First-Ever MSI Detection Kit Approved in China: Transforming Personalized Cancer Therapy
Since the clinical diagnosis and treatment of tumors transitioned from the era of radiotherapy and chemotherapy to that of targeted therapy and immunotherapy, classifying tumor types by biomarkers has gradually become a parallel approach to the traditional classification based on primary organs. In the indications for an increasing number of new oncology drugs, it is no longer common to simply list “Stage * cancer”; instead, terms such as “Stage III lung cancer with EGFR gene mutations” and “Stage III breast cancer with HER2 gene mutations” have emerged.
In 2017, the FDA approved pembrolizumab for the treatment of patients with unresectable or metastatic solid tumors that are deficient in mismatch repair (dMMR) or exhibit high microsatellite instability (MSI-H) and have been previously treated. This marked the first pan-cancer oncology drug worldwide whose indication was defined directly by a biomarker, granting regulatory endorsement to microsatellite instability (MSI), a prominent biomarker in tumor immunotherapy.
Microsatellites, or short tandem repeats (STRs) in the human genome, include mononucleotide repeats, dinucleotide repeats, and even repeats of larger nucleotide units. Microsatellites are distributed throughout the human genome, with approximately 19 million currently identified.
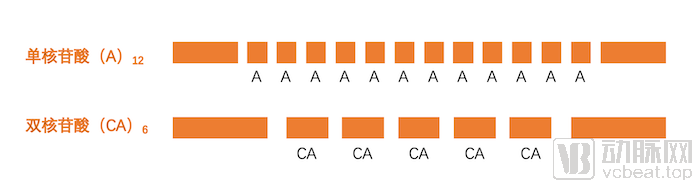
Schematic Diagram of Microsatellites in the Genome
In 1997, the U.S. National Cancer Institute (NCI) first defined microsatellite instability (MSI). MSI refers to alterations in microsatellite length caused by insertions or deletions of microsatellite repeat units in tumor tissues compared with normal tissues. It is the fifth most common type of mutation in tumors. MSI-High (MSI-H) tumors are those exhibiting a phenotype of high microsatellite instability.
According to statistics, there were approximately 4.5 million new cancer cases in China in 2015. For patients tested as MSI-H (microsatellite instability-high), the applicable tumor treatment regimens often differ from those for patients without such mutations. Consequently, an increasing number of genetic testing companies in China have begun offering MSI testing services to cancer patients; however, no MSI testing products with regulatory approval have been launched on the market.
This situation persisted until 2021. In late January, the National Medical Products Administration (NMPA) approved TumorShu Genomics’ application for the “Microsatellite Instability (MSI) Detection Kit (Multiplex Fluorescent PCR-Capillary Electrophoresis Method).” This kit is the first MSI detection kit to receive NMPA approval in China, providing a reference basis for clinicians to formulate individualized diagnosis and treatment plans. Four years after its establishment, TumorShu Genomics has secured the first certification for MSI testing. What was the regulatory approval pathway behind this achievement? With the first certification granted, how will MSI testing and precision oncology undergo transformation? Recently, VCBeat conducted an exclusive interview with Yan Linghua, founder of TumorShu Genomics, to explore these questions.
When we discuss tumor gene mutations, we typically refer to point mutations, insertions/deletions (indels), fusions, and amplifications. Such genetic alterations often lead to functional abnormalities in one or two genes, thereby disrupting signal transduction within their respective pathways; malignant tumors arise and progress through this process. Tumors with high microsatellite instability (MSI-H) follow a similar pathogenic logic, albeit more complex.
Microsatellite instability (MSI) within coding regions leads to frameshift mutations, which trigger the functional inactivation of relevant genes. Given the vast number of microsatellites distributed throughout the genome, microsatellite instability affecting multiple genes results in functional abnormalities in numerous genes across various tumor-associated signaling pathways, thereby driving the onset and progression of MSI-H tumors.
