Enhancing Medical Record Quality: How Informatics Empowers National Healthcare Standards
On February 20, the Bureau of Medical Administration and Hospital Management of the National Health Commission released the “2021 National Goals for Improving Medical Quality and Safety” (hereinafter referred to as the “Goals”) on its official website. The “Goals” represent the annual national objectives for improving medical quality and safety put forth at the state level. They not only summarize and analyze China’s current status of medical quality and safety and apply the resulting insights, but also serve as an important means to further focus on weak links and key areas in medical quality and safety, clarify the direction for industry-wide improvements, and enhance the scientific, standardized, and refined management of medical quality and safety.

Screenshot from the official website of the National Health Commission
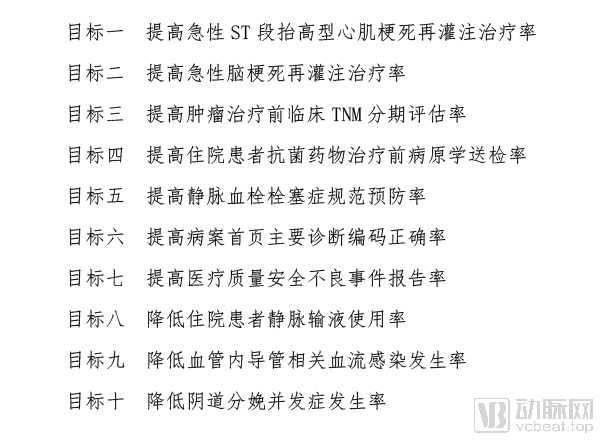
The current edition of "Goals" establishes ten national goals for improving medical quality and safety, the majority of which pertain to clinical treatment. The content related to healthcare informatization primarily focuses on Goal 6: "Improving the Accuracy of Primary Diagnosis Coding on the Front Page of Medical Records." This indicator plays a foundational and critically important role in DRG (Diagnosis-Related Groups) and subsequent payment reforms.
The front page of the medical record serves as a summary of the patient’s inpatient diagnosis and treatment, representing the most concentrated, significant, and core component of the entire medical record. It essentially encompasses all basic patient information and all data required for Diagnosis-Related Group (DRG) classification—including demographic details, hospitalization process information, diagnostic and therapeutic information, and cost information—thereby forming the basis for DRG implementation.
Globally, the development of Diagnosis-Related Group (DRG) systems, as well as the accurate grouping and determination of weights, relies on two types of foundational data: first, clinical information contained in medical record face sheets, including diagnosis codes and procedure codes; and second, cost information derived from medical records.
During the DRG grouping process, physicians or coders must determine the appropriate DRG category for each case based on clinical information; assess whether the homogeneity within different DRG categories is sufficiently high based on DRG cost data; and decide whether further subdivision into separate groups is warranted if homogeneity is inadequate. Therefore, the collection and analysis of data from the medical record face sheet are critical to accurate DRG classification and weight determination.
DRG grouping is primarily based on data from the inpatient medical record face sheet, including principal diagnosis, secondary diagnoses, and surgical procedures. Although DRG versions across different countries and regions incorporate localized designs tailored to local characteristics, their overall grouping logic and methodology are largely similar, generally involving a three-step classification strategy.
First, cases are classified by principal diagnosis to form Major Diagnostic Categories (MDCs), which are primarily characterized by anatomical and physiological systems. Then, cases are further subdivided into Adjacent Diagnosis-Related Groups (ADRGs) by comprehensively considering the principal diagnosis and principal procedure. Finally, ADRGs are refined into Diagnosis-Related Groups (DRGs) by taking into account other individual patient characteristics, comorbidities, and complications.
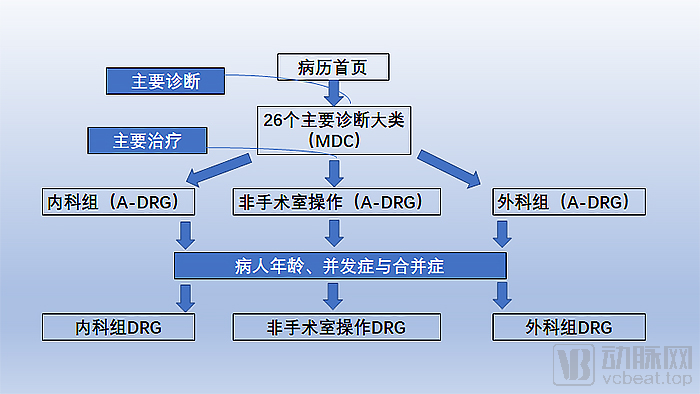
Throughout the entire process, MDC assignment typically relies solely on the principal diagnosis code; the classification from MDCs to ADRGs utilizes both the principal diagnosis code and the principal procedure code, while the further classification from ADRGs to DRGs incorporates additional diagnoses and procedures, as well as other variables reflecting individual patient characteristics. Consequently, the DRG grouping process imposes extremely high requirements on the quality of data in the medical record face sheet, particularly the coding data quality.
