Can China's New 27-Point Medical Record Quality Control Guidelines Break Down Hospital Data Silos?
As a critical carrier of medical activity records, medical records have always been the primary source of data for healthcare quality management and the foundation for scientific research across various clinical specialties, making their importance self-evident. However, in practice, issues such as insufficient attention from physicians and hospitals, the absence of talent development systems, and a significant shortage of qualified professionals mean that quality management of this essential documentation remains an ongoing priority for hospitals.
Recently, the National Health Commission released the “Quality Control Indicators for Medical Record Management (2021 Edition)” along with its accompanying interpretation. After many years, medical record issues have once again been prioritized as a key management task. Unlike the 2016 focus on quality management of the medical record face sheet, this initiative extends quality control to the entire medical record. The document outlines 27 calculation formulas covering five areas: human resource allocation indicators, timeliness of medical record documentation, compliance rate of major examination records, compliance rate of diagnostic and treatment behavior documentation, and medical record archiving quality indicators. This effort aims to promote effective improvement in medical record quality through the establishment of a scientific and standardized quality control system, thereby enhancing the role of medical records in health big data.
Following the release of the document, VCBeat engaged in discussions on the policy with companies specializing in the development of medical record quality control applications, such as Baidu Lingyi Zhihui and Huimei Technology, as well as multiple industry experts. The analysis of the policy was summarized into three aspects:
I. The Significance of Policies for Medical Record Quality Control;
II. Detailed Explanation of the 27 Quality Control Indicators for Medical Record Management ;
3. Multi-dimensional Industry Impact.
Through three key dimensions, we aim to dissect the catalytic role of policies in driving hospitals and the industry forward, thereby understanding the potential value of this market.
When it comes to medical big data and informatization, the most frequent criticism centers on the problem of information silos both between medical institutions and within hospitals. For years, researchers have attempted to build bridges across these silos, only to find that overcoming one obstacle inevitably reveals another. After all, the fragmentation of medical information and privacy concerns make it difficult for researchers to unlock a comprehensive solution through any single metric.
However, among the various data carriers, medical record data stands out as a potential solution to break down data silos. Since the early 21st century, the Chinese government has required hospitals to submit data from their medical records departments. Subsequently, the introduction of the HIMSS (Healthcare Information and Management Systems Society) ratings in China, as well as the recent emphasis on performance evaluations for tertiary public hospitals, have all incorporated the quality of medical record face sheets into their assessment criteria. Therefore, regardless of the hospital, the coding, core fields, and ID requirements for medical record face sheets are uniform. As a result, data from medical record face sheets represent the most complete and trustworthy data source.
However, even the most comprehensive and trustworthy face sheet data of medical records have flaws that cannot be ignored.Following the implementation of Diagnosis-Related Groups (DRGs), the role of medical records in hospitals has undergone a dramatic transformation. Initially serving merely as documentation of clinical activities, medical records now function as critical vouchers for health insurance reimbursement, becoming a core determinant of hospital operational costs and revenue.
It was only then that people realized that the data on the front pages of medical records in many hospitals were unreasonable, leading to flawed baseline parameters for assessing healthcare quality and, consequently, unreasonable results. The legacy of past documentation practices has now become an operational risk. Therefore, the data quality of medical record front pages must be standardized, and to achieve this standardization, it is essential to address the quality of the medical records themselves.
Therefore, from the documents released this time, we can discover thatPast policies primarily imposed requirements and restrictions on the front page of medical records, whereas this policy explicitly specifies quality standards for medical records and even mandates timeliness in data entry.The determination of the state to standardize medical quality is evident from the numerous indicators.
Certainly, under the recent policies of the National Health Commission, the implementation of Diagnosis-Related Groups (DRG) is poised to yield positive impacts. More importantly, against the backdrop of elevating the development of healthcare big data to a national strategy, it is crucial to identify solutions to address the issues of non-standardization, high costs, and low value associated with medical big data. This will facilitate the transition from experience-driven to data-driven decision-making, thereby enabling deeper insights into problems within the healthcare system and identifying effective solutions.
However, to conduct a detailed analysis of the changes brought about by future medical record quality control, we must analyze each medical record management quality control indicator.
