Return to Value-Based Healthcare: The Future of Medical Payment Models
Article selected from the official account: Jiong Shen Product View, author: Jiong Jiong Tong Xue, published with authorization from VCBeat.
The previous article primarily discussed how commercial health insurance manages health by addressing the likelihood of disease onset at its source, thereby reducing the number of patients who fall ill and those with severe conditions, in order to control medical costs. This middle installment focuses on the value and implementation pathway of Diagnosis-Related Groups (DRGs), explaining how reasonable pricing through diagnostic case groups helps payers control healthcare expenditures.
If commercial health insurance is a strategy for “managing patients,” then Diagnosis-Related Groups (DRGs) are primarily a strategy for “managing providers.” Currently, the majority of medical expenses incurred by patients are determined by individual physicians. Is there a more rational approach that both ensures therapeutic efficacy for patients and reduces healthcare insurance expenditures? The following section examines how DRGs address this challenge.
Based on real-world cases around us, the majority of patient expenses are incurred on hospital examinations, medication purchases, and surgical treatment fees, which also constitute the largest expenditure for health insurance. According to 2012 statistics from the U.S. Institute of Medicine (IOM), the annual costs in the United States stemming from unnecessary treatments due to misdiagnosis, along with waste caused by various ineffective treatments, totaled as high as $750 billion—a staggering figure.
However, from the perspective of a commercially rational actor rather than a public-interest-oriented one, medical institutions may not prioritize cost savings for patients. This is particularly true in the current broader economic climate, especially within private hospitals.In reality, the most effective way to increase revenue is to admit more patients and prescribe more medications and tests. Some unscrupulous medical institutions even exploit the pretext of unavoidable medical risks, neglecting changes in patients’ actual conditions and issuing rough diagnoses. They then prescribe medications based on subsequent test results. Given the inherent uncertainties in medical practice and individual variations among patients, it is difficult to definitively establish misdiagnosis even when it occurs.
Based on China's Civil Code and information from legal websites, I have learned that medical liability in China is currently categorized into two types: fault-based and no-fault, as follows:
1. No-Fault Misdiagnosis and Mistreatment
(1) The early symptoms of the disease are atypical, and its onset, progression, and evolution have not yet manifested;
(2) The etiology of the disease is unknown, and effective diagnostic and therapeutic measures are lacking;
(3) Difficulties in timely and definitive diagnosis of rare diseases and complex, refractory conditions;
(4) Limitations of technical expertise and equipment conditions;
(5) Individual patient differences; patients and their families concealing important medical history or failing to comply with medical advice regarding relevant auxiliary examinations.
2. Negligent Misdiagnosis and Mistreatment:
(1) Inadequate history taking, with neglect of relevant medical history;
(2) Inadequate physical examination, resulting in the omission of important positive signs;
(3) Neglecting necessary differential diagnoses;
(4) Failure to interpret relevant auxiliary examination results carefully and in a timely manner;
(5) Overconfidence, failing to heed the opinions of others or instructions from senior physicians; failure to request consultations for cases with unclear diagnoses or suboptimal therapeutic outcomes within the specified timeframe;
(6) Failure to engage in professional development, resulting in substandard technical proficiency and failure to recognize diseases that should and can be identified.
“Can Medical Expenses Resulting from Misdiagnosis Be Claimed for Compensation?” – Compiled by Hualv.com
If you examine this description closely, it is not difficult to find that there are few elements that can be absolutely quantified, and the granularity of qualitative content is relatively broad. Therefore, it is challenging to define the boundaries of medical liability. Whether a doctor’s performance is constrained by the current level of medical practice or whether they knowingly commit misconduct for personal gain at the expense of patients often comes down to luck. One can only hope to encounter physicians who possess both professional ethics and clinical expertise each time. Of course, the majority of doctors in the market are honorable; I am not disparaging the medical profession, but rather acknowledging the possibility, however rare, that a small number of individuals may tarnish the reputation of the healthcare industry.
Therefore, in response to the aforementioned issues, the Chinese government has spared no effort in recent years to promote Diagnosis-Related Groups (DRG)-based payment. The aim is to standardize treatment protocols and reasonably estimate costs, thereby curbing these irrational practices. Compared with the traditional fee-for-service model, DRG-based payment offers significant advantages by mitigating a range of problems such as excessive testing, overtreatment, and overprescription. However, its applicability is somewhat limited, which constitutes a drawback. Nevertheless, as data becomes increasingly abundant and policy standards are progressively refined, the system is expected to improve continuously. By prioritizing key challenges and addressing the major component of hospitalization expenses, substantial progress has already been achieved.

