Is the 'Outpatient DRG' Coming? An In-Depth Look at Jinhua's Outpatient Payment Reform Pilot
On January 14, 2021, the Information Office of the Jinhua Municipal People’s Government held a press conference on deepening healthcare security reform and the citywide implementation of outpatient “APG Point-Based” payment in Jinhua City. It announced that the Jinhua Municipal Healthcare Security Administration, in conjunction with the Jinhua Municipal Finance Bureau and the Jinhua Municipal Health Commission, had issued the *Interim Measures for Outpatient Payment under Basic Medical Insurance in Jinhua City*, thereby launching the reform of outpatient “APG Point-Based” payment across the entire administrative area of Jinhua City.

This reform represents another innovative pilot by Jinhua City in health insurance payment methods, following the “DRG Point System,” and has also been included as a provincial-level pilot. Therefore,What Exactly Is the Outpatient Payment System Represented by the APG Points Method? How Do Outpatient Payment Systems Operate Abroad? What Are the Characteristics of Jinhua’s Outpatient Payment System Compared with Pioneers, and Where Is There Room for Improvement?VCBeat (WeChat ID: Vcbeat) attempts to interpret this by drawing on practices from other countries and expert opinions.
APG, short for Ambulatory Patient Groups, is literally translated as "Ambulatory Case Mix Groups." Similar to the increasingly well-known DRG (Diagnosis-Related Groups), APG is a type of case mix classification system. Other case mix classification systems include RUG (Resource Utilization Groups), FRG (Functional Related Groups), and URG (Urgency Related Groups).

Common Case Grouping and Classification
Their commonality lies in grouping and clustering cases in a specific manner to facilitate management or payment. Naturally, due to differing grouping criteria, these case-mix systems are each suited to different contexts. Taking Diagnosis-Related Groups (DRGs) as an example, their classification is based on diagnoses and procedures; therefore, DRGs are suitable as a risk-adjustment tool only for cases where diagnosis and treatment modalities significantly impact resource utilization and treatment outcomes—namely, short-stay inpatient cases.
DRGs have indeed effectively curbed the rise in short-term inpatient costs. However, this represents only a portion of overall medical practice. As hospitals shifted inpatient costs to outpatient services, outpatient expenses grew at a rate far exceeding natural growth drivers such as inflation and advancements in medical technology. In response, outpatient bundled payment models were introduced to address outpatient cost containment.
At the pilot launch event in Jinhua City, it was noted that prior to the implementation of the “APG Point-Value Method” for outpatient payment reform, outpatient medical expenses were not subject to global budgeting. Settlements were based on actual costs incurred by designated hospitals and pharmacies, leading to a rapid surge in outpatient expenditure. The annual growth rate of outpatient medical insurance fund spending was approximately 20%, significantly higher than the growth rate of inpatient medical insurance fund spending observed after the DRG pilot. Through the reform of composite outpatient payment mechanisms, the annual growth rate of outpatient medical insurance fund expenditures is expected to be controlled within 10%, thereby forming a closed-loop management system alongside DRGs.
Currently, the grouping criteria for bundled outpatient payments primarily include the disease type, treatment modality, and cost utilization associated with outpatient medical services. The Jinhua Municipal Healthcare Security Administration’s “Measures for Outpatient Payment under Basic Medical Insurance in Jinhua City (Trial)” (hereinafter referred to as the “Trial Measures”) provides an explanation of the Ambulatory Patient Group (APG) classification used in Jinhua City.
According to the Trial Measures, Jinhua’s Ambulatory Patient Groups (APGs) primarily consolidate multiple settlement cases with the same primary diagnosis for a single patient within one treatment cycle (currently provisionally defined as one day) at the same medical institution into a single case, based on similarities in clinical pathways and resource utilization. Through clustering analysis, APG groups tailored to Jinhua’s local conditions are formed. These APG groups are specifically categorized into three types: Surgical Procedure APGs, Medical Service APGs, and Ancillary Service APGs.
Surgical Procedure APGs primarily include cases dominated by surgical interventions (including anesthesia, medications, etc.). If such cases involve significant diagnostic or laboratory tests, these items must be separately classified into Ancillary Services APGs. The same principle applies to cost calculation: surgery-related costs are grouped under Surgical Procedure APGs, while associated diagnostic and laboratory test costs are grouped under Ancillary Services APGs.
Internal Medicine Service APGs cover cases primarily managed with pharmacological treatment. Similar to Surgical Procedure APGs, if such cases include significant diagnostic tests or laboratory examinations, these items are classified into Ancillary Service APGs. For cost calculation purposes, expenses related to internal medicine pharmacological treatment are included in the Internal Medicine Service grouping costs, while costs for associated diagnostic and laboratory tests are included in the Ancillary Service grouping costs.