The document categorizes the 27 indicators into five major groups: human resource allocation indicators, timeliness of medical record documentation indicators, compliance rate of records for major examinations, compliance rate of diagnostic and treatment behavior documentation, and medical record archiving quality indicators. Certain indicators exhibit interrelationships.
I. Human Resource Allocation Indicators

The shortage of personnel in medical records departments has long been a key factor constraining the quality of medical records. On one hand, medical record quality control places extremely high demands on the capabilities of quality control staff; qualified personnel must have a clinical background. For instance, the job posting for quality control positions at West China Hospital requires applicants to hold “a master’s degree or higher” and possess “a background in clinical medicine or related fields.” Such recruitment requirements are by no means low—in fact, they are significantly higher than those for many clinical departments in central urban hospitals.
On the other hand, a single medical record can range from dozens to hundreds of pages. Manual quality control is highly time-consuming, and even experienced physicians find it difficult to identify errors within large volumes of data in a short period. Many errors can only be detected by cross-referencing various sections of the medical record, which places exceptionally high demands on the comprehensive competencies of quality control personnel.
Under these various factors, the number of quality control staff in the medical records departments of ordinary hospitals is typically fewer than ten, and even high-quality Grade A tertiary hospitals generally do not exceed 40. This means that the average daily workload for each quality control specialist ranges from 40 to 60 medical records, far exceeding the international average of 10 records per day. Quality and quantity cannot be simultaneously optimized; consequently, medical records in hospitals currently exhibit varying degrees of quality issues.
Having understood the pain points, we then examine the policy. The document mentions that the average monthly workload of inpatient medical record management staff and medical record coders will be calculated, essentially aiming to assess the actual human resource needs of medical records departments. Baidu Lingyi Zhihui told VCBeat: “Many experts have emphasized the importance of medical records and highlighted the talent shortage in medical record departments, yet no one has precisely quantified the extent of this gap. From another perspective, just as hospital staffing needs are determined by analyzing the nurse-to-physician ratio, the emergence of such metrics provides regulatory authorities with data-driven insights to accurately assess manpower requirements in medical record departments and thereby develop effective talent cultivation mechanisms.”
II. Timeliness Indicators for Medical Record Documentation
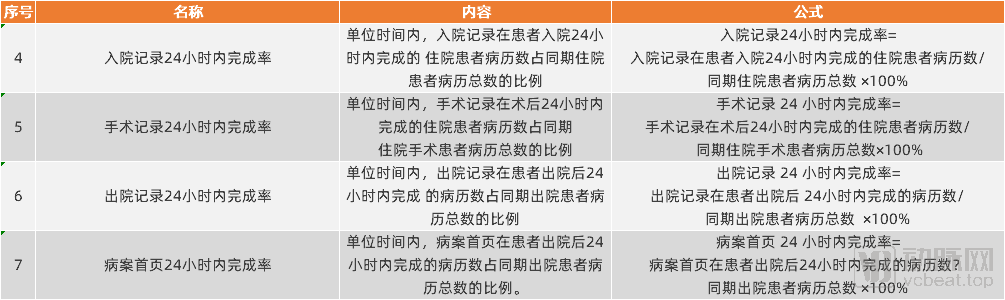
Part II of the document establishes standards for the timeliness of medical record documentation. It requires that admission notes, operative reports, discharge summaries, and the front sheet of the medical record be completed within 24 hours. These standards, which had been previously established, are reiterated here.
There are multiple interpretations for imposing timeliness requirements. First, within the clinical diagnosis and treatment workflow, information should be entered promptly upon completion of each step. However, due to the heavy workload in medical practice, many physicians are accustomed to completing diagnostic and treatment records in a batch after finishing their primary tasks, which may lead to erroneous entry of certain information.
Liu Jiao, Vice President of Medicine at Huimei Technology, told VCBeat, “The issue of timeliness is generally quite severe. We conducted a statistical analysis on the timeliness of medical records at a Grade A tertiary hospital. Over a two-week period, we reviewed 800 electronic medical record (EMR) timeliness entries. The results showed that 495 EMR admission notes had timeliness issues, and 317 EMR discharge summaries had timeliness issues.”
