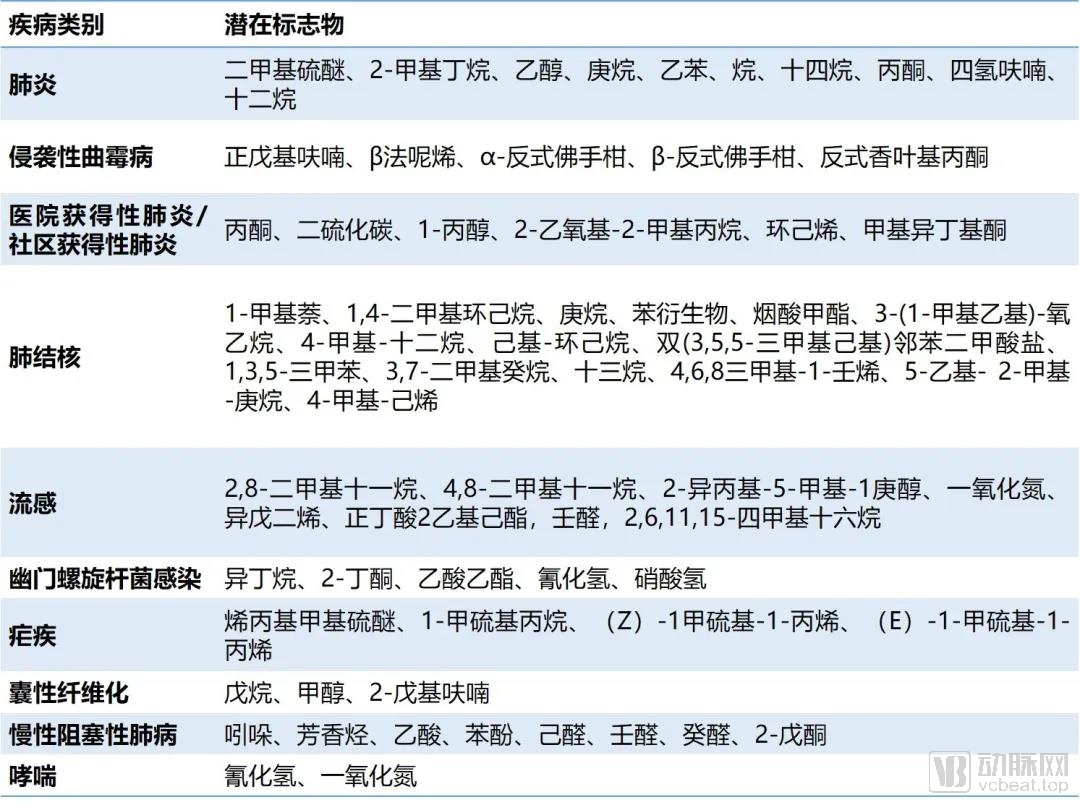
Table 4. Selected Infectious Diseases and Their Potential VOCs. Source: Miracle Light – Article Compilation
The interactions between endogenous VOCs from the host and symbiotic microorganisms greatly increase the complexity of the exhaled metabolome. Moreover, VOC concentrations in exhaled breath are typically extremely low, ranging from parts per million by volume (ppmv) to even parts per billion by volume (ppbv). Consequently, achieving reliable, high-quality, and standardized breath sampling and analytical detection poses considerable challenges.
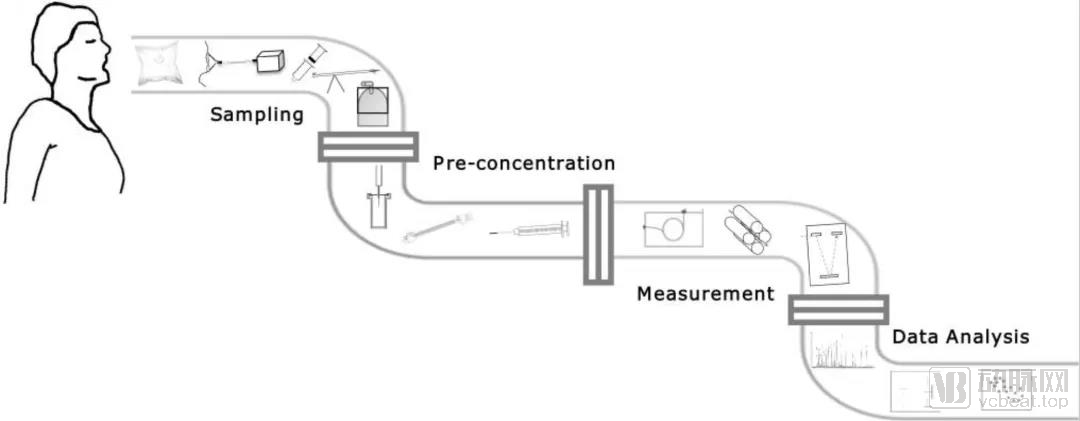
Figure 3. Exhaled Breath Collection Procedure[7]
Sample preconcentration methods and high-sensitivity analytical instruments are crucial. The core of sample collection is to capture endogenous gases free from environmental gas components, enabling precise analysis and avoiding interfering factors.