MSI-H Phenotype
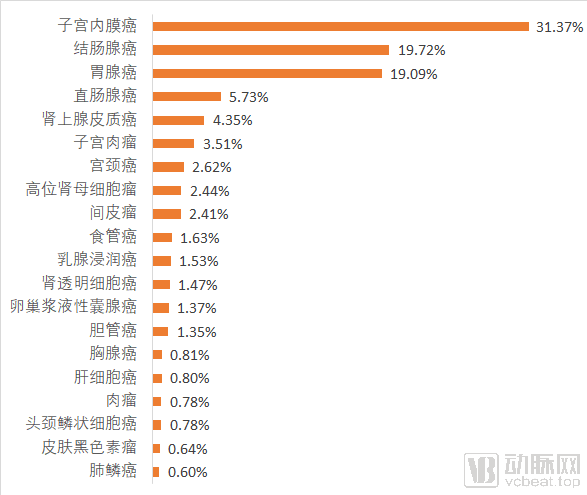
Proportion of MSI-H Patients Across Various Cancer Types
Based on estimates of the incidence rates of MSI-H across various cancer types, there are over 300,000 new cases of MSI-H tumors annually. This figure is comparable to the number of new breast cancer cases diagnosed each year and is significantly higher than that of other common malignancies, such as prostate cancer, thyroid cancer, ovarian cancer, and lymphoma. Meanwhile, patients with different types of MSI-H tumors often share similar clinical pathological and molecular pathological characteristics.
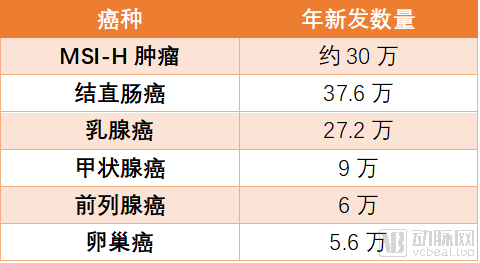
Comparison of Annual New Pathological Cases Between MSI-H Tumors and Other Cancer Types. Data Source: JCO Precis Oncol
For example, studies have shown that microsatellite instability (MSI) occurs predominantly in stage II colorectal cancer and in the proximal colon. MSI-High (MSI-H) tumors exhibit distinct clinicopathological features, including poor differentiation, mucinous components, lymphovascular invasion, and T-cell infiltration. Furthermore, MSI-H tumors share common molecular characteristics. Research indicates that MSI is frequently observed in patients with KRAS wild-type, BRAF mutations, PIK3CA mutations, and high tumor mutational burden (TMB-H). Gene mutations in specific pathways—namely MMR, WNT, PI3K, and NOTCH—are enriched in MSI-H tumors, irrespective of the tumor’s anatomical origin. In other words, MSI-H tumors constitute a unique entity characterized by distinct molecular pathogenic mechanisms and special clinicopathological and molecular features.
Thus, using MSI as a biomarker to differentiate tumor types serves two key purposes: on one hand, it identifies a large cohort of patients with similar tumor types who have differentiated therapeutic needs; on the other hand, patients with MSI-H tumors typically share similar clinicopathological and molecular pathological features, thereby assisting clinicians in formulating and optimizing comprehensive treatment regimens for this population. This constitutes the underlying rationale for the growing recognition of the clinical value of MSI testing.
MSI testing was first used in the screening for Lynch syndrome. Lynch syndrome, formerly known as hereditary non-polyposis colorectal cancer (HNPCC), is the most common type of hereditary tumor. MSI testing can serve as an initial screening tool for Lynch syndrome; for patients identified as MSI-H, germline mutation testing of the MMR genes associated with Lynch syndrome is performed to confirm the diagnosis.
Furthermore, MSI testing is widely used in clinical practice for prognostic assessment and prediction of adjuvant chemotherapy efficacy in tumors such as colorectal cancer and gastric cancer, thereby identifying patients who require further chemotherapy after surgery.
In recent years, the most prominent application of MSI testing has been predicting response to cancer immunotherapy.
Dingxiangyuan states in the *Encyclopedia of Microsatellite Instability* that microsatellite instability generates a large number of frameshift mutations, leading to shifts in the reading frame and causing subsequent changes in downstream codons. This results in the production of entirely different peptide chains, also known as “frameshift peptides” (FSPs). These FSPs act as neoantigens with high immunogenicity, eliciting an immune response from tumor-infiltrating lymphocytes (TILs). This explains one of the reasons why MSI-H tumors are sensitive to immunotherapy. Furthermore, MSI-H tumors are typically associated with high tumor mutation burden (TMB), and high TMB is also a marker of sensitivity to immunotherapy.