Auxiliary Service APGs primarily cover cases involving diagnostic tests and laboratory examinations. As previously mentioned, Auxiliary Service APGs include the test and examination items from both Surgical Procedure APGs and Internal Medicine Service APGs. In addition, Auxiliary Service APGs encompass outpatient consultation fees, general diagnosis and treatment fees, consumables requiring separate compensation, and drugs included in the National Reimbursement Drug List through price negotiations. Among these, nationally negotiated drugs are grouped by their generic names, with newly added nationally negotiated drugs being grouped by generic names starting from the following year.
According to publicly available information, Jinhua City began exploring outpatient payment reforms as early as January 2020. At the work deployment meeting for the reform of outpatient payment under the Basic Medical Insurance in Jinhua City held on January 2, 2020, the Jinhua Municipal Healthcare Security Administration planned to implement a reform combining capitation-based outpatient payment with family physician contracting payments (the “APG Point System” payment method).
In May 2020, Jinhua City’s reform of outpatient medical insurance payment, which combines capitation with the Ambulatory Patient Groups (APG) point-based method, was included as a provincial-level pilot project in Zhejiang Province. As the first initiative of its kind in China and the only one nationwide at the time, this outpatient payment reform marked the fourth national or provincial-level pilot project undertaken by the Jinhua Municipal Healthcare Security Administration since its establishment.
By July 2020, Dongyang City, under the jurisdiction of Jinhua City, had completed the second round of feedback on the grouping results for historical outpatient data. Through cluster analysis of 1.41 million records covering various types of outpatient medical expenses totaling RMB 394 million from 16 medical institutions, the local Healthcare Security Administration categorized Ambulatory Patient Groups (APGs) into 761 groups for city-level hospitals and 347 groups for primary care hospitals in Dongyang. This also indicates that preparations for outpatient payment reforms across the entire Jinhua region are proceeding in an orderly manner.
Ultimately, by consolidating the citywide groupings, the outpatient payment pilot in Jinhua City established 1,391 Ambulatory Patient Group (APG) categories. By leveraging big data analytics to examine historical outpatient case volumes and reasonably calculate the average historical costs for each disease group, a payment standard mutually recognized by medical insurance authorities, hospitals, and patients was formulated.
Notably, although the outpatient payment reform in Jinhua City is abbreviated as “APG Point-Based Payment,” the APG point system does not constitute its entirety. In fact, Jinhua’s outpatient payment reform adopts a composite payment method that combines capitation under a global budget with the APG point-based payment system.
First, a global budget management system is implemented for the outpatient medical insurance fund. The global budget is managed separately by municipal and county (city) pooling areas, covering expenditures from the pooled fund for insured individuals’ outpatient services (including externally dispensed electronic prescriptions) at designated medical institutions both within and outside the pooling area, as well as medication purchases at designated pharmacies. Outpatient services include general outpatient care, outpatient care for chronic diseases, and outpatient care for special diseases.
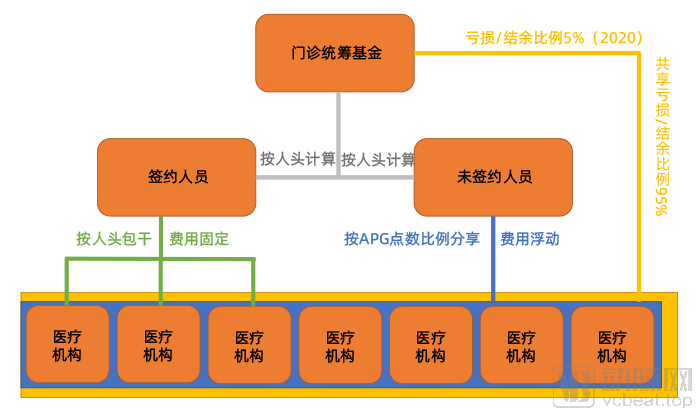
Diagram of the Jinhua Outpatient Payment System, by VCBeat
Payment methods for the medical insurance fund across the entire pooling area are divided into two main categories: capitation and APG point-based payment, with different methods adopted according to specific circumstances.
First, a capitation model will be implemented. Jinhua City will promote the signing of contracts between medical institutions and basic medical insurance enrollees, thereby allocating the outpatient capitation fund to the contracted medical institutions (or medical consortia) for consolidated management. Any surplus shall be retained by the medical institutions, while any deficit shall be borne by them.
For capitation-based payment, the per-capita payment rate is the key determinant of whether healthcare institutions operate at a profit or a loss. It is reported that Jinhua City uses big data analytics to determine the outpatient capitation fund allocation for insured individuals, based on their outpatient visit patterns across the city over the previous two years.
It is worth noting that the capitation-based outpatient services in Jinhua City currently cover general outpatient and chronic disease outpatient care, but temporarily exclude special disease outpatient care for enrolled insured individuals. This exclusion is due to the specific service capacity requirements that special disease outpatient care imposes on medical institutions. The Trial Measures also state that “as the service capacity of contracted medical institutions improves, capitated quotas for special disease outpatient care for enrolled individuals may be gradually allocated to these contracted institutions (medical consortia).”