Many physicians, if they fail to complete medical records in a timely manner, often copy another patient’s medical record at a later stage and make minor adjustments based on it. This practice leads to discrepancies between the actual clinical situation and the documented medical records. Article 25, “Incidence Rate of Unreasonable Medical Record Copying,” is designed to address this issue by encouraging physicians to document medical records promptly, thereby improving data quality.”
Secondly, ensuring the timeliness of medical record documentation guarantees the reliability of medical records as proof for payment. Baidu Lingyi Zhihui stated: “During the course of diagnosis and treatment, a patient’s condition is in a state of continuous change. If medical records are to serve as proof for payment and legal purposes, there must be time-bound constraints to prevent data tampering. Therefore, the core purpose of implementing timeliness controls is to ensure the fairness and rationality of payment practices when such data is used as evidence for DRG-based payments.”
III. Compliance Rate of Major Examination Records, Compliance Rate of Diagnosis and Treatment Behavior Records
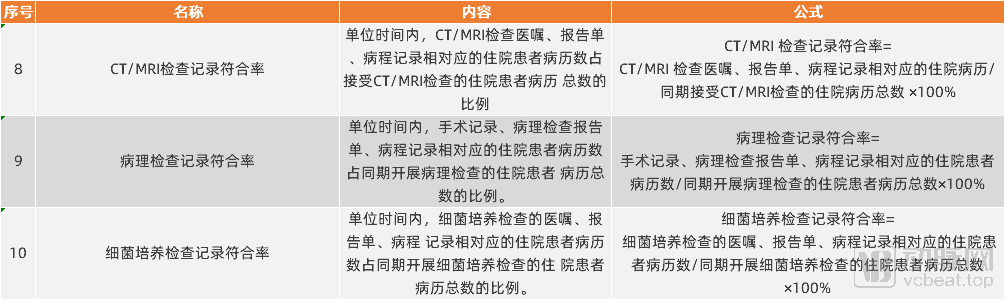
On December 31, 2020, eight ministries and commissions, led by the National Health Commission, jointly issued the “Notice on Printing and Distributing the Guiding Opinions on Further Standardizing Medical Practices and Promoting Rational Medical Examinations,” which emphasized strengthening medical management and further standardizing medical practices. Among these efforts, eleven indicators—including the compliance rate of records for major examinations and the compliance rate of records for diagnosis and treatment behaviors—provide data support for future regulatory oversight.
"In fact, since the control over the proportion of drug costs in hospitals was implemented, hospital drug expenses have decreased as expected, but the costs of examinations and tests in some hospitals have continued to rise. This situation is particularly evident in the use of certain large-scale examination and testing equipment."Therefore, the state must regulate the use of medical equipment by determining when such procedures are indicated and when they are not, thereby curbing unreasonable costs. The introduction of metrics such as the concordance rate for CT/MRI examination records, the concordance rate for pathological examinations, and the concordance rate for bacterial culture records aims to address this issue.“Liu Jiao stated.
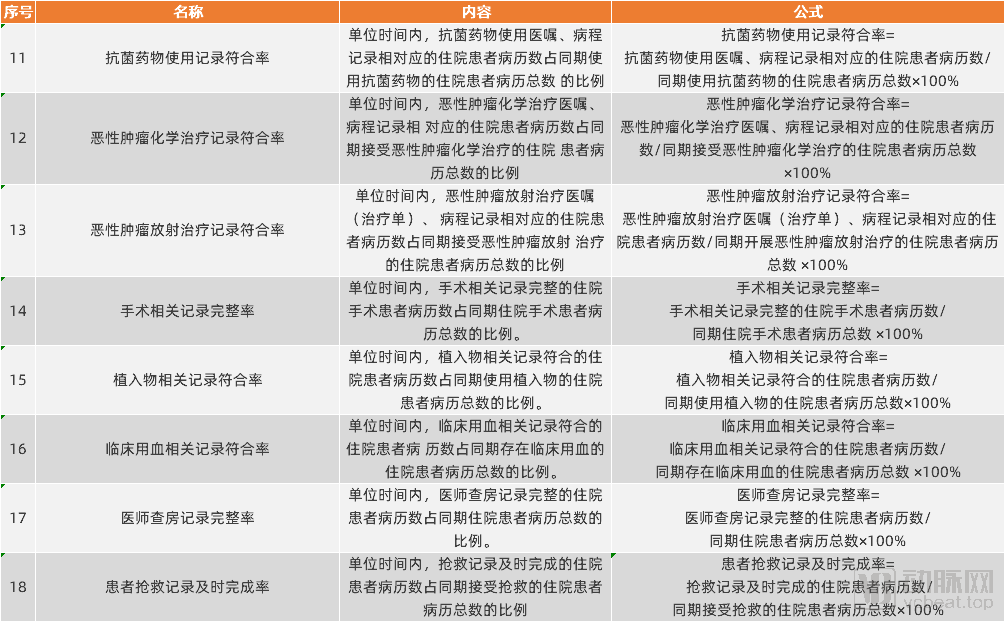
The compliance rate of diagnosis and treatment records is designed to address the issue of drug abuse. According to data from iResearch, the total output value of anti-tumor drugs in China grew by more than 20% in 2019, with sales volume of anti-tumor injections increasing by 16.73%. The rise in drug usage has been accompanied by risks of misuse and irrational health insurance expenditures, ultimately leading to more frequent emergence of multidrug-resistant bacteria and increased pressure on health insurance payments.