A clinical study in 2015 first demonstrated that patients with MSI-H colorectal cancer could benefit from pembrolizumab treatment. Subsequent multiple clinical studies have further expanded the scope of MSI-H patients who can respond to immunotherapy to more than 10 types of tumors. In other words, MSI testing has been proven to be a pan-cancer predictive tool for tumor immune response.
By 2020, the latest published results from the KEYNOTE-177 study demonstrated that pembrolizumab, as a first-line treatment for MSI-H metastatic colorectal cancer, offered both clinical and statistical significance compared to chemotherapy. These findings have further expanded the application of MSI testing in predicting tumor immune response. In the National Comprehensive Cancer Network (NCCN) guidelines for colorectal cancer diagnosis and treatment, MSI testing has been established as a mandatory procedure for selecting first-line therapies, and it is recommended for predicting immune response in more than 10 types of tumors.

Data on Clinical Application Scenarios of MSI in Major Cancer Types
Yan Linghua pointed out that, in theory, MSI testing is necessary for all patients diagnosed with colorectal cancer, gastric cancer, endometrial cancer, or small bowel adenocarcinoma; tumor patients requiring Lynch syndrome screening; and all patients with solid tumors seeking immunotherapy. Among these, MSI testing is primarily used in early-stage patients for prognostic assessment, Lynch syndrome screening, and guidance on adjuvant chemotherapy, whereas in advanced-stage patients, it is mainly employed to predict response to immunotherapy.
In the early stage, due to the absence of registered products on the market, MSI testing was primarily conducted through Laboratory Developed Tests (LDTs), with an annual capacity of approximately 100,000 cases in China. Yan Linghua told VCBeat, “This provides very limited coverage for the 300,000 patients with MSI-H status. We estimate that the annual clinical demand for MSI testing is 1.5 million cases.”
In MSI diagnosis, the configuration of the detection panel often determines the false-positive or false-negative rate of the test results. There are two internationally authoritative MSI detection panels. One is the NCI Panel, which consists of two mononucleotide loci (BAT-25 and BAT-26) and three dinucleotide loci (D2S123, D5S346, and D17S250), commonly known as the 2B3D Panel. The other is the Pentaplex Panel, which includes five mononucleotide microsatellite loci: BAT-25, BAT-26, NR-21, NR-22, and NR-24.
Since late 2016, Tree Genetics has collaborated with leading domestic oncology experts to conduct clinical studies on microsatellite instability (MSI), accumulating MSI testing data from over 20,000 patients and publishing nearly 30 academic papers. In Yan Linghua’s view, the core significance of these research findings lies in validating the efficacy of the 2B3D Panel for MSI detection in the Chinese population, thereby providing evidence-based support for the development of additional MSI testing products.
“Although the 2B3D panel is recognized as an authoritative standard by many international guidelines, the evidence supporting these consensus recommendations is based on data from European and American populations, whose genetic characteristics differ from those of the Chinese population,” pointed out Yan Linghua. “Tongshu Gene conducted three clinical studies to address which MSI detection panel should be adopted for the Chinese population.” The three clinical studies included: a head-to-head comparative analysis of the NCI panel and the Promega panel; a comparative study of the NCI panel, the Promega panel, and a 24-locus panel; and a study on tumor heterogeneity comparing MSI testing with microdissection.
Clinical studies have demonstrated that the sensitivity of the NCI panel in the Chinese population is 18% higher than that of the Promega panel, while the 24-locus panel exhibits the lowest sensitivity. This indicates that selecting a greater number of loci for MSI testing does not necessarily yield better results; rather, it is essential to choose validated loci to enhance the detection rate. The third clinical study by TreeGenes further revealed that MSI testing is minimally affected by tumor heterogeneity, thereby confirming that MSI testing can provide higher-quality clinical evidence.
Yan Linghua’s rigorous oversight of the panel design for Tongshu Gene’s MSI testing may have seemed somewhat stringent. Only after extensive clinical validation did Yan Linghua finalize the development of an MSI detection reagent based on the 2B3D NCI Panel. During this period, Tongshu Gene did not offer commercial MSI testing services to patients, thereby upholding the objectivity of its clinical research. “Panel selection is critical to the development of MSI testing; any issues at this stage would make it difficult to ensure product quality,” emphasized Yan Linghua.