In summary, the core value of DRGs lies in shifting the incentive structure for healthcare services: from rewarding volume-based fee-for-service to allowing providers to retain savings from compliant care, thereby curbing excessive medical treatment and establishing reasonable expenditure controls.
First and foremost, DRGs are essentially a healthcare quality management tool, primarily applied to the performance evaluation of short-term inpatient medical services and the control and management of health insurance payment quotas. The scientific basis of DRG-based payment lies in its use of optimal clinical pathways for case-mix groups as evidence-based foundations, while continuously undergoing iterative upgrades through comprehensive big data research methodologies. It is important to note that various types of health insurance consumption data from China’s 1.4 billion insured population, along with hospital medical record data, are uploaded to national databases. With access to these data, it becomes possible to broadly estimate the approximate costs associated with each case-mix group.
DRG-based payment generally follows the following design:

1. Base Rate
“The base rate” corresponds to the cost required per unit of medical service, which is consistent across all DRG case groups. This value can be calculated using historical data, particularly in regions where DRG-based payment is being piloted for the first time.
For example, when Wuhan piloted Diagnosis-Related Groups (DRGs) payment under the Basic Medical Insurance for Urban Employees (hereinafter referred to as “Employee Medical Insurance”), it used the average cost per hospitalization case from the year prior to the reform across all Employee Medical Insurance inpatient cases as the base rate.
2. Weight
“Weight” reflects the average treatment cost of cases in different DRG groups, which is generally determined by the complexity of treating the case group. For some cost data that are difficult to determine, clinical experts will be invited to discuss and combine past experience to make a decision.
For example: If the weight of one DRG is 2.0 and another is 1.0, it can be simply understood that the cost of the former is twice that of the latter.
3. Adjustment Factors
“Adjustment factors” typically emerge when DRG-based payment systems are widely implemented across different years, regions, and hospital tiers, although other factors may also contribute. In theory, DRGs adhere to the principle of “same price for the same disease.” However, significant variations exist in consumption levels across different regions and in treatment costs among hospitals of different tiers. To facilitate more effective implementation, an adjustment factor is introduced to enable differential reimbursement rates.

For example, due to regional differences between Tibet and Shanghai, as well as variations in local hospital classifications, tertiary Grade A hospitals in Shanghai receive higher reimbursement for treating similar cases compared to secondary Grade A hospitals in Tibet.
Its overarching guiding principle is “prospective pricing and bundled payment.” Reasonable prices are set based on historical data, with a fixed reimbursement amount assigned to each condition. This approach incentivizes hospitals and physicians to adhere to optimal clinical pathways and use medications rationally under the premise of proven efficacy, operating under the rule of “bearing excess costs internally and retaining surpluses.” The goal is to achieve effective patient outcomes at lower costs, rather than generating revenue through overprescribing. This creates stronger incentives for physicians to adopt cost-effective products with favorable therapeutic effects. Meanwhile, the medical insurance system can leverage Diagnosis-Related Groups (DRGs) to evaluate healthcare service performance using six indicators across three dimensions, thereby providing performance-based bonus rewards to hospitals and physicians for exceeding benchmarks.
① Healthcare Service Capacity (Number of DRG Groups, Case Mix Index [CMI])
② Healthcare Service Efficiency (Time Consumption Index, Cost Consumption Index)
③ Medical Service Safety (Mortality Rate in Medium-Low Risk Groups, Mortality Rate in High-Risk Groups)
This effectively encourages physicians to enhance their clinical competencies, pursue advanced training in medical techniques, and increase their enthusiasm for adopting more cost-effective treatment modalities in patient care!
Of course, some may argue that this could lead to another extreme: “undertreatment,” where physicians, in an effort to cut costs, opt for cheaper medications and simpler surgical procedures, thereby failing to implement necessary treatment plans. To address this issue, DRGs also define their scope of application, prioritizing mature case groups that can be readily standardized and regulated. For other cases, implementation can proceed gradually as data collection becomes more comprehensive.
The overall grouping methodology of Diagnosis-Related Groups (DRGs) is a management system that categorizes cases with similar clinical processes and comparable cost consumption into the same DRG based on individual patient characteristics, such as age, gender, length of stay, clinical diagnoses, conditions, procedures, disease severity, comorbidities and complications, and outcomes. Payment is then made according to pharmaceutical and medical service fee standards established for each group. This system is more suitable for covering inpatient medical expenses for short-term critical, emergency, and severe cases, primarily targeting inpatient cases with a length of stay of less than 60 days.