Revisiting the Issue of Medical Insurance Payment. In the explanations for the above 11 indicators, three elements are consistently mentioned: physician orders/surgical requisitions, report forms, and progress notes.Physician orders and surgical requisitions represent the payment for medical services, while test reports reflect the outcomes of service delivery; progress notes facilitate process control by further reconciling payment actions with execution results.
“In the past, assessments of healthcare quality typically monitored only one of three key indicators, leading to situations where physicians issued medical orders but patients did not receive the corresponding treatments. Now, by implementing unified control over all three processes, the National Health Commission can accurately trace the rationale behind medical practices, thereby achieving substantive oversight of clinical behavior,” Baidu Lingyi Zhihui told VCBeat. To ensure consistency between the front page of medical records and the complete medical history, and to guarantee the accuracy and traceability of the front-page data, the company has collaborated with the Chinese PLA General Hospital since 2019 to explore relevant solutions. These efforts have gradually yielded beneficial applications in areas such as health insurance regulation and hospital internal controls.

Smart Medical Record Sample
IV. Quality Indicators for Medical Record Archiving
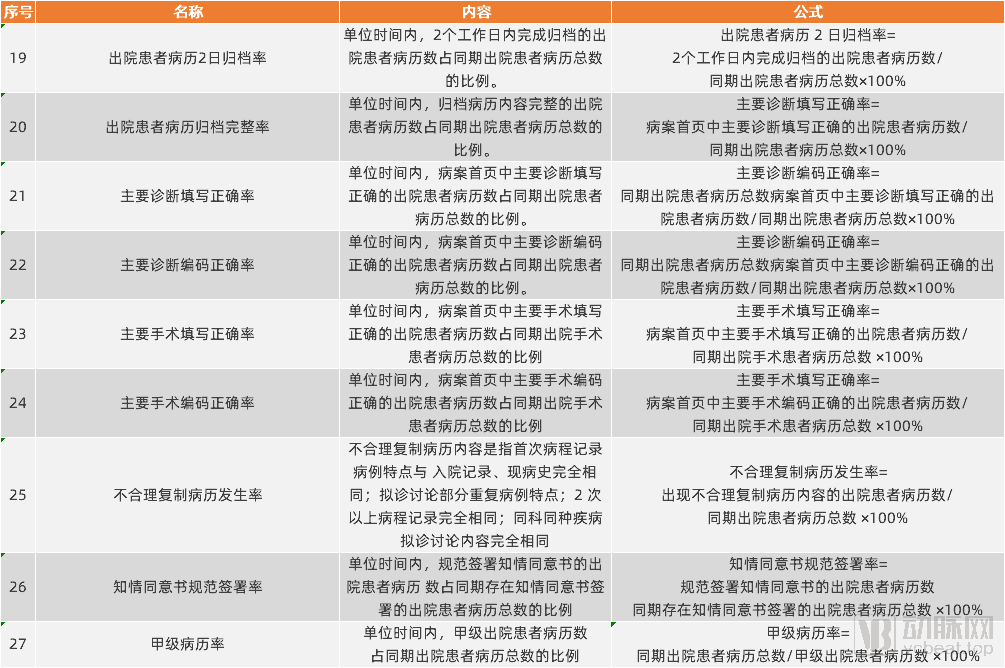
There are a total of nine quality indicators for medical record archiving. Among these, the four most targeted indicators are the accuracy rate of primary diagnosis documentation, the accuracy rate of primary diagnosis coding, the accuracy rate of primary procedure documentation, and the accuracy rate of primary procedure coding. These indicators will further enhance the quality of medical records, ultimately ensuring compliance with DRG requirements.