Currently, capitation-based payment models are relatively rare in China. Interpretations provided at the press conference stated that “by leveraging economic incentives, capitation will further stimulate the intrinsic motivation of primary healthcare institutions to deliver family doctor contract services, encouraging them to take a more proactive and active role in providing such services. This will enable the delivery of chronic disease management and comprehensive, high-quality health services to residents within their jurisdictions, thereby better fulfilling the role of family doctors as gatekeepers of health.”
This will drive relevant healthcare institutions to place greater emphasis on basic public health services and health management within their coverage areas, shifting the focus from disease treatment to disease prevention. By keeping enrolled members physically and mentally healthy, detecting early signs of disease for timely intervention, and reducing unnecessary waste of outpatient medical insurance funds, healthcare institutions can achieve surpluses under the fixed capitation payment model.
Under the current outpatient payment mechanism, all outpatient services constitute revenue for healthcare institutions. With a strong incentive to maximize outpatient visits and diagnostic tests, these institutions naturally lack the motivation to prioritize disease prevention and health management.
Meanwhile, this approach will also steer health insurance funds toward contracted services and primary care institutions. On one hand, through patient enrollment contracts and corresponding capitation payments, primary medical institutions can sustain and expand their operations, thereby further enhancing their medical technical capabilities. On the other hand, as chronic disease management, which accounts for a significant proportion of outpatient visits, is shifted to primary care institutions, the outpatient burden on large hospitals is alleviated, allowing them to allocate more resources to tackling complex and rare diseases. A virtuous cycle of “tiered diagnosis and treatment” may thus gradually take shape. Jinhua City has also set targets for the primary care visitation rate, with a goal of 65% by 2020.
For insured individuals who have not entered into contracts, the outpatient capitation fund is pooled and utilized jointly by eligible medical institutions, with payments made according to the APG point-based method. Unlike the fee-for-service rate method, the Jinhua point-based method assigns points to disease groups and implements a floating point value based on the principle of "expenditure determined by revenue, maintaining a balance between revenue and expenditure, and achieving a slight surplus." At the end of the year, the actual value of each point is determined based on the total budget for this portion of the fund and the total APG points accumulated by hospitals across the city, and the payment due to each medical institution is then calculated accordingly.
The outpatient medical insurance fund operates under a mechanism of “retaining surpluses and sharing deficits.” In simple terms, if the annual final accounts of the pooled outpatient fund show a surplus or deficit, the healthcare institutions and the medical insurance fund will retain or share the amount according to a specified ratio. In 2020, the sharing ratio between the medical insurance fund and healthcare institutions was 5%:95%. This means that if there is a surplus in the outpatient medical insurance fund for the year, the medical insurance fund retains 5% of the surplus, while healthcare institutions retain 95%. However, if the outpatient medical insurance fund incurs a deficit, healthcare institutions are required to bear 95% of the losses exceeding the budget.
The Jinhua APG point-based method is a form of bundled payment for outpatient services. Globally, this payment system has been widely adopted, with the outpatient payment systems in the United States and Germany serving as representative examples.
The United States was the first country to develop the Diagnosis-Related Group (DRG) payment system. In 1967, Robert B. Fetter and his team at Yale University developed the first generation of DRGs, commonly known as the “Yale DRG.” As the progenitor of DRG systems, the Yale DRG was initially used for quality management, with the aim of helping clinicians and hospitals monitor service quality and utilization rates.
Due to the soaring healthcare costs in the United States, Diagnosis-Related Groups (DRGs) have also been applied to insurance payments to achieve cost containment. New Jersey was the first state to introduce DRGs into its pilot payment system reforms. Subsequently, the DRG system underwent revisions, with significant adjustments made to the coding system and grouping rules. Notably, the involvement of clinicians was incorporated, making the revised DRG system better aligned with actual clinical practice.
DRGs have indeed effectively curbed the rapid growth of inpatient costs. However, hospitals have found ways to circumvent DRG-based cost controls by discharging patients earlier or shifting costs from inpatient to other settings, leading to a rapid increase in outpatient and other expenses. In this context, it is imperative to implement effective controls over outpatient costs.
Medicare, a public health insurance program primarily designed for individuals with disabilities, patients with end-stage renal disease, and adults aged 65 and older—similar to China’s basic medical insurance system—has adopted a new outpatient payment system to replace the traditional one.