A single continuous exhalation based on CO2Capnography is divided into four phases: dead space ventilation, the transition phase of dead space and alveolar gas mixing, alveolar plateau, and end-expiratory phase. Compared with mixed sampling from Phase II and Phase III, sampling from Phase III is more representative and avoids false-positive results caused by the introduction of exogenous gases. The principle of sampling requires strict control of the procedure during respiratory sample collection to ensure reproducibility.
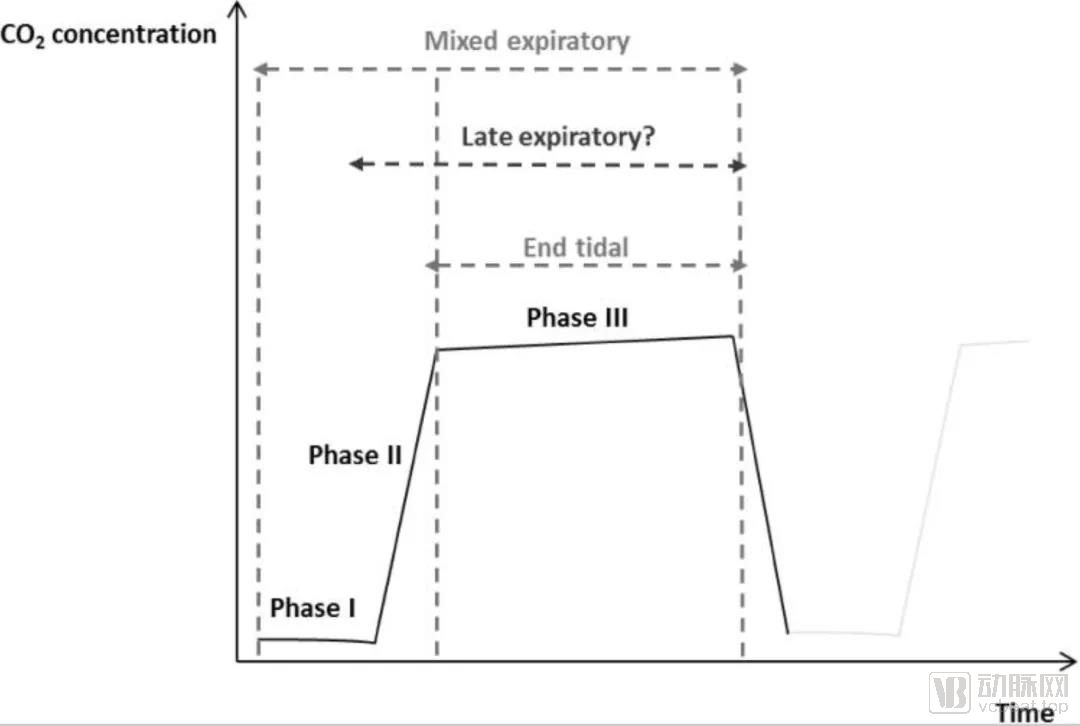
Figure 4. Time-Partial Pressure of Carbon Dioxide Waveform[7]
Due to the limitations of traditional analytical methods, pre-concentration of samples is required to improve analytical accuracy and, to some extent, reduce the significant losses incurred during separation and purification. Common methods for gas sample concentration include thermal desorption (TD) tubes and solid-phase microextraction (SPME).
Thermal desorption tubes utilize adsorbents to capture and enrich gases, which are subsequently released into detection instruments via thermal desorption. Commonly used adsorbents include Tenax TA & GR, Carbograph 5TD, and carbon molecular sieves (Carboxen). The selection of adsorbent materials is critical to prevent the loss of trace potential VOC markers due to excessive adsorption. However, regardless of volatility or polarity, the interactions between analytes and adsorbents at the packed interface inevitably affect reproducibility, thereby influencing compound recovery rates and potentially compromising stability during storage.