If the data on the medical record face sheet is filled out incorrectly, it will usually lead to errors in DRG grouping, thereby causing significant impact.
Taking the principal diagnosis as an example, DRG grouping first considers the patient’s principal diagnosis and determines the Major Diagnostic Category (MDC) for group assignment based on the principal diagnosis established by the attending physician.
The CHS-DRG Subgrouping Scheme Version 1.0, issued by the National Healthcare Security Administration, explicitly stipulates that the principal diagnosis refers to “the disease (or health condition) determined by the medical institution through diagnosis and treatment as the primary reason for the patient’s current hospitalization.” Specifically, it is the diagnosis that poses the greatest threat to the patient’s health, consumes the most medical resources, and results in the longest length of stay for the current hospitalization.
In the early stages, due to a limited understanding of the Diagnosis-Related Group (DRG) system, Beijing experienced a notable case during its DRG pilot implementation: a patient was hospitalized for nine months at a certain hospital for uterine fibroids, incurring exorbitant costs and triggering significant public outcry.
Investigation revealed that the patient was indeed hospitalized for uterine fibroids; however, lung cancer was detected during preoperative examinations. The patient was subsequently transferred to the Oncology Department for treatment of lung cancer and later returned to the Gynecology Department for management of uterine fibroids. Following a hysterectomy, the patient developed deep vein thrombosis in the lower extremities. These cumulative factors resulted in a prolonged hospitalization lasting nine months.
In this example, a dual error occurred involving the principal diagnosis and combined hospitalization. First, two separate hospital admissions should have been recorded with different principal diagnoses. Subsequently, in accordance with the principles for determining the principal diagnosis, the two principal diagnoses should be assigned separately: lung cancer first, followed by uterine fibroids.
In addition to the principal diagnosis, the principal surgical procedure and other diagnoses listed on the medical record face sheet all influence DRG grouping. Inaccurate completion of the medical record face sheet can lead to erroneous coding and grouping, resulting in upcoding, undercoding, or omitted codes. Minor errors may lead to claim denials by health insurance payers, causing financial losses for hospitals; severe cases may result in repeated instances of unintentional health insurance fraud, subjecting the institution to regulatory penalties.
On August 2, 2019, the National Health Commission issued a special letter to criticize a tertiary hospital in Xi’an, pointing out serious inaccuracies in the medical record face sheet data submitted by the hospital. A large number of medical record face sheets contained identical information for primary diagnosis, primary surgical procedures, discharge status, and total hospitalization costs, resulting in reported rates of 100% for surgical procedures, minimally invasive surgeries, and Level 4 surgeries. These severe data discrepancies rendered it difficult to calculate indicators related to medical record face sheets.
Upon thorough investigation, it was confirmed that the original data from the hospital’s medical record face sheets had been tampered with to bypass the automated screening procedures of the information system. Although the data were successfully uploaded, they were inaccurate. Consequently, the relevant entities and responsible individuals received severe disciplinary actions.
According to statistics, the categories of issues arising from the front page of medical records and their underlying causes are mainly as follows.
The first category comprises diagnostic issues that reflect the severity and complexity of the patient’s condition, as well as data quality. The primary causes of these issues include: non-uniform diagnostic terminology on the front page of the medical record; errors, omissions, non-standardization, or incompleteness in the principal diagnosis; errors, missing entries, or non-standardization in secondary diagnoses; and missing or inaccurate individual factors such as age and gender.
The second category pertains to data quality reflecting the availability and utilization intensity of medical resources, such as issues related to surgical procedures. The primary causes of these issues include the lack of standardized nomenclature for surgical procedures on the front page of medical records; omissions or inaccuracies in documenting the primary surgery; omissions or inaccuracies in recording other surgeries or procedures; and missing data entries, such as completely blank fields for intensive care unit (ICU) stay duration and mechanical ventilation time.
