PI3K Inhibitor Buparlisib Emerges as a Promising Breakthrough in Head and Neck Cancer Amid Limitations of PD-1 and EGFR Therapies
Head and neck cancers are a group of highly aggressive, heterogeneous tumors and represent the sixth most common cancer type worldwide. Among these, 90% are squamous cell carcinomas. Due to limited public awareness, the severity of head and neck cancers is often overlooked, resulting in 70%–80% of patients being diagnosed at locally advanced or advanced stages. This complicates treatment, and 50%–60% of patients experience recurrence within two years, ultimately leading to poor prognosis and high mortality rates.
According to the latest data from international research institutions, the number of new head and neck cancer cases in China reached 142,000 in 2020, with an incidence rate second only to thyroid cancer, which ranked eighth, showing a steady upward trend; the number of deaths approached 75,000.
The emergence of PD-1 monoclonal antibodies has introduced a novel therapeutic approach for head and neck cancer. In 2021, the indication for Opdivo (O drug) in head and neck cancer was officially approved in China. However, in the same year, a prestigious UK agency did not recommend Opdivo for patients with head and neck cancer.
Why Have PD-1 Monoclonal Antibodies Encountered a Complex and Contradictory Landscape in the Indication for Head and Neck Cancer? Which Targets Will Next Enter the Broad Market for Head and Neck Cancer After PD-1?
Historically, the treatment of head and neck cancers has relied primarily on surgery combined with radiotherapy and chemotherapy. However, surgical intervention in head and neck cancer presents significant technical challenges. On one hand, surgery is difficult to perform in certain specific subtypes, such as nasopharyngeal carcinoma. On the other hand, because the surgical site is located in the head and neck region, postoperative outcomes may adversely affect patients’ facial appearance, speech, and even swallowing function, thereby severely compromising their quality of life.
Compared with surgery, radiotherapy and chemotherapy are less restricted in the treatment of head and neck cancer. HoweverGiven the frequent recurrence and distant metastasis observed in patients, chemoradiotherapy can only control disease progression in the short term but fails to enable long-term survival with tumor burden.
When conventional therapies yield limited benefits, the advent of targeted therapy has provided patients with new treatment options. In 2006, the U.S. FDA approved Erbitux (cetuximab) in combination with radiation therapy (as first-line treatment) or as monotherapy (after standard treatment failure) for non-metastatic head and neck cancer. In 2011, its indications were further expanded to include use in combination with chemotherapy for metastatic head and neck cancer.Thus, cetuximab became the world’s first targeted therapy approved for the treatment of head and neck cancer.
Clinical data demonstrate that cetuximab effectively prolongs patient survival compared with standard therapy. In the EXTREME study, the addition of cetuximab to chemotherapy extended median overall survival by nearly three months compared with chemotherapy alone. Furthermore, in the CHANGE-2 study conducted in China, cetuximab combined with platinum-based chemotherapy improved median overall survival by 2.2 months and achieved an objective response rate (ORR) of 50% compared with chemotherapy alone. Based on the favorable results from the EXTREME and CHANGE-2 studies, Erbitux (cetuximab) was approved by China’s National Medical Products Administration (NMPA) in 2020 for first-line treatment of recurrent or metastatic squamous cell carcinoma of the head and neck, in combination with platinum-based or fluoropyrimidine chemotherapy.
Cetuximab has become a boon for patients with head and neck cancer, primarily because its target, EGFR, is frequently mutated in this disease.However, from another perspective, although EGFR-targeted drugs have a relatively high overall response rate, their efficacy is only superior to that of chemotherapy and cannot “cure” head and neck cancer.
Following EGFR, a new breakthrough in head and neck cancer has emerged with PD-1. Immunotherapy, led by PD-1 monoclonal antibodies, can potentially cover nearly all types of tumors, and head and neck cancer is naturally one of the indications under focus. Although the FDA has approved PD-1 inhibitors for the treatment of head and neck cancer, the overall response rate remains low.