Solid-phase microextraction is a simple and effective solvent-free sample preparation technique that integrates all steps of conventional liquid-liquid extraction—including extraction, concentration, and transfer for detection—into a single device, thereby greatly simplifying the sample preparation process. It involves exposing a coated fused-silica fiber to the headspace of the sample, where analytes are directly enriched into the fiber coating using polydimethylsiloxane (PDMS) and polyacrylate (PA) as adsorbent materials, followed by coupled gas chromatography for the detection of volatile organic compounds (VOCs).[8]。
However, whether using adsorption columns or solid-phase microextraction, issues such as the selection of enrichment materials, high consumable costs, and adsorption losses are inevitable due to the enrichment process. These factors significantly affect the reproducibility of sample detection, thereby compromising the accuracy of the results. Highly sensitive online analytical instruments that do not require enrichment effectively address these challenges and represent a crucial factor in facilitating clinical application.
Currently, the most widely used system in scientific research is the high-sensitivity GC–MS analysis system. When combined with a pre-concentration system, it can effectively perform offline collection, separation, and identification of most compounds in human breath, such as aliphatic compounds, alcohols, aldehydes, ketones, amines, and halogenated compounds. It is also sensitive enough to quantify VOCs at the ppbv level. However, the time-consuming nature, high cost, losses during enrichment, operational complexity, inability to provide real-time detection, and challenges in achieving standardized reproducible measurements pose significant barriers to its clinical application.
E-nose electronic noses utilize nano-sensor arrays to detect known components in complex mixtures of exhaled VOCs, offering advantages such as miniaturization, portability, real-time analysis, and low cost; however, they are inadequate for studying complex diseases or performing precise quantitative analysis of low-concentration VOCs.
Compared with GC-MS, proton transfer reaction mass spectrometry (PTR-MS) can detect VOC concentrations at the pptv level, enabling multiple online measurements without the need for time-consuming and costly pre-concentration steps. It has currently been applied to monitor anesthesia, respiratory patterns, and hemodialysis. However, for VOC analysis, it still has limitations in detecting low-molecular-weight alkanes and sulfur-containing compounds associated with bacterial metabolism.
The newly developed SPI-TOF at the Dalian Institute of Chemical Physics leverages composite ionization technology to enable rapid, online analysis of trace components in gases. With its excellent reproducibility, low degree of fragmentation, and no need for pre-concentration, it holds the potential to become a standard analytical tool for VOCs.
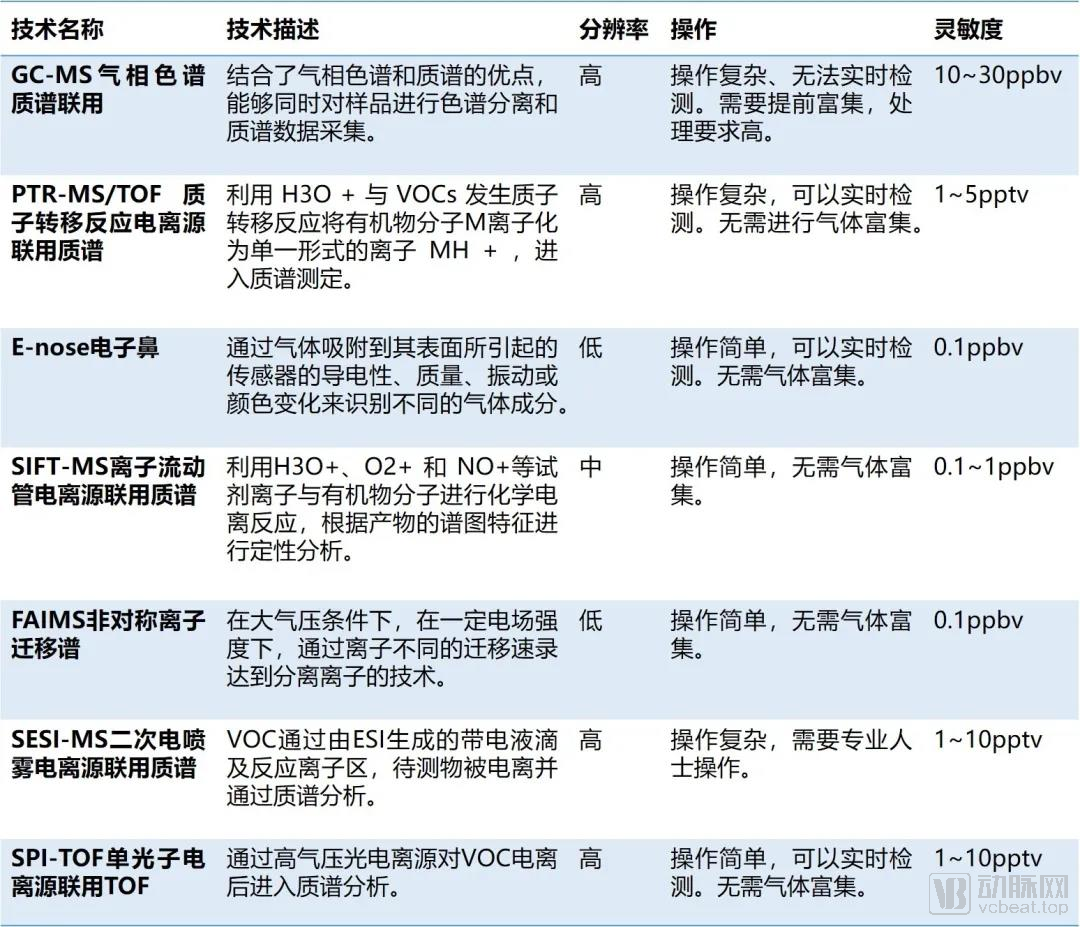
Table 5 Comparison of Existing VOC Detection Technologies and Performance. Source: Compiled by Miracle Light
According to incomplete statistics, there are nine companies worldwide specializing in breath-related technologies, distributed across various countries. Among them, Owlstone is the most representative and well-funded enterprise, yet it still has some way to go before achieving a leading position.