Category 3 pertains to medical outcomes, specifically issues related to discharge status. Incorrect documentation of discharge status on the front sheet of the medical record (e.g., death, discharge against medical advice, discharge not against medical advice, or incorrect transfer information) leads to such issues.
The fourth category pertains to cost and time consumption, specifically cost-related issues. Such problems arise from errors in the medical record face sheet, such as surgical procedures being recorded with a surgical fee of zero, discrepancies between itemized charges and the total cost, or admission dates occurring after discharge dates.
Finally, there is the issue of coding. This includes coding selection errors resulting from incorrect completion of the medical record face sheet, as well as inconsistencies in the coding dictionary used during its completion.
Since 2008, China has strengthened statistical practices in accordance with the law by incorporating the medical record face sheet into the National Statistical Survey System. At that time, however, the data collection relied on the Patient Discharge Survey Form rather than the full-scale collection of medical record face sheets. This form included nearly 50 indicators, which constituted the core elements of the medical record face sheet. In 2013, following the implementation of the new medical record face sheet, it was integrated into the statistical survey system for comprehensive data collection. All fields of the medical record face sheet were collected, and the National Medical Record Face Sheet Database was established.
However, an assessment of the data quality of the submitted medical record face sheets at that time revealed significant variability across provinces, indicating substantial room for improvement. In fact, experience from other countries implementing Diagnosis-Related Groups (DRG) shows that the quality of hospital medical record face sheets is often unsatisfactory during the initial phase, a challenge that China has also been unable to avoid.
To rapidly improve the quality of medical record face sheets, the National Health Commission has incorporated this metric into performance evaluations in recent years. In 2019, both the performance evaluation for tertiary public hospitals and that for secondary public hospitals mandated improvements in the quality of medical record face sheets. Hospitals were required to complete these forms in accordance with unified national standards, strengthen quality control over the face sheets, and enhance the management of data quality for uploaded face sheet records, thereby ensuring the objectivity and authenticity of the evaluation data.
Meanwhile, the National Healthcare Security Administration has also leveraged payment mechanisms to compel hospitals to improve the quality of medical record front sheets. Once errors occur in the healthcare settlement list—which serves as the “healthcare insurance version” of the medical record front sheet—hospitals may face consequences ranging from denial of due reimbursement to administrative penalties. With financial interests directly at stake, hospitals have naturally placed greater emphasis on the quality of medical record front sheets.
Nevertheless, the quality of medical record front sheets in hospitals across China remains unsatisfactory. One reason why the National Healthcare Security Administration introduced Diagnosis-Intervention Packet (DIP) after launching CHS-DRG is that most hospitals generally struggle to achieve the required accuracy rate for medical record front sheets under DRG within a short period.
The current "Goals" further strengthen quality control of the medical record face sheet and propose two objectives.
First, improve the accuracy of principal diagnosis coding on the medical record face sheet. This plays a critically important foundational role in accurately compiling disease spectra for healthcare institutions and regions, supporting Diagnosis-Related Groups (DRG) classification, and evaluating the quality and safety of medical care as well as technical capabilities.
Second, the principal diagnosis on the hospital discharge summary must be documented correctly. This requires physicians and medical record management personnel to accurately select and standardize the entry of the principal diagnosis on the inpatient medical record face sheet in accordance with regulations, and to assign codes accurately using the nationally unified disease classification codes.
So, why is the work on hospital medical record face sheets such a persistent challenge?
The first line of defense in completing the front sheet of medical records is the clinician. However, clinicians often face heavy workloads and may have an inadequate understanding of coding practices. To save time, when no exact disease code is available, clinicians may use codes for similar conditions, leading to adjustments in diagnoses. This results in discrepancies between the patient’s actual condition and the diagnoses and treatments documented on the front sheet of the medical record. Alternatively, driven by financial incentives, some may alter medical records based on coding requirements, directly causing inaccuracies in the original information.
Meanwhile, many attending physicians who are responsible for completing the medical record front sheet delegate this time-consuming and labor-intensive task to resident physicians. These residents are often interns, visiting scholars, or standardized training physicians. However, due to their lack of sufficient experience, they are prone to making errors when filling out the medical record front sheet.
Numerous issues also persist within medical records departments during the quality control phase. A significant contributing factor is the heavy workload, insufficient staffing, and inadequate professional expertise within the medical records quality control units, coupled with the difficulty in recruiting or rapidly training qualified personnel, which hinders the effective execution of medical records quality control.