Traditionally, the Centers for Medicare & Medicaid Services (CMS), the administrative agency for Medicare, reimburses outpatient expenses through three mechanisms. The first, and most common, is fee-for-service payment (covering items such as laboratory tests, medical devices and supplies, end-stage renal disease dialysis services, and ambulance services), where fees are paid item by item according to a pre-approved fee schedule. The second is a hybrid payment method based on the lower of outpatient service costs or charges, or combining fee-for-service with the lower of costs or charges. The third method involves payment based on the lower of the reasonable costs or charges for comparable outpatient medical services in the same geographic area.
Except for the first method, which is based entirely on fee-for-service payment, the remaining two methods require that the recognition of outpatient service costs and expenses be determined retrospectively after audit and settlement, following at least two years of service provision by the clinic.
Due to variations in costs and expenses across different hospitals, Medicare is required to pay different amounts for the same medical services provided by different healthcare institutions. For instance, Medicare typically reimburses large hospitals at higher rates than private clinics for identical services. This payment “scissors gap” incentivizes large hospitals to establish satellite outpatient facilities (even located miles away from the main hospital) or acquire independent private practices, thereby securing higher Medicare reimbursements.
Meanwhile, cost-related payment methods have left hospitals with no incentive to curb over-treatment—the more services they provide, the more reimbursement they receive; reducing disease burden actually means lower hospital revenue. According to statistics, in the decade prior to 2000, Medicare’s outpatient costs soared at an annual rate of 9%. Most of this increase in outpatient spending was driven by over-treatment, rather than normal population growth or inflation.
Therefore, starting in August 2000, the United States implemented the Outpatient Prospective Payment System (OPPS) for reimbursing hospital outpatient services. Ambulatory Payment Classifications (APCs), based on Ambulatory Patient Classification grouping, constitute a core component of this system specifically designed for outpatient service reimbursement and are commonly referred to as “APC-based payment.”
Similar to the DRG system, Medicare classifies outpatient services or items into Ambulatory Payment Classification (APC) groups and pays a fixed rate for each group, irrespective of the actual costs incurred in providing these services or items. This imposes requirements on hospitals’ cost control; under comparable conditions, the lower the cost of delivering medical services or items, the greater the surplus the hospital retains from Medicare payments.
APC payments cover a wide range of services; all outpatient services provided by Medicare-participating healthcare institutions are eligible for APC reimbursement. In addition, certain mental health services provided by some community mental health centers or similar facilities are also included.
The Indian Health Service (IHS), which provides federal services exclusively to American Indians and Alaska Natives in reservation areas, as well as emergency centers reimbursed at reasonable costs, do not adopt APC payment. In addition, since Maryland is the only region in the United States with pricing authority, implementing equal prices for medical insurance and commercial insurance, most outpatient services provided by hospitals and cancer hospitals in Maryland also do not adopt APC payment.
With few exceptions, the U.S. Ambulatory Payment Classification (APC) system groups services based on clinical similarity and resource utilization into significant surgical and non-surgical procedures, outpatient and emergency department services, and ancillary services. APC payments cover hospital outpatient services previously reimbursed by Medicare on a cost- or charge-based basis, including outpatient surgeries, imaging and other diagnostic tests, outpatient and emergency department visits, medical supplies, colorectal cancer screening, and various other preventive services.
Medicare calculates the national unadjusted group rates for these individual medical or surgical services by multiplying the scaled relative weights of APC groups by a conversion factor. The relative weights measure the geometric mean cost of resources required for an APC group. The conversion factor converts the scaled relative weights into dollar-based rates.
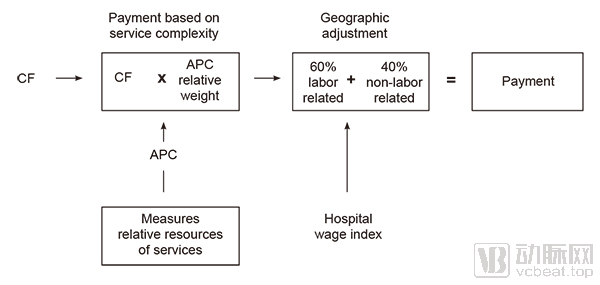
Payment Calculation Method of the U.S. APC Outpatient Payment System, Screenshot from the CMS Official Website
Subsequently, the actual payment amount is calculated by multiplying the pre-adjustment national group rate by the geographic practice cost index (GPCI). The adjustment primarily consists of two major components, with the local healthcare worker wage index being the most significant, accounting for 60% of the total adjustment factor.
In addition, the Centers for Medicare & Medicaid Services (CMS) provides certain adjustments for specific types of hospitals. First, teaching hospitals receive additional payments because they offer more comprehensive and complex services, which typically incur significantly higher costs than those of ordinary community hospitals. Therefore, teaching hospitals are eligible for extra compensation.
Second are hospitals with a public-welfare orientation, primarily serving low-income populations. Since the United States does not have mandatory health insurance coverage and hospitals cannot refuse to treat uninsured patients, such public-welfare hospitals may receive additional compensation to maintain basic medical service coverage.