Currently, multiple domestic and international guidelines and consensus statements, including the Chinese Society of Clinical Oncology (CSCO) Guidelines for the Diagnosis and Treatment of Colorectal Cancer (2020 Edition), the Expert Consensus on Molecular Biomarkers in Colorectal Cancer (2018 Edition), the Chinese Expert Consensus on Clinical Diagnosis, Treatment, and Family Management of Hereditary Colorectal Cancer (2018 Edition), and the ESMO Consensus: Recommendations for Microsatellite Instability Testing in Immunotherapy and Its Relationship with PD-1/PD-L1 Expression and Tumor Mutational Burden (2019 Edition), all recommend using the 2B3D NCI Panel for MSI testing.
It is understood that TumorTree Genetics has assembled a dedicated team of nearly 20 professionals from its R&D, medical, and product departments to focus on clinical research for MSI testing. In addition to the three key panel studies mentioned above, TumorTree Genetics has also conducted a study on tumor incidence among approximately 3,000 MSI-H patients, exploring the prevalence of MSI-H in patients with colorectal cancer, gastric cancer, endometrial cancer, liver cancer, glioma, and other malignancies. Although research on tumor incidence in MSI-H patients is a niche field, it provides important references for guiding precision oncology in clinical practice. Furthermore, TumorTree Genetics has initiated prospective clinical studies on PD-1 inhibitor therapy in MSI-H patients. Data from enrolled patients have demonstrated a clear correlation between MSI status and the efficacy of PD-1 inhibitors.
Yan Linghua candidly stated that since the inception of Tongshu Gene, his goal has been to develop compliant diagnostic products. In Yan’s view, in vitro diagnostics (IVD) companies should position themselves as providers of user-friendly diagnostic tools for physicians; only by effectively serving physicians can they ultimately benefit patients. Microsatellite instability (MSI) testing is one such strategic direction.
The original intention behind Tongshu Gene’s development of its MSI testing product was closely tied to Yan Linghua’s father’s experience with cancer. More than a decade ago, Yan Linghua’s father was diagnosed with advanced gastric cancer. During the second cycle of a planned six-cycle postoperative adjuvant chemotherapy regimen, he experienced severe adverse reactions. Yan Linghua keenly suspected that his father might be microsatellite instability-high (MSI-H), and thus unlikely to benefit from adjuvant chemotherapy. Subsequent testing confirmed Yan Linghua’s hypothesis, leading to the discontinuation of adjuvant chemotherapy. His father remains in good health to this day. “At that time, I was convinced that MSI testing was truly needed by the broad population of patients with gastrointestinal tumors,” said Yan Linghua. “Our goal is to ensure that every patient who requires MSI testing receives qualified MSI testing.”
Therefore, after selecting the 2B3D NCI Panel and initiating the relevant validation processes, TumorTree Genomics promptly engaged with regulatory authorities and clinical experts to demonstrate that the assay kit could achieve an accuracy rate of 99%, or even 100%, in large-scale clinical applications. “This means that from the R&D stage onward, we must develop products that score 100, or even 120 out of 100; otherwise, failure at the registration testing stage is inevitable,” stated Yan Linghua.
Tongshu Gene’s registration submission materials include clinical trial data from over 1,000 patients; however, early primer selection and methodological validation involved more than 10,000 MSI tests. In accordance with regulatory requirements, Tongshu Gene validated its MSI detection kit using multiple comparative methods, including Sanger sequencing, immunohistochemistry (IHC), and next-generation sequencing (NGS).
In clinical practice, in addition to the gold-standard method of PCR combined with capillary electrophoresis for assessing microsatellite instability (MSI) status, immunohistochemistry (IHC) is also commonly used to detect mismatch repair (MMR) proteins, thereby indirectly reflecting MSI status.
MSI status results from functional abnormalities in MMR proteins. The principle of IHC is to reflect MSI status by detecting the expression of four major proteins (MLH1, MSH2, MSH6, and PMS2) in the MMR system. The IHC method is low-cost, time-efficient, and widely adopted in pathology departments of medical institutions in China. Studies have shown that the concordance between IHC and PCR combined with capillary electrophoresis can exceed 85%.