First, the workload is excessive. According to the 2010 revised "National Hospital Work Regulations, Hospital Management Systems, and Responsibilities of Hospital Staff," the ratio of personnel dedicated to inpatient medical record management to hospital beds in Grade II Class A hospitals and above shall be no less than 1:50; the ratio of personnel dedicated to outpatient medical record management to the average daily outpatient volume shall be no less than 1:300. However, the actual situation falls far short of these standards.
。
Compared with 2010, hospital management efficiency and bed turnover rates have increased rapidly today, while the workload for medical record quality control has further intensified; even when configured according to the highest standards, the regulations from 2010 can no longer meet current practical demands.
Secondly, the current medical records management staff lack sufficient professionalism. According to the requirements for medical records management personnel in the "Hospital Accreditation Standards," the proportion of non-related major personnel should be less than 20% at most, and even with relaxed requirements, it should still be less than 50% as the minimum requirement.
The reality is that hospital medical records departments lack professional technical personnel; most staff are transferred from nursing roles, and a small number are even non-medical contract workers, resulting in insufficient mastery of clinical knowledge.
Currently, there are no relevant professional qualification examinations in China. Only the training examination certificate issued by the Medical Records Professional Committee of the Chinese Hospital Association is widely recognized for its credibility. Although it does not constitute an official credential, it is required as a job qualification in certain regions. Based on historical data, more than 1,000 students enroll annually in coding and medical record quality control programs, with approximately 200 actually taking the examination, resulting in a pass rate of less than 50%.
Furthermore, quality control physicians and medical coders are required to possess a comprehensive understanding of clinical practices, as well as disease profiles and treatment modalities across various departments, entailing exceptionally high professional standards. In the early stages, nearly all domestic quality control experts in China had accumulated many years of clinical experience before transitioning to specialize in quality control. Such career paths are now extremely rare, leading to a concerning lack of successors among industry leaders.
Finally, the work intensity is excessively high. Based on the actual number of quality control personnel in hospitals, each individual must review more than 12,500 medical records annually to meet requirements, which translates to an average of over 50 medical records per person per day. In practice, however, due to the time-consuming nature of quality control tasks and the energy demands of other responsibilities, it is difficult for hospital staff to achieve this target on a daily basis, often limiting them to ensuring only basic substantive quality control. By comparison, coders in countries such as the United States and Australia are required to review only 4–5 medical records per day.
It is evident that, to improve the quality of medical record face sheets, the fundamental issue to be addressed is the human factor.
To rapidly achieve the goal of improving the quality of medical record face sheets, the "Goals" proposes four core strategies.
First, medical institutions should fully leverage the role of their Medical Record Management Committees, improve relevant management systems and mechanisms, and develop and implement technical guidelines for the standardized completion of medical record face sheets within their institutions, thereby further clarifying principles such as the selection of principal diagnoses and ICD coding.
Second, medical institutions shall strengthen training on the standardized completion and quality monitoring of the front page of medical records, so as to improve the ability of medical personnel to accurately document principal diagnoses and assign codes.
Third, establish an institutionalized, normalized, and multi-departmental collaborative monitoring and evaluation mechanism, conduct data analysis and feedback by quarter and by department, incorporate target improvement outcomes into performance management, and establish incentive and constraint mechanisms.
Fourth, apply quality management tools to identify and analyze factors affecting the institution’s achievement of this goal, propose improvement measures, and implement them.
These strategies have strengthened the emphasis that hospitals and physicians place on medical record face sheets from institutional, methodological, and ideological perspectives. Furthermore, given the reality that a substantial increase in workforce capacity is not feasible in the short term, leveraging information technology to enhance capabilities is undoubtedly a critical option.
Generally, informatics solutions for medical record quality control follow largely similar workflows: first, establishing management standards and quality control rules for medical records, and then implementing process management based on these rules to ensure that the quality of medical record face sheets meets the established management standards.
After establishing quality control management standards and rules, process management for quality control can be implemented on the medical record face sheet. Currently, most medical record quality control solutions offer IT systems featuring intelligent coding and comprehensive quality control of the medical record face sheet, supporting quality management throughout the entire creation process of the medical record face sheet.