In addition, CMS has established additional compensation provisions for special circumstances, such as outlier cases exceeding the payment cap, rural sole community hospitals (Rural SCHs) with no other healthcare facilities in the vicinity, and referrals involving designated children’s hospitals and cancer hospitals.
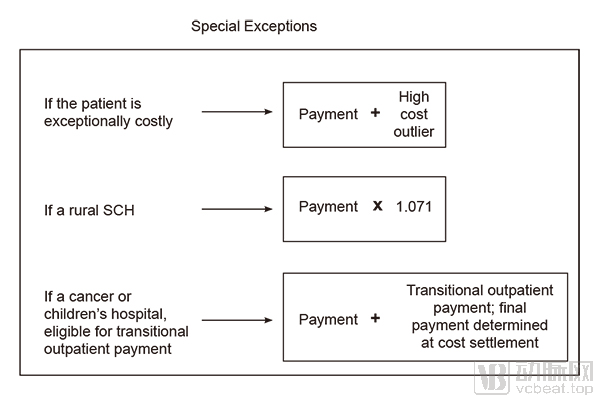
Calculation Methods for Certain Special Payments Under the U.S. APC Outpatient Payment System, Screenshot from the CMS Official Website
Each year, the Centers for Medicare & Medicaid Services (CMS) reevaluates Ambulatory Payment Classification (APC) groups and their relative weights, primarily based on changes in hospital practices and medical procedures, advancements in new technologies, the addition of new services and the elimination of outdated ones, reflection of updated cost data, and other relevant factors.
Furthermore, CMS has established dedicated New Technology APC groups. Services that meet the criteria for new technology APCs are assigned to these reserved new technology groups. The primary distinctions between these specialized new technology APC groups and standard APC groups are twofold: new technology groups reflect only costs, not clinical characteristics; and the payment rate for each new technology APC group is determined by its median cost rather than by relative weight.
In addition to the United States, Germany is also a country with a relatively mature application of bundled payments in healthcare financing. For outpatient services, Germany has a corresponding outpatient payment system. Broadly speaking, outpatient care in Germany is primarily provided by independent physicians and their clinics located throughout local communities.
Germany has a well-established tiered diagnosis and treatment system. General practice clinics located throughout the country serve as the first point of contact for outpatients. If further examination is required, patients are referred to the appropriate specialist clinics. Should these specialist clinics determine that they cannot manage the case, they will refer the patient to a hospital for further treatment.
In this process, both general practice clinics and specialty clinics fall within the scope of outpatient reimbursement. As patients referred to hospitals often require hospitalization or surgical procedures, outpatient examinations and related services provided by hospitals are reimbursed in accordance with the outpatient fee schedule periodically reviewed and published by the German Hospital Federation.
Final payments are allocated among general practice clinics, specialty clinics, and hospitals throughout the entire care continuum, based on algorithms that reflect their respective service volumes. For instance, if a specialist participates in post-referral surgeries at a partner hospital, the professional fees for the surgical services will be paid to the specialist, while costs related to equipment and team support will be paid to the hospital. Therefore, to maximize income, specialists typically establish collaborative relationships with hospitals, leveraging the hospitals’ equipment and multidisciplinary teams to perform surgeries.
In brief, Germany’s outpatient and inpatient funds operate independently but are subject to a shared global budget, creating a competitive dynamic. Specifically, if the outpatient fund’s expenditures fall below budget while the inpatient fund’s exceed it in a given year, the outpatient budget will be reduced and the inpatient budget increased in the following year.
“Therefore, although general practice clinics and specialty clinics have a certain competitive relationship throughout the process and require point-based allocation, under normal circumstances, general practice clinics will refer patients to specialty clinics rather than directly to hospitals, based on the shared goal of expanding the outpatient care fund pool. In this way, tiered diagnosis and treatment naturally takes shape,” said Wang Qian, a German DRG expert and Executive Director of Aceso Health.
In Germany, outpatient reimbursement is also divided between statutory health insurance and private health insurance, with both systems employing a point-based method to calculate payments. The key difference lies in the point value: generally, the point value for private health insurance is higher than that for statutory health insurance, and it applies higher weighting coefficients based on service volume and complexity.
Wang Qian, a German DRG expert and Executive Director of Aceso Health, offered an illustrative interpretation: “For example, during blood draws, we sometimes encounter patients with very fine veins that require multiple attempts, which is time-consuming and labor-intensive. For patients covered by commercial insurance or paying out-of-pocket, clinics can reasonably charge a higher markup. However, statutory health insurance reimbursement does not include such an adjustment factor; the payment remains the same for patients whose blood is easy to draw as for those for whom it is difficult.”
Meanwhile, private health insurance imposes far more lenient controls on cost ceilings than statutory health insurance. Consequently, some clinics in Germany choose to accept only privately insured or self-paying patients to achieve higher revenues. However, statutory health insurance has stricter accreditation requirements, mandating that clinics obtain the corresponding qualifications.