However, the interpretation of immunohistochemistry (IHC) places high demands on pathologists, and test results are susceptible to subjective bias, leading to false negatives and false positives. Furthermore, the selection of primary antibodies in IHC is critical for determining positive and negative outcomes, while the operational procedures are difficult to standardize, thereby compromising the reproducibility of IHC results and affecting diagnostic accuracy. Therefore, Yan Linghua believes that combining PCR with capillary electrophoresis and IHC represents a more reliable approach for microsatellite instability (MSI) testing under current conditions.

Comparison of MSI Detection Across Different Technical Approaches
In recent years, with the advancement of molecular biology and the reduction in next-generation sequencing (NGS) costs, whole-exome sequencing and multi-gene targeted panel sequencing have gradually been applied to the detection of microsatellite instability (MSI). NGS offers high throughput and sensitivity, enabling the simultaneous assessment of thousands of MSI loci, mismatch repair (MMR) gene status, and other molecular biomarkers using an NGS panel. However, according to Yan Linghua, given the greater complexity of NGS data analysis, it is essential to establish standardized algorithms and evaluation criteria for MSI assessment. Furthermore, broader clinical adoption of this approach requires further accumulation and validation of data specific to the Chinese population.
After the MSI product reached its preliminary design finalization, Tongshu Gene spent nearly six months designing its clinical trials. During this period, they repeatedly communicated with industry experts and, leveraging previously accumulated research data, secured participating medical institutions for the registration-enabling clinical trials on a case-by-case basis.
Yan Linghua told VCBeat that he was deeply grateful for the experience of registering and filing Tongshu Gene’s MSI product, from which he learned a great deal. “This process demonstrated that everyone acted with a sense of responsibility toward patients; this is exactly how we should proceed.”
In an exclusive interview with VCBeat, just one week after the National Medical Products Administration (NMPA) officially approved Tongshu Gene’s MSI testing product for market launch, Yan Linghua could barely contain his excitement. “The approval of this product will inevitably bring profound changes to the MSI testing market. However, I believe what is more significant is that patients with MSI-H tumors are now one step closer to receiving more precise clinical treatment regimens,” said Yan Linghua. “First, stability: performing MSI testing within hospitals is undoubtedly more reliable. Second, timeliness: previously, samples for MSI testing had to be sent out for centralized analysis, with results returned after 4–5 days. In contrast, in-hospital MSI testing can deliver results as quickly as on the same day.”
Following the market launch of the test kit, MSI testing will deliver greater clinical value. For instance, in predicting tumor immune response, the National Health Commission mandates that only qualified diagnostic reagents be used to guide the administration of antineoplastic agents. Cancer patients selected for immunotherapy often present with critical conditions and face high drug costs; employing compliant MSI testing provides protection for both physicians and patients.
Currently, Tongshu Gene has assembled a 20-member commercial team and aims to distribute its MSI testing reagents to medical institutions across China within the next two to three years. According to Yan Linghua’s projections, there are at least 200 medical institutions in China capable of performing MSI testing. Based on an estimated annual volume of 1,000–1,500 MSI tests per institution, MSI testing reagents are poised to become the single most in-demand diagnostic product in the field of precision oncology.
Based on feedback from clinical practitioners, there is a strong clinical demand for MSI testing; however, the lack of compliant products on the market has made it difficult for many hospitals to make selections. Since the product registration certificate was granted, TumorTree Genomics has received numerous procurement intentions from medical institutions. “Therefore, the approval of the product registration certificate will provide strong momentum for increasing the volume of MSI testing samples from 100,000 to 1.5 million,” speculated Yan Linghua. He added that following the issuance of the first certificate, more MSI testing reagents are expected to become available, fully meeting the clinical demand for MSI testing.
For Tree Genetics, obtaining the registration certificate for its MSI testing product marks a significant milestone in the innovation and exploration of precision medicine, but it is by no means the end. Yan Linghua stated that, while vigorously promoting the rapid clinical adoption of its MSI testing reagents to meet clinical demand, Tree Genetics will continue to exert effort in two other areas of oncology precision medicine, striving to achieve key breakthroughs in ctDNA and large-panel tumor NGS testing in the future.
Writing Reference:
DXY: Encyclopedia of Microsatellite Instability
Tumor Time: Microsatellite Instability—A Tumor Marker That Cannot Be Ignored
Chunyu Doctor: Microsatellite Instability (MSI) Testing in Colorectal Cancer and Its Clinical Significance