New Version of Tertiary Hospital Evaluation Standards Released: DRG Becomes Core Evaluation Framework
On December 28, the National Health Commission (hereinafter referred to as the NHC) released the Accreditation Standards for Tertiary Hospitals (2020 Edition) (hereinafter referred to as the 2020 Standards). This is the first entirely new version of the standards in the nine years since the NHC issued the Accreditation Standards for Tertiary General Hospitals (2011 Edition) (hereinafter referred to as the 2011 Standards) in 2011.
Image source: Official website of the National Health Commission
VCBeat (WeChat ID: Vcbeat) compared the 2020 edition of the standards with the 2011 edition. It found that the 2020 edition places significant emphasis on DRGs; it is fair to say that DRGs will become a crucial component of the future accreditation standards for tertiary hospitals!
In the 2020 edition of the standards, the most significant revision is the division of all content into three parts. Among these, Part II focuses on data monitoring for medical service capabilities and quality safety, comprising 74 sections and 240 monitoring indicators. This part carries a weight of no less than 60% in the overall accreditation score, making it the highest priority.
Image from “Accreditation Standards for Tertiary Hospitals (2020 Edition)”
Compared with the 2011 edition, the second part of the 2020 edition places greater emphasis on monitoring indicators related to hospital resource allocation, quality, safety, services, and performance, as well as on routine monitoring data for DRG evaluation, single-disease quality control, and key medical technologies, while extensively applying the DRG evaluation system. It is no exaggeration to say that DRG serves as the core thread running through the entire second part of the 2020 edition.
The 2020 edition of the standards for medical service capacity includes six indicators: the number of diagnosed disease categories (based on four-digit ICD-10 subcategories), the number of inpatient surgical procedures (based on four-digit ICD-9-CM-3 subcategories), the number of DRG groups, DRG Case Mix Index (CMI), DRG Time Index, and DRG Cost Index. All these indicators are directly related to Diagnosis-Related Groups (DRGs).
Hospital quality indicators include the annual improvement in national medical quality and safety goals, overall inpatient mortality rate, neonatal inpatient mortality rate, surgical patient inpatient mortality rate, unplanned readmission rate within 0–31 days after discharge for inpatients, unplanned return to the operating room for reoperation within 48 hours or 31 days post-surgery for surgical patients, and inpatient mortality rates for 115 low-risk ICD-coded conditions. These indicators are, to varying degrees, associated with Diagnosis-Related Groups (DRGs).
Chapter 7 of the 2011 edition of the standards also sets forth corresponding requirements for hospitals’ medical service capabilities. For instance, routine monitoring indicators for treatment quality include: the number of cases with concordance between intraoperative frozen section and paraffin-embedded section diagnoses; the number of cases with concordance between preoperative and postoperative pathological diagnoses for malignant tumors; the number of inpatient deaths and cases of discharge against medical advice; the number of inpatient surgical procedures and associated deaths; the number of critically ill inpatients undergoing emergency resuscitation and associated deaths; the number of critically ill patients in the emergency department undergoing emergency resuscitation and associated deaths; and the inpatient mortality rate among neonatal patients.
Among the inpatient healthcare quality and safety monitoring indicators that can be directly benchmarked against the 2020 version of the DRG standards, the 2011 version focused on three categories of outcome quality: readmission rates (rehospitalization and reoperation), mortality rates (in-hospital death and postoperative death), and safety indicators (complications and patient safety). These included indicators for key inpatient diseases (total number of cases, number of deaths, number of rehospitalizations within 2 weeks and 1 month, average length of stay, and average hospitalization cost), key inpatient surgeries (total number of cases, number of deaths, number of unplanned postoperative reoperations, average length of stay, and average hospitalization cost), as well as anesthesia and inpatient patient safety indicators.
In greater detail, the three indicators in the 2020 edition of the standards—namely, the number of diagnosed conditions treated (based on four-digit ICD-10 subcategories), the number of inpatient surgical procedures performed (based on four-digit ICD-9-CM-3 subcategories), and the number of DRG groups—represent the “breadth” of a hospital’s medical service capacity. The greater the number of DRG groups covered by these three indicators, the more comprehensive the hospital’s technical capabilities are. For instance, if a general hospital can cover more than 400 DRG groups in a given year, while another hospital in the same region covers only slightly over 200, this indicates that the latter has weaker comprehensive service capabilities compared to the former.
DRG-CMI measures the “depth” of overall medical services, i.e., the level of technical complexity; a higher value indicates greater complexity in hospital medical services. Suppose the average case weight for hospitals in a certain region is 1. Under the same number of cases, Hospital A has an average weight of 1.5, while Hospital B has only 0.7. This suggests that Hospital A has a higher level of technical expertise, whereas Hospital B has a lower level.
The DRG Time Index refers to the average time required for a hospital to treat a specific DRG group, while the DRG Cost Index refers to the average cost incurred by a hospital in treating that same DRG group. These two metrics, adjusted for case-mix weights, can be used to measure hospital efficiency.
Given the stringent data collection requirements of Diagnosis-Related Groups (DRG), the 2020 edition of the standards also establishes uniform specifications for data collection. The collected data, sourced from the National Clinical Improvement System (NCIS), the Hospital Quality Monitoring System (HQMS), and various provincial-level data collection systems, adheres to unified data requirements and standards.