Unlike commercial insurance, which pays clinics and physicians directly, Germany’s statutory health insurance funds—equivalent to China’s basic medical insurance—do not make direct payments to contracted physicians or clinics. Each year, the statutory health insurance funds first negotiate with the National Association of Statutory Health Insurance Physicians (KBV) and its regional Associations of Statutory Health Insurance Physicians (KVs) to determine the per-capita fee for each insured individual at both the federal and regional levels. The total outpatient care payment budget for each region is then finalized based on the total number of insured individuals.
KBV then allocates the budget internally and provides corresponding compensation based on factors such as physicians’ specialties, the age demographics of the patient population served, and the total volume of services, thereby preventing excessive income disparities among physicians in different specialties.
KBV allocates funds each quarter based on the outpatient records submitted by physicians. Subsequently, the Physicians’ Association provides corresponding compensation payments to physicians according to their workload. The reimbursable services and their respective point values are stipulated in the statutory “Uniform Evaluation Standard for Federal Medical Services.”
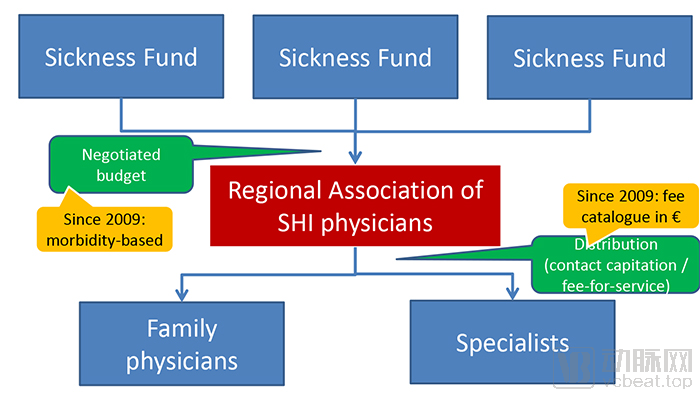
German Outpatient Payment System, screenshot from Wilm Quentin’s presentation slides
In calculating the point value, Germany initially adopted the floating-point method. The value per point was determined based on the previously established global budget for capitation payments and the calculable total number of points for outpatient services. The reimbursement payable to a physician was calculated by multiplying the point value by the number of points eligible for compensation.
This approach is characterized by “determining expenditures based on revenue,” delivering remarkable cost-control results and generally precluding overspending. Outpatient attending physicians are unaware of the monetary value of each point in advance, which can theoretically help curb overtreatment to some extent.
However, in practice, it has been observed that as the total number of points increases, point devaluation becomes increasingly severe. To compensate for this depreciation in point value, physicians often choose to increase the volume of medical services provided, which, to some extent, further exacerbates point devaluation. This gradually leads to a situation where physicians deliver more medical services while their income remains virtually stagnant.
To address this issue, since 2000, Germany’s statutory health insurance funds have adopted a fixed-point value system for outpatient reimbursement. Under this system, the point value is determined through prior negotiations between the National Association of Statutory Health Insurance Physicians (KBV) and the health insurance funds, based on the total volume of physician services and the age structure of the insured population. To compensate for the depreciation of point values, the point value is appropriately increased each year.
Since the initially assigned point value was low, it failed to reflect the true cost of medical services. Beginning in 2009, following negotiations, the point value for outpatient payments under the statutory health insurance fund has been increased nearly every year based on precise calculations.
Excess expenditures are generally not entirely denied payment; however, overall, overpayment does not offset actual costs. Therefore, such negative incentives reduce the likelihood of overutilization of medical services. Similar to the U.S. APC system, Germany’s outpatient payment system also incorporates buffer mechanisms for new technologies. New technologies can be reimbursed separately and subsequently incorporated into classification groups during the annual update process.
Wang Qian, a German DRG expert and Executive Director of Aceso Health, believes that Germany’s outpatient payment system has achieved its intended effects, primarily in three aspects.
First, Germany’s outpatient payment system has played a beneficial role in patient triage by keeping services that do not require hospitalization within the outpatient setting, thereby demonstrating excellent cost-containment effects. Meanwhile, through long-term communication and review by expert panels, the outpatient and inpatient payment systems have established mutually recognized referral criteria.
Secondly, Germany’s outpatient payment system has promoted internal development and communication within the entire outpatient care system. General practitioners and specialists engage in regular communication. In addition to routine technical exchanges, the outpatient system also balances point values with service volumes, thereby reducing the risk of point devaluation caused by indiscriminate increases in service volume.
Finally, there is the improvement in medical efficiency. Under the previous fee-for-service system, outpatient clinics could increase service payments by splitting items and prolonging treatment cycles. The German outpatient payment system has standardized the clinical practices of outpatient healthcare providers through reforms and optimization, fundamentally eliminating such undesirable behaviors.