In 2016, Keytruda and Opdivo were successively approved for the indication of head and neck cancer.First, in August 2016, Keytruda received accelerated approval from the FDA for patients with recurrent or metastatic head and neck squamous cell carcinoma (HNSCC) who had disease progression during or after platinum-containing chemotherapy, based on treatment data from HNSCC patients enrolled in KEYNOTE-012, a multicenter, non-randomized Phase 1b clinical trial.
In this study, the objective response rate (ORR) and complete response rate (CR) for Keytruda were not particularly impressive, standing at only 16% and 5%, respectively. However, among patients who achieved a response, 82% maintained their response for more than six months. Given the strong unmet need for new treatment options in head and neck cancer, the FDA opted to grant Keytruda accelerated approval.
Following the accelerated approval of Keytruda, Opdivo’s coverage quickly caught up. In November 2016, Opdivo was also approved for the same indication as Keytruda: recurrent or metastatic squamous cell carcinoma of the head and neck (SCCHN) with disease progression during or after platinum-based chemotherapy. However, Opdivo did not rely on the Fast Track designation; instead, its approval was based on robust results from a Phase III clinical trial (CheckMate-141).
CheckMate 141 randomized subjects in a 2:1 ratio to the Opdivo treatment group (n=240) and the investigator’s choice control group (n=121). In January 2016, the independent Data Monitoring Committee (DMC) for this clinical trial determined, after evaluating interim data, that the study had met its primary endpoint, leading to early termination of the trial. In this study, the risk of death was reduced by 30% in the Opdivo group, with a median overall survival of 7.5 months, significantly prolonging patient survival compared to 5.1 months in the control group.
Following their dual approval for second-line treatment, PD-1 monoclonal antibodies have further advanced into first-line therapy. In June 2019, the FDA approved Keytruda as a monotherapy for first-line treatment of PD-L1-positive metastatic or unresectable recurrent head and neck squamous cell carcinoma (HNSCC), or in combination with standard chemotherapy for first-line treatment of the same indication. In China, in December 2020, the National Medical Products Administration (NMPA) website updated the status of Keytruda as a monotherapy for PD-L1-positive metastatic or unresectable recurrent HNSCC to “Approval Completed – Pending Certificate Issuance,” marking the entry of immunotherapy into the first-line treatment regimen for head and neck cancer in China.
Additionally, if pembrolizumab (Keytruda) has been used as first-line therapy, PD-1 monoclonal antibodies will not be used as monotherapy in the second-line setting. For patients who are insensitive to PD-1 monoclonal antibodies, standard treatment regimens remain the only option for second-line therapy after first-line treatment failure.In other words, the advancement of PD-1 monoclonal antibodies to an earlier line of therapy once again leaves a gap in the second-line treatment landscape for HNSCC.
Although PD-1 monoclonal antibodies ultimately received regulatory approval for the treatment of head and neck cancer, their development process was far from smooth.
The UK’s National Institute for Health and Care Excellence (NICE) has issued guidance recommending against the use of Opdivo for the treatment of adult patients with recurrent or metastatic squamous cell carcinoma of the head and neck (SCCHN) whose disease has progressed during or after platinum-based chemotherapy. The key reason for this recommendation is that,In the CheckMate 141 study, there was no comparison of the efficacy difference between Opdivo and docetaxel, the optimal chemotherapy drug currently used for treating head and neck cancer.
Whether it is Keytruda or Opdivo, the ultimate fact demonstrated is thatPD-1 monoclonal antibodies are indeed effective in some patients with head and neck cancer, and those who are sensitive to the treatment can achieve very favorable outcomes. However, for patients who are not sensitive, PD-1 monoclonal antibodies have not demonstrated significant clinical superiority over chemotherapy.This has significantly undermined the breakthrough status of PD-1 monoclonal antibodies in the diagnosis and treatment of head and neck cancer.Overall, PD-1 monoclonal antibodies demonstrate suboptimal response rates in patients with head and neck cancer, with only a small subset of patients experiencing prolonged survival.