Outpatient cases, rehabilitation cases, cases requiring long-term hospitalization, and cases with identical diagnoses and treatment regimens but significant variations in resource consumption and/or treatment outcomes are also unsuitable for inclusion. For instance, certain psychiatric disorders with uncertain therapeutic efficacy are excluded from this grouping. Only enrolled medical records are subject to DRG-based payment. Therefore, it can be simply understood that diseases amenable to standardized management and assembly-line processing, where individual differences can be disregarded, will be incorporated into the DRG system in the future. In essence, this represents a further upgrade of industrialization, which may even be replaced by AI in the future.
Furthermore, the CHS-DRG system currently in use adopts the National Healthcare Security Administration (NHSA) version of ICD-10 codes, which comprise 2,048 categories, 10,172 subcategories, and 33,392 items for disease diagnoses. The NHSA version of ICD-9-CM3 codes includes 890 subcategories, 3,666 detailed items, and 13,002 entries for surgical procedures and operations. Core Diagnosis-Related Groups (ADRGs) are established based on the grouping principles of “consistency in clinical processes” and “similarity in resource consumption.”

It is structured hierarchically from broad to specific categories, first stratified by primary disease diagnosis, then by surgical procedures and interventions, and further by individualized characteristics, thereby establishing a three-tier grouping system:
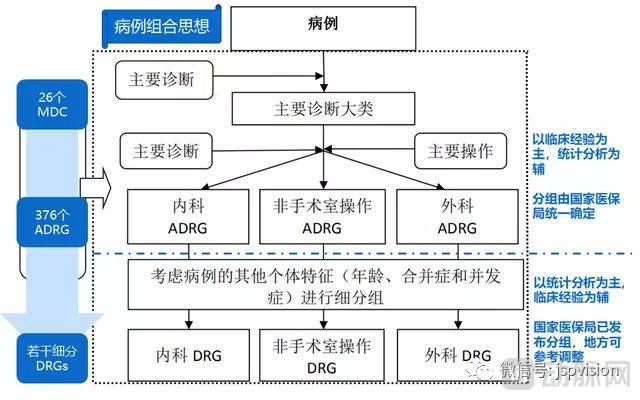
Level 1 (coarsest granularity): Cases are assigned to the corresponding Major Diagnostic Categories (MDC) based on the principal diagnosis listed on the patient’s medical record face sheet, in accordance with the International Classification of Diseases, Tenth Revision (ICD-10). MDCs are primarily categorized by anatomical and physiological systems, with the CHS-DRG system initially divided into 26 MDCs.
Level 2 (medium granularity): Within each Major Diagnostic Category (MDC), cases are further subdivided into Adjacent Diagnosis Related Groups (ADRGs) based on surgical procedures and treatment modalities. An ADRG is a cluster of cases with similar clinical processes, including disease diagnoses and primary procedures. Depending on the presence or absence of surgical interventions, ADRGs are classified into three major categories—Medical ADRGs, Surgical ADRGs, and Non-Operating Room Procedure ADRGs—comprising a total of 376 groups.
Level 3 (fine granularity): Taking into account other individual patient characteristics, comorbidities, and complications, the corresponding Adjacent Diagnosis Related Groups (ADRGs) are further subdivided into several Diagnosis Related Groups (DRGs). To achieve the goal of “equal payment for the same condition,” another metric—the Coefficient of Variation (CV)—is introduced to assess the degree of variation among cases. The overall grouping logic is illustrated in the figure below:
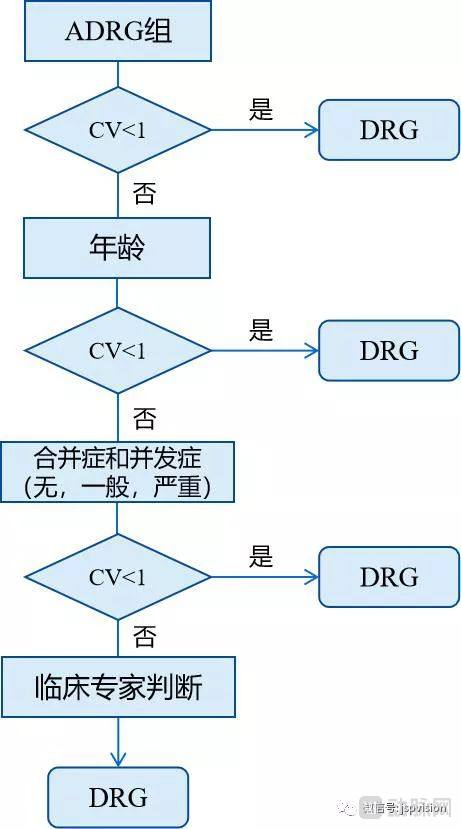
Subclassification is performed using the statistical classification node method:
① First, examine whether the coefficient of variation (CV) of hospitalization costs (or length of stay) is less than 1. If it is less than 1, no further subdivision is performed, as high consistency in resource consumption within the group is assumed; thus, the ADRG group can serve as a DRG subgroup.