The Intelligent Medical Record Coding System primarily leverages technologies such as big data, machine learning, and knowledge graphs to provide intelligent ICD coding. It helps hospitals improve the quality and efficiency of medical record coding by offering coding assistance and quality control in two key scenarios: coding during physicians' diagnosis and treatment processes, and formal coding by medical coders. This enables hospitals to shift coding and quality control upstream into clinical and diagnostic workflows.
This technology can significantly reduce the workload in the coding process, but its implementation is far from easy, primarily for two reasons. First, the underlying data quality in hospitals is poor, with medical records written by each physician varying considerably. Second, due to the high variability and complexity of the Chinese language, NLP word segmentation is much more challenging than in English, imposing stringent requirements on algorithms.
Addressing the pain points associated with the deployment and application of electronic medical records (EMRs) and medical record face sheets, Darui Jisi has adopted multiple measures to enhance medical record quality control. These measures provide comprehensive coverage across the entire workflow, including pre-event planning, in-process monitoring, and post-event analysis. Key functionalities include pre- and in-process grouping prediction, intelligent coding assistance during the process, data quality control during and after the process, as well as clinical decision support and pathway management.
This solution also provides comprehensive support for intelligent coding assistance for medical record front pages and clinical course documentation. Leveraging the latest AI machine learning and NLP (Natural Language Processing) technologies, it offers an integrated intelligent coding application programming interface (API). It can be seamlessly integrated into hospital information systems (HIS), electronic medical records (EMR), physician workstations, and other clinical workflows, thereby improving coding accuracy and efficiency while reducing the coding workload in hospitals.
In-process and post-event data quality control enables analysis of in-process quality control and post-event statistical audits for medical record front sheets and health insurance settlement lists. The solution embeds a vast library of quality control rules and supports hospital-based experts in independently defining and extending rules. Furthermore, it allows for custom quality control rules and automatically calculates scores in accordance with the regulations issued by the National Health Commission.
“The application of artificial intelligence in medical record front pages and clinical course documentation is highly targeted and valuable. Through big data training, AI can directly codify rules, providing targeted and effective support for hospitals in quality control during and after care,” affirmed Tan Xiaogang, Founder and CEO of Darui Jisi, recognizing the value of AI in medical record quality control.
Huoshu Technology, which specializes in MDT-based system solutions, provides a three-tier quality control system involving clinicians, medical records departments, and quality control departments. This approach shifts the quality control of medical record front sheets to the physician end, ensuring data quality at the source. Additionally, it introduces intelligent algorithms to build a diagnostic omission identification model, further improving coding accuracy. Meanwhile, it can also detect DRG-risk cases in real time and provide early intervention.
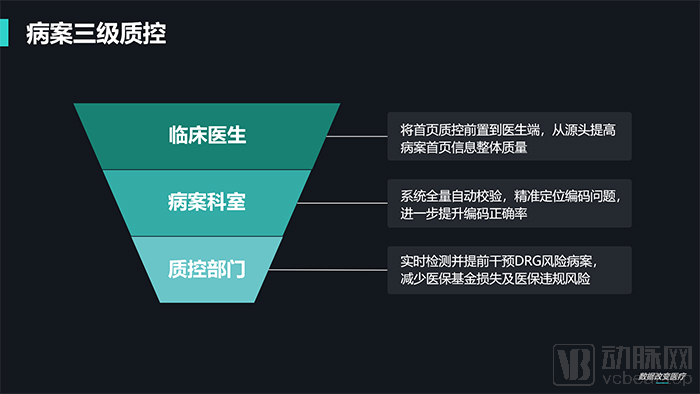
Medical Record Quality Control Information Solution Typically Adopts a Multi-Level System of Pre-, Intra-, and Post-Event Controls (Image from Huoshu Technology)
Following the introduction of CHS-DRG, the medical insurance settlement list will replace the previous role of the medical record front sheet. Huoshu has also keenly identified new directions for optimization and will implement targeted improvements in the future to address the specific characteristics of the medical insurance settlement list (such as the adoption of the medical insurance version of disease classification and procedure codes, and the emphasis on healthcare resource consumption), thereby ensuring a seamless transition for hospitals when switching to CHS-DRG.
The real-time pre-grouping function leverages rule engines, NLP technology, and correlation analysis to minimize the impact of DRG rules on physicians’ electronic medical record (EMR) documentation habits, shifting the completion of core grouping information to the inpatient period. Integrated with phased cost management, the solution divides the hospitalization process into distinct diagnostic and treatment stages and provides benchmark cost ranges by cost structure to serve as a reference for physicians.