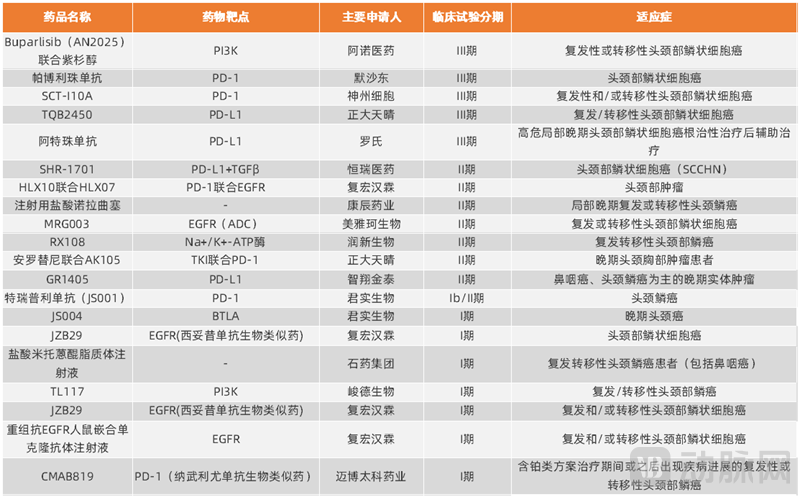
Head and Neck Cancer Clinical Trials Registered on the Drug Clinical Trial Registration and Information Publicity Platform
According to the Drug Clinical Trial Registration and Information Publicity Platform, products currently undergoing registrational clinical studies for head and neck cancer in China can be broadly categorized into three types.The first category comprises novel targets demonstrating clinical potential, primarily PI3K; the second category includes two core targets with established efficacy in head and neck cancer, namely EGFR and PD-(L)1; and the third category encompasses other targets still in early-stage development.
Among products in Phase III clinical trials, apart from four PD-(L)1 monoclonal antibodies, there is only one pan-PI3K inhibitor from Anol Therapeutics.Given the relatively extensive body of research on PD-(L)1, PI3K, as a novel therapeutic target in head and neck cancer, presents substantial market opportunities.
From a global perspective on the development of PI3K inhibitors, five such agents have been approved for marketing; however, their indications are primarily limited to hematologic malignancies and breast cancer. Currently, no PI3K inhibitor has been approved for head and neck cancer, and even the number of products actively pursuing this indication remains limited.
There are currently two PI3K inhibitors undergoing head and neck cancer-related research in China: Buparlisib from Anuo Medicine and TL117 from Junde Biopharma. This article will take Buparlisib, which has demonstrated faster clinical progress, as an example to explore the clinical value of PI3K inhibitors in head and neck cancer.
Buparlisib was initially developed by Novartis. In July 2018, Arno Therapeutics entered into an agreement with Novartis, securing exclusive global rights to develop, manufacture, and commercialize Buparlisib. In the Phase II clinical trial BERIL-1, previously conducted under Novartis’s leadership, Buparlisib in combination with paclitaxel demonstrated significant clinical value. According to data reported in publications related to this Phase II study, the objective response rate (ORR) in the experimental arm (Buparlisib plus paclitaxel) reached 39%, compared with only 14% in the control arm (placebo plus paclitaxel). Furthermore, the experimental arm showed a markedly longer median overall survival of 10.4 months, versus 6.5 months in the control arm. Owing to its outstanding performance in the Phase II clinical trial, Buparlisib was granted Fast Track designation by the U.S. Food and Drug Administration (FDA).
More encouragingly, in animal models, Buparlisib significantly inhibited tumor growth and exhibited a dose-response trend in tumor-bearing mice refractory to PD-1 inhibitors. This suggests that Buparlisib is not only effective in patients insensitive to PD-1 monoclonal antibodies but may also synergize with them, thereby providing therapeutic coverage for the entire head and neck cancer population.
In terms of Phase III clinical trials, Buparlisib received clinical trial approval from the U.S. FDA in December 2018 and from China’s NMPA in July 2020, respectively. Furthermore, the FDA has agreed that Arno Therapeutics may submit a New Drug Application (NDA) early if the objective response rate (ORR) meets predefined criteria at the interim analysis. This indicates that the development progress of Buparlisib for the indication of head and neck cancer is likely to be further accelerated.