The ICD codes used are based on the National Clinical Version 2.0 of the Classification and Codes of Diseases, commonly referred to as the "Clinical Version of ICD-10"; the surgical procedure codes used are from the National Clinical Version 2.0 of the Classification and Codes for Surgical Procedures, commonly referred to as the "National Clinical Version of ICD-9-CM3."
In contrast, although the 2011 version of the standards also stipulated disease classification codes and procedure codes, there was no consensus on DRG development in China at that time, and significant variations existed in the coding systems and DRG groupers adopted across different regions. Most critically, due to the lack of unified and objective data collection sources and standards, data usability was poor.
Overall, the evaluation under the 2011 standards relied primarily on relatively broad data metrics. In contrast, the 2020 standards place greater emphasis on daily quality management and performance, supported by specific, data-driven indicators that offer a more objective assessment. Diagnosis-Related Groups (DRG) will play a central role in this process; therefore, a thorough understanding and mastery of DRG as a tool will be key to determining whether hospitals can successfully pass the Grade A Tertiary Hospital accreditation.
In addition to the significant change of introducing DRGs, the 2020 version of the standards also features several other notable improvements compared to the 2011 version.
First, it fully integrates newly issued policies and healthcare reform requirements to reflect contemporary relevance. Building on the continuity of the 2011 edition, the 2020 edition incorporates provisions from laws, regulations, and rules promulgated and implemented in recent years—including the Basic Healthcare and Health Promotion Law, the Regulations on the Prevention and Handling of Medical Disputes, the Measures for the Administration of Medical Quality, the Measures for the Administration of Clinical Application of Medical Technologies, and the Key Points of Core Systems for Medical Quality and Safety—as well as reform requirements such as the development of a tiered diagnosis and treatment system and the modern hospital management system.
Meanwhile, in response to the current COVID-19 pandemic, the 2020 edition of the standards has added requirements for normalized prevention and control measures. Section 3 of Part I (“Preliminary Requirements”) of the 2020 edition provides the following definition for “Safety Management and Major Incidents”: occurrence of a Level 1 medical accident determined to involve full liability, or a major medical accident directly adjudicated by the health administrative department; occurrence of a major hospital-acquired infection event resulting in serious consequences; occurrence of a major safety accident, such as a significant fire, radioactive source leakage, or hazardous gas leakage, that leads to official notification or penalties; concealment or underreporting of major medical negligence incidents; and large-scale medical data breaches or other major cybersecurity incidents resulting in serious consequences.
Second, as previously mentioned, there is a shift from subjective qualitative assessment by supervisors to objective quantitative evaluation, thereby enhancing scientific rigor. By introducing a more scientific and objective DRG evaluation system, the 2020 version of the standards aims to guide regions in transitioning from an assessment approach primarily based on on-site inspections, subjective qualitative judgments, and centralized reviews to a work mode that integrates routine monitoring, objective indicators, on-site inspections, and a combination of qualitative and quantitative assessments.
Third, the on-site assessment provisions have been reorganized, integrated, and simplified to enhance operability. The 2020 edition of the standards comprises 183 items across 24 sections for on-site inspections, representing a substantial reduction from the 66 sections and 354 items in the 2011 edition.
On the one hand, redundant provisions in the original standard were comprehensively reviewed and consolidated to improve work efficiency; on the other hand, provisions that lacked operational feasibility or could be replaced by routine data monitoring instead of on-site inspections were eliminated or adjusted to enhance the standard’s operability.
Finally, the 2020 edition of the standards places greater emphasis on drawing upon advanced concepts and experiences from both international and domestic sources, thereby demonstrating enhanced compatibility. It fully incorporates the methodologies and standards of certain international hospital accreditation bodies, while also adopting best practices and experiences from various provinces and cities in China, thus achieving greater alignment and compatibility with advanced philosophies in accreditation and evaluation management both domestically and internationally.
As a management tool, DRG serves the dual purposes of “cost control” and “quality management.” In fact, the first-generation DRG system developed by Yale University in the United States was designed as a quality management tool to help clinicians and hospitals monitor service quality and utilization.
In the 2020 edition of the standards, Diagnosis-Related Groups (DRG) have been elevated to the status of a core tool. This means that all tertiary hospitals in China, as well as secondary hospitals aspiring to upgrade to tertiary status, must promptly familiarize themselves with and accelerate the implementation of DRG systems within their institutions in the coming period.
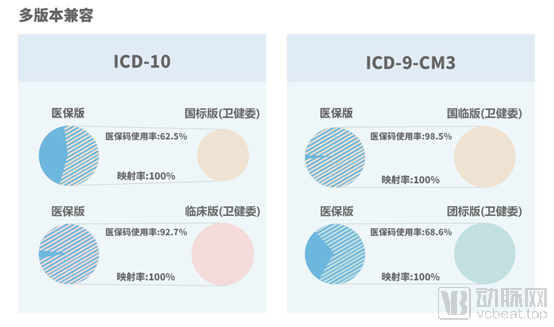
Image source: Official website of the National Healthcare Security Administration
Meanwhile, on the payment side, the National Healthcare Security Administration (NHSA) is vigorously promoting CHS-DRG and DIP. Since the 2020 version of the standards applies to all tertiary hospitals nationwide without specifying any exceptions, this implies that even tertiary hospitals in DIP pilot cities are still required to use DRG tools for accreditation purposes. Given that NHSA medical insurance codes can achieve 100% mapping to the National Health Commission’s codes, this may also indirectly reflect the future trajectory of both DIP and DRG.