It is evident that the design of Jinhua’s outpatient payment system largely draws on the frameworks and structures of those in the United States and Germany. However, it incorporates certain distinctive features in its specific design, overall resembling the German outpatient payment system more closely.
Compared with the US APC system, both the German outpatient payment model and the Jinhua APG point-based method incorporate global budgets to prevent fund overspending. In fact, the absence of a global budget is the most criticized aspect of the US APC system, directly leading to its poor cost-containment effectiveness. Without budgetary constraints, all compliant expenses are reimbursable, allowing hospitals and physicians to simply increase service volume to secure higher payments.
Compared with Germany’s outpatient payment system, Jinhua’s Ambulatory Patient Groups (APG) also adopt a regional global budget calculated on a per-capita basis. However, unlike Germany’s exclusive reliance on the service point value method, Jinhua’s outpatient payment system differentiates between enrolled and non-enrolled patients based on local conditions. Payments for enrolled patients are made through capitated lump-sum arrangements, while payments for non-enrolled patients follow the APG point-value method. This approach aims to integrate objectives such as tiered diagnosis and treatment, health management, and outpatient cost containment.
In many foreign countries, health management is often directly linked to beneficiaries’ premium expenditures or accompanied by corresponding financial incentives. In such cases, beneficiaries are typically motivated to improve their lifestyle habits to maintain physical and mental well-being. Meanwhile, health management funds abroad are usually independent and accounted for separately from outpatient services. In the United States, which adopts a capitation-based payment model, all medical expenses—including outpatient care, hospitalization, and rehabilitation—are incorporated into the per-capita payment through actuarial calculations. Even if hospitals incur losses on certain services, these can be offset by managing costs in other areas.
Due to differing national conditions, China’s basic medical insurance system does not currently provide a separate pooled fund for health management. Consequently, the Jinhua outpatient payment pilot program has opted to endow the outpatient fund with corresponding health management functions. While the original design intent was commendable, hospitals are in fact unable to enforce mandatory measures on patients, thereby shifting the burden that should rightfully be borne by beneficiaries onto healthcare institutions. The presence of a certain proportion of unhealthy patients among the enrolled population, or the occurrence of unforeseen circumstances, can significantly increase the likelihood of deficits in the capitation-based payments received by healthcare institutions.
This will lead to hospitals skimping on medical services, or even shirking responsibility for patients, thereby reducing the number of contracted patients. In effect, this represents a strategic preference for the APG point-based payment method to mitigate the risk of losses. As a result, the originally intended functions of tiered diagnosis and treatment and health management will be significantly undermined.
“Healthcare providers can only exert an indirect influence on patients and cannot mandate insured individuals’ health behaviors or dietary habits. Therefore, it is unreasonable to impose liability consequences on service providers. For instance, if all 1,000 insured individuals enrolled with a family physician are obese and engage in unhealthy lifestyle habits such as drinking, smoking, and physical inactivity, the family physician would face a high probability of financial loss under a capitation payment model. Consequently, they would likely opt out of capitation in favor of a point-based payment system, which at least ensures they do not incur losses. This undermines the original intent of the system design,” explained Wang Qian, Managing Director of Aceso Health and a German DRG expert.
“From the perspective of health management objectives, given the inherent shift in responsibility flows, it is more reasonable for payers to enter into agreements directly with insured individuals. For instance, if an insured individual declines additional preferential health programs, resulting in increased medical service utilization, they must bear the corresponding consequences. Conversely, upon achieving specified health targets, they may receive certain rewards,” Wang Qian further added.
Determining the base rate for partial calculations using the APG point system is also a distinctive feature of the Jinhua APG model. The Jinhua APG employs a floating-point method for calculating point-based rates, meaning that the monetary value per point is not fixed but depends on the current budget and the total number of points accumulated in the region; consequently, the point value may fluctuate, being either higher or lower. As this approach is budget-based, it generally prevents overspending and demonstrates effective cost containment. This has been well demonstrated in both German outpatient payment systems and the practical application of the Jinhua DRG point system.
However, practice in Germany reveals that under the floating-point method, clinics cannot calculate their applicable reimbursement rates prior to settlement due to the non-fixed point values. In such scenarios, clinics tend to increase service volumes to accumulate more points, thereby hedging against the risk of potential depreciation in point value. Consequently, this often leads to actualized point devaluation; although clinics provide more services, they do not receive proportionally higher payments, and their revenues may even decline. Over time, this undermines hospital incentives and hinders the further advancement of payment reform.