On April 15, 2021, Ascentage Pharma announced that the first patient had been successfully dosed in Shanghai East Hospital in its Phase III clinical study evaluating buparlisib in combination with paclitaxel for the treatment of recurrent or metastatic head and neck squamous cell carcinoma (HNSCC). This study will enroll nearly 500 patients with HNSCC across more than 150 research centers in 15 major countries and regions throughout North America, Europe, and the Asia-Pacific region. Eligible patients include those who have experienced disease progression after prior treatment with PD-1/PD-L1 monotherapy, PD-1/PD-L1 inhibitors combined with platinum-based chemotherapy, or sequential therapy with PD-1/PD-L1 inhibitors and platinum-based chemotherapy (regardless of the order of administration).
This also signifies that the first large-scale Phase III clinical trial of PI3K inhibitors in head and neck cancer has officially commenced, bringing novel mechanism-based therapeutic regimens for this disease within close reach.
In addition to PI3K inhibitors, which warrant attention, other products poised to achieve rapid breakthroughs in head and neck cancer are almost exclusively focused on targets that have already been clinically validated.
First, regarding the EGFR target, Henlius has implemented a relatively focused strategy, encompassing its internally developed novel product HLX07 and JZB29, a biosimilar of cetuximab. The development progress of JZB29 is relatively slow compared to other ongoing programs, whereas HLX07 is being evaluated in combination with PD-1 inhibitors for the treatment of head and neck cancer.
In addition to the two products from Henlius, Meiyake Biotech, the holding company of Lepu Biopharma, also has an EGFR-targeted ADC monoclonal antibody currently in Phase II clinical trials, although limited information has been disclosed to date.
There are numerous PD-(L)1 products. Merck’s Keytruda, SinoCellTech’s SCT-I10A, Roche’s atezolizumab, and Chia Tai Tianqing’s TQB2450 have all entered Phase III clinical trials. In Phase II, Junshi Biosciences’ toripalimab, Hengrui Medicine’s PD-L1/TGF-β bispecific antibody SHR-1701, and Henlius’ HLX10 are also advancing their layouts targeting this pathway.
For the crowded PD-(L)1 monoclonal antibody market, head and neck cancer represents an indication where only Opdivo has recently entered the Chinese domestic market. Consequently, both new products awaiting approval and leading already-approved agents are still strategizing their entry into this therapeutic area. However, historical R&D trends indicate that the development of PD-1 monoclonal antibodies has repeatedly encountered setbacks, with PD-L1 monoclonal antibodies facing even greater challenges. In 2018, AstraZeneca’s PD-L1/CTLA-4 combination therapy failed in Phase III clinical trials. Similarly, in 2020, the Phase III clinical study of Pfizer/Merck KGaA’s PD-L1 monoclonal antibody, Avelumab, also failed to meet its primary endpoint of progression-free survival (PFS).
Therefore, these new head and neck cancer therapeutic products based on existing mechanisms face competition from both approved and clinical-stage products; however, PI3K inhibitors demonstrate significant potential in the indication of head and neck cancer.
Other novel mechanism-based products are few in number and relatively behind in their research stages. Excluding combination therapies and bispecific antibodies that leverage known mechanisms, only Runxin Biologics’ Na+/K+-ATPase inhibitor RX108 and Junshi Biosciences’ BTLA monoclonal antibody JS004 remain; significant breakthroughs are unlikely to emerge in the short term.
In summary, in the current field of head and neck cancer treatment, the traditional regimen of surgery combined with chemotherapy remains the mainstream clinical approach. While EGFR-targeted therapies and PD-(L)1 inhibitors are gradually being incorporated into treatment protocols, the former demonstrates suboptimal efficacy, and the latter benefits only a limited patient population. Consequently, there remains a significant unmet need in clinical practice.
Based on currently investigational drugs, clinical study results disclosed for PI3K inhibitors have demonstrated significant therapeutic potential. In particular, they may serve as an excellent complementary option for patients unresponsive to PD-(L)1 monoclonal antibodies, bringing a breakthrough to the treatment of head and neck cancer.