“All intelligent judgments are fundamentally driven by algorithms, such as medical record quality control, in-hospital prediction, and real-time analysis of hospital data. Although we engage in these areas, we never hype up concepts like artificial intelligence. The healthcare sector requires long-term, steadfast dedication, so we place the greatest emphasis on practical implementation. Only with precise data can we deliver tangible value to hospitals,” stated Zhang Wei, CEO of Huoshu Technology.
Chen Xianli, Vice President of Wanghai Kangxin, stated that hospitals need to strengthen the quality of medical record data to ensure accurate coding that truly reflects medical practices, as the information for DRG or DIP payment compensation and case grouping results is derived from the front page of the medical record. Meanwhile, 15 performance indicators for public hospital assessments are directly sourced from the front page of the medical record. Therefore, the quality of the front page of the medical record serves as a crucial data foundation.
Wanghai Kangxin’s medical record quality control establishes a full-chain management system for the front page of medical records, spanning from pre-consultation documentation standards to intra-consultation quality control alerts and pre-coding, and finally to post-consultation quality control and intelligent coding. By leveraging the medical record quality control and ICD intelligent coding system, it enhances both the quality of medical records and coding efficiency.
“Wanghai Kangxin’s intelligent coding tool is embedded within the electronic medical record (EMR) system. Leveraging big data and AI technologies, it provides intelligent coding recommendations during diagnosis and treatment based on patient characteristics, diagnoses, procedures, and other factors, while automatically generating information for the medical record face sheet. Upon confirmation by the medical records department and clinical departments, the final medical record face sheet is produced.” Chen Xianli stated that Wanghai Kangxin’s intelligent coding system not only enables hospitals to perform coding more intelligently and accurately, thereby improving the quality of medical records, but also enhances the operational efficiency of the medical records department.
The medical record quality control module of Ping An Medical Insurance Technology’s DRG Integrated Management Platform also incorporates artificial intelligence technologies such as an intelligent coding engine, natural language processing (NLP), and medical knowledge graphs. It provides pre-event alerts for medical record documentation and real-time quality management during the process, offering grouping references to physicians while they document electronic medical records, thereby addressing issues at the source.
It also features post-discharge medical record quality control analysis, which effectively reduces common issues in the completion of medical record face sheets—such as incomplete data, non-standardized entries, arbitrary addition, deletion, modification, or substitution of data standards, and logical inconsistencies—through intelligent review.
Overall, these digital solutions have indeed played a significant role in improving the quality of hospital medical records. Prior to implementing medical record quality control programs, most hospitals had an early case grouping rate of only around 60%. However, within one to two months after launching these quality control initiatives, the rate rapidly increased to over 90%, substantially enhancing the data quality of medical record face sheets.
With the release of The Objectives, greater emphasis is being placed on the quality of medical record face sheets, which serve as the foundation for Diagnosis-Related Groups (DRGs). Given that the shortage of medical records personnel is unlikely to be resolved in the short term, hospitals will be compelled to undertake information technology upgrades. This shift will transform case review processes from post-hoc audits to pre-event reviews, thereby significantly improving the accuracy of medical record face sheet documentation and optimizing clinical workflows.
Information technology solutions can empower medical record quality control by leveraging big data, artificial intelligence, and other advanced tools. Recent policies clearly indicate that relevant institutions are further strengthening the data infrastructure to support the implementation of Diagnosis-Related Groups (DRG), ensuring that payment reforms led by DRG achieve their intended outcomes. This field is undoubtedly poised to enter a golden age of development in the near future.
Editor’s Note: Portions of this article are excerpted from the co-authored book Domestic and International Practices of DRG-Based Payment. The book is edited by Liu Zhichen, who served as a joint postdoctoral fellow at the Postdoctoral Mobile Station in Public Administration of Fudan University and the Postdoctoral Workstation of the Statistical Information Center of the National Health Commission, and currently serves as Chief Expert in the Healthcare Industry at China Unicom Group and a member of the Industrial Internet Expert Committee of China Unicom Group. The associate editors are Zhu Suisong, Director of the Network Technology Department at Shenzhen Nanshan Hospital, Adjunct Professor at Shenzhen University, and External Executive Leader; and Wang Qin, Secretary-General of the Health Insurance Working Committee of the Chinese Society for Health Informatics and Medical Big Data, and Deputy Director of the Life Insurance Department of the Insurance Association of China.
Reproduction without permission is prohibited.