It is worth noting that although the National Health Commission has imposed requirements on the aforementioned indicators, reviewing the collected data is by no means a straightforward process. Taking the requirements for principal diagnosis as an example, documenting the principal diagnosis involves a relatively complex process of reasoning and decision-making. Constrained by physicians’ individual capabilities, conducting a comprehensive manual audit of this indicator is not feasible.
For example, the notification on the performance appraisal results of tertiary public hospitals in 2020 mentioned that, in the data collection and quality control phases, the “Tianhe-2” supercomputer at the National Supercomputing Center in Guangzhou was used for the first time to compute and analyze the big data sets for performance appraisal.Organized more than 100 experts in medical records, finance, clinical practice, and management to conduct manual quality control.This has effectively ensured that performance appraisal results are authentic, objective, and fair.” In other words, given the current situation, the only way for the state to address issues such as the documentation and coding of principal diagnoses is to repeatedly educate hospitals through random inspections; however, this cannot be institutionalized as a routine inspection practice.
Therefore, Baidu Lingyi Zhihui believes that establishing monitoring indicators is only the first step. There is still a long way to go in leveraging information technology and even artificial intelligence to simulate the thought processes of medical coders, normalize the evaluation of primary diagnosis rationality, and ensure the efficient operation of the entire system. Of course, adhering to its mission of empowering primary healthcare with evidence-based AI, the company is also exploring how to better utilize AI reasoning to provide decision support recommendations for coders in primary care hospitals.
Based on the documents, the policy primarily affects three target groups: regional regulatory agencies, hospitals, and health IT companies.
For regional regulatory authorities, the issuance of policies provides a lever for healthcare quality reform. If hospitals can be driven to fully report data on various indicators, regulators will be able to effectively standardize medical practices, promote appropriate medical testing, and advance the implementation of Diagnosis-Related Groups (DRG). However, as noted above, this merely completes the data collection phase of the overall regulatory process; the analysis and processing of massive datasets may require support from technologies such as Natural Language Processing (NLP).
For hospitals, the requirement to ensure performance metrics has, to some extent, eliminated gray income, increased the daily workload of physicians, and imposed higher demands on hospitals’ capabilities in information collection and cross-verification of data. This necessitates further investment in informatization construction to enhance interoperability and risk control capabilities. In the long run, this will improve the quality of medical services, and hospital revenue models will shift from diversified operations to DRG-based incentives.
For healthcare IT enterprises, the release of each new policy presents both fresh opportunities and challenges, and this particular policy is undoubtedly a boon for companies specializing in smart medical record informatization. As previously mentioned, given the current structure of the healthcare workforce, the most effective approach to improving data quality and optimizing clinical workflows is to leverage information technology solutions. This involves delegating cumbersome tasks to AI and shifting from labor-intensive, spot-check-based quality control to computer-driven, content-focused quality assurance, thereby enabling comprehensive processing of collected data. Based on current tender prices for medical record quality control systems, which range from RMB 500,000 to 2 million, hospital investments in smart medical records are poised to create a market worth hundreds of billions of yuan. Meanwhile, as informatization services become increasingly reliant on the precision and intelligence of Natural Language Processing (NLP) technology, traditional IT companies are compelled to collaborate with specialized health information technology firms. This trend presents a rare opportunity for companies such as Lingyi Zhihui and Huimei Technology.
Overall, the quality control indicators for medical record management mentioned in this policy will serve initiatives such as the performance evaluation of tertiary public hospitals, Diagnosis-Related Groups (DRG), and the further standardization of clinical practices to promote appropriate medical examinations, but are not limited to these areas. Given the diversity and completeness of the data collected, future policies may leverage these indicators as a key mechanism to drive further reforms in healthcare informatization and the quality of medical services.