② If the value is greater than or equal to 1, proceed to the next step to evaluate factors such as age, comorbidities, and complications. If the CV at this level is also greater than or equal to 1, continue to the next decision node;
③ At this stage, due to the significant variability, a clinical expert panel will be convened for comprehensive assessment until the coefficient of variation for hospitalization costs (or length of stay) falls below 1.
Thus, we can appreciate the rigor of this DRG grouping! The core objective is to clarify resource utilization for each disease and ensure price transparency. Consider this example: Zhang San, a 32-year-old male patient, was diagnosed with femoral shaft fracture at a Grade A tertiary hospital in Wuhan and underwent open reduction and internal fixation with a plate for femoral fracture, incurring costs of RMB 20,000. In contrast, Wang Wu, another 32-year-old male patient with the same diagnosis, underwent the same procedure at a Grade A tertiary hospital in Chengdu but incurred costs of RMB 80,000. Both cases fall under the same DRG group, IF15, with a benchmark price range of RMB 30,000–40,000. This indicates that Wang Wu’s expenditure of RMB 80,000 is unreasonable.
The overall design philosophy of DRG-based payment is inherently scientific and rigorous. Moreover, this mechanism offers the added benefit of transparency, which constitutes a tremendous boon for patients. At the very least, it enables patients to estimate the approximate cost of their treatment before care is delivered, rather than being subject to whatever amount the hospital dictates after treatment is completed. This approach returns a portion of decision-making power to patients. It is well established that any industry experiences significant advancement once “information asymmetry” is eliminated—a trend already validated in sectors such as e-commerce (Taobao), travel and hospitality (Ctrip), and real estate brokerage (Beike).
Furthermore, the implementation of DRGs will also impact another group of industry players: pharmaceutical companies. Previously, drugs with advantages in national medical insurance coverage enjoyed significant benefits. The traditional logic was that “inclusion in the national medical insurance list provided strong government endorsement, which increased physicians’ willingness to prescribe and improved patient acceptance, naturally driving rapid sales growth.” However, even if a drug is included in the medical insurance catalog, this no longer guarantees strong sales. Market performance will revert to the drug’s intrinsic “product competitiveness,” meaning physicians will prioritize prescribing cost-effective medications with proven efficacy, aligning with the prescribing guidelines under the DRG system.
Similarly, adjuvant drugs and traditional Chinese medicine (TCM) injections are likely to face immediate impact, as their efficacy remains unclear while their prices are not inexpensive. I have had such personal experiences during medical consultations: doctors would prescribe a genuinely indicated Western medication, only to supplement it with a large number of proprietary Chinese medicines, resulting in exorbitantly high pharmaceutical costs. Therefore, I subjectively believe that these two categories of drugs will inevitably be prioritized for phase-out in the future. This shift actually serves to positively recalibrate the pharmaceutical industry, urging certain pharmaceutical companies to return to the core essence of drug development. Instead of engaging daily in marketing tactics, courting physicians, and misleading patients, they should focus on enhancing their R&D capabilities, improving manufacturing processes and therapeutic efficacy, and developing more cost-effective, high-quality medications.
Therefore, when DRGs are integrated with commercial health insurance, the cost rates for each disease category become predictable and controllable. Meanwhile, standardized treatment protocols provide an evidence-based framework that ensures therapeutic efficacy for patients. This enhances the certainty of deliverables for commercial insurance, thereby facilitating the implementation and market launch of commercial health insurance products.
The emergence of DRGs primarily addresses the second-tier need of patient value discussed in my previous article—namely, the demand for “precise diagnosis.” It compels all stakeholders in the healthcare industry to return to their original mission and the essence of value-based healthcare, making information more transparent and shifting from profit-driven to user-value-driven models, thereby eliminating information asymmetry and imbalanced benefit distribution. If the first article focused on “managing patients,” and the middle one on “managing physicians,” then the final installment will address “managing pharmaceuticals,” discussing PBM (Pharmacy Benefit Management). Stay tuned for more.