“For example, if the outpatient care fund had a budget of RMB 1 billion shared among 200 clinics, with the total number of points amounting to approximately 100,000, the point value under the floating-point system would be calculated as RMB 1 billion divided by 100,000. Providers tended to believe that by delivering more services, they could secure a larger share of the fixed budget. As a result, the service volume might double in the following year, reaching 200,000 points, while the total budget would likely remain largely unchanged. Consequently, the point value would then become RMB 1 billion divided by 200,000.” Wang Qian, Executive Director of Aceso Health and a German DRG expert, noted that the floating-point system has its inherent limitations.
In addition to Germany’s outpatient payment system, the United States also previously adopted a floating-point method in its physician payment system, which similarly led to point devaluation as physicians increased service volume to hedge against financial risk. Ultimately, the United States abolished the floating-point method. Therefore, from the perspective of positive incentives, whether and how to establish a base rate should become an essential consideration for the future.
Certainly, while the fixed point value method stabilizes point values, it is prone to imbalances between global budgets and fixed point values. In Germany’s outpatient payment system, point values are determined through negotiations between the National Association of Statutory Health Insurance Physicians (KBV), which represents physicians, and health insurance funds, taking into account the balance between global budgets and hospital service volumes—a model worthy of reference. Furthermore, some experts suggest that a combination of global budgets and population-based payments could be explored.
There are also differences in the setting of adjustment factors. In the United States, the primary adjustment factor for Ambulatory Payment Classifications (APCs) is mainly determined by local healthcare workers’ wage levels, with relatively less weight given to hospital-specific variations. Germany, by contrast, adopts a negotiation-based approach between its inpatient and outpatient systems, allocating budgets and providing corresponding compensation internally based on factors such as physicians’ specialties, the age distribution of the served population, and the total volume of services, thereby preventing excessive income disparities among specialists in different fields. Overall, both approaches aim to achieve tiered diagnosis and treatment as well as relative equity.
The differentiation coefficient for Jinhua’s APG is calculated based on the average cost per APG case across hospitals of different tiers. Its original intent was to acknowledge the real-world disparities in resource consumption among hospitals of varying levels. However, given that tiered diagnosis and treatment has not yet become a reality, this differentiation coefficient ensures that the high costs incurred by large tertiary hospitals do not lead to financial losses. Under such conditions, tertiary hospitals have little incentive to refer patients with common diseases to primary care institutions. Meanwhile, primary care hospitals are forced to compete at lower prices, which hinders the implementation of tiered diagnosis and treatment and may, in the long run, lead to risks of insufficient medical services or the shifting of patient costs.
Meanwhile, since the allocation of non-contracted funds is based on a points-based ratio, the presence of differentiation coefficients may further concentrate resources in large hospitals, which is also detrimental to the implementation of tiered diagnosis and treatment. Therefore, some experts suggest that after the current mechanism has been piloted for a period and the data have been further refined, consideration could be given to adjusting the differentiation coefficients to favor primary care hospitals for common disease groups, thereby promoting tiered diagnosis and treatment.
In this regard, the National Healthcare Security Administration’s (NHSA) CHS-DRG pilot evaluation conducted at the end of last year also noted that national standards should progressively advance toward “equal pricing for the same disease (group) across hospitals of the same tier,” and ultimately toward “equal pricing for the same disease (group) within the same city.” Undoubtedly, this will require a certain amount of time. In Germany, it took five years to transition from institution-specific DRG rates to unified rates at the state level, while the unification of outpatient payment rates took even longer.
Compared with DRG, the implementation of APG is more challenging. This requires medical institutions to possess high diagnostic and treatment efficiency, standardized technical protocols, advanced medical capabilities, and well-developed infrastructure. Meanwhile, support from local medical insurance policies is also indispensable. Given that most regions across China are still in the exploratory phase of implementing DRG, it will be difficult to roll out APG in the short term. Jinhua’s pioneering pilot program for outpatient APG demonstrates both the region’s strong healthcare service capacity and the bold exploration undertaken by its medical insurance authorities.
In terms of system design, Jinhua’s APG model draws on the structure of outpatient payment systems abroad while incorporating local innovations. For instance, it integrates capitation-based quota management for enrolled individuals, aiming to embed health management into the overall framework. Of course, the ultimate effectiveness of these design features will require time to evaluate.
No reform can be achieved overnight; all require optimization and adjustment through iterative practice. It is certain that following the implementation of DRG, outpatient payment reform will soon follow. VCBeat will continue to closely monitor these developments.
Editor’s Note: We extend our sincere gratitude to the readers of VCBeat for their invaluable assistance during the preparation of this article.
References
Zhu Mingjun: “The Payment System for Statutory Health Insurance in Germany”
Jinhua Release: “This Health Insurance Reform Is Being Implemented Across the Entire Jinhua Region! Authoritative Interpretation Released”
CMS:Hospital Outpatient Prospective System
PD.Dr.med Wilm Quentin, MSc HPPF:Health care purchasing and payment systems in Germany
Paul·L·Grimaldi:Untraveling Medicare’s Prospective Payment System for Hospital Outpatient Care