Commercialized detection technologies primarily include mass spectrometry (GC-MS, SIFT-MS, FAIMS, SESI-MS) and sensors. Most companies were established after 2015 and are still engaged in technological optimization and clinical validation; the industry as a whole is in its early stages of development, with limited competition. Product pipelines are largely focused on pulmonary diseases, cancer, blood glucose monitoring, and digestive system disorders. The U.S. National Cancer Institute has provided a $2 million grant to fund a multicenter blinded study by Menssana Research, and multiple companies have secured successive rounds of financing, indicating favorable industry development trends.

Table 6. Incomplete Statistics of Commercial Companies, Source: Compiled by Miracle Light
From ancient disease diagnosis through taste and odor recognition to modern metabolomic analysis, the field has consistently sought breakthroughs in breath testing. However, due to the complexity of metabolomics, the lack of standardized tools and optimized processes for sample collection, sample enrichment, and analysis in breath testing workflows has posed significant challenges to industrialization. Basic research efforts are exploring various gas sampling methods and employing different strategies for sample enrichment, while also addressing issues related to adsorption–desorption losses and separation biases. Consequently, there is no clear academic consensus on specific volatile organic compound (VOC) biomarker panels for any given disease.
With further iterations and upgrades in online analytical technologies, system errors associated with sample concentration will be eliminated. Meanwhile, high-sensitivity analytical instruments enable standardized, high-throughput sample analysis. Consensus on biomarkers for disease screening and diagnosis is gradually being established, and low-cost, user-friendly, non-invasive breath testing is on the verge of an industrial boom.
[References]
[1]Francesco FD, Fuoco R etc.Breath analysis: Trends in techniques and clinical applications. Microchemical Journal. 2005;79:405–410.
[2]Souvik Das, Saurabh Pal, Madhuchhanda Mitra.Significance of Exhaled Breath Test in Clinical Diagnosis: A Special Focus on the Detection of Diabetes Mellitus. J Med Biol Eng. 2016; 36(5): 605–624.
[3]Hakim M, Broza YY, Barash O, et al. Volatile organic compounds of lung cancer and possible biochemical pathways. Chem Rev 2012; 112: 5949–5966.
[4]Hanna GB, Boshier PR, Markar SR, Romano A. Accuracy and Methodologic Challenges of Volatile Organic Compound–Based Exhaled Breath Tests for Cancer Diagnosis: A Systematic Review and Meta-analysis. JAMA Oncol. 2019;5(1):e182815. doi:10.1001/jamaoncol.2018.2815.
[5]Waqar M. Ahmed,Orcid etc.Exhaled Volatile Organic Compounds of Infection: A Systematic Review.ACS Infect. Dis. 2017, 3, 10, 695–710.
[6]Lieuwe D.J.Bos,PeterJ.Sterk.Volatile Metabolites of Pathogens: A Systematic Review.plospathogens. May 9, 2013.
[7] Exhaled breath analysis: a review of ‘breath-taking’ methods for off-line analysis;Oluwasola Lawal, Waqar M. Ahmed etc.Metabolomics. 2017; 13(10): 110. Published online.
[8]Solid-phase microextraction: a powerful sample preparation tool prior to mass spectrometric analysis.Vas G, Vékey K. Mass Spectrom. 2004 Mar; 39(3):233-54.
# About Blue Rainbow
Blue Rainbow is an incubation and venture capital platform initiated by BGI, serving global startups in life sciences and precision medicine. It focuses on cutting-edge research and technologies across multi-omics scales—including DNA, RNA, proteins, cells, and tissues—and is committed to fostering an innovation ecosystem with comprehensive support to enhance the efficiency of industrial translation.