Racing Against Death Beyond Seconds: The Public Health–Clinical Relay in Sudden Cardiac Arrest
Author: Chen Yang
During the Euro Cup group stage match on June 13, Danish player Christian Eriksen suddenly collapsed due to cardiac arrest. Within 37 seconds, medical personnel rushed onto the field with an automated external defibrillator (AED) to administer emergency care, successfully saving Eriksen’s life. The entire rescue process was broadcast live to a global audience, raising awareness of the “golden four minutes” for sudden cardiac arrest resuscitation. On November 27, 2019, a Taiwanese actor suddenly suffered cardiac arrest and collapsed while running during a TV show recording. No immediate defibrillation or cardiopulmonary resuscitation (CPR) was administered at the scene, and despite more than two hours of emergency treatment at the hospital, he ultimately died from sudden cardiac death. Both incidents attracted widespread public attention at the time, bringing terms such as “sudden cardiac death,” “AED,” and “CPR” into the public spotlight. The vastly different outcomes of these two high-profile cases highlight that efforts to prevent and manage sudden cardiac death must go beyond merely emphasizing the “golden four minutes.” According to estimates in the Report on Cardiovascular Diseases in China, nearly 600,000 people die from sudden cardiac death annually in China, equivalent to one person collapsing every minute due to cardiac arrest, yet the survival rate remains as low as 1%. Much more needs to be done to protect the large population at high risk of sudden cardiac death.
I. Sudden Cardiac Death and Survival Rates
Sudden cardiac death accounts for 5%–15% of total mortality in industrialized nations; however, the exact incidence remains relatively unclear in both China and Western countries (the United States and Europe). In the United States, sudden cardiac death constitutes 5.6% of annual deaths. In 1999, an estimated 450,000 cases of sudden cardiac death occurred in the U.S., with the incidence of cardiac arrest estimated at over 180,000–450,000 cases. In North America and Europe, the estimated incidence in the general population is 50–100 per 100,000 individuals. Among these cases, resuscitation was attempted in two-thirds of cardiac arrest patients, with survival outcomes varying significantly: the out-of-hospital survival rate is 1%–6%; among out-of-hospital cardiac arrest patients who survive to hospital discharge, those receiving emergency treatment have a survival rate of 5%–10%; and when the underlying arrhythmia is ventricular fibrillation, the survival rate rises to 15%.
The "Report on Cardiovascular Diseases in China," released by the National Center for Cardiovascular Diseases, indicates that an estimated 544,000 people in China die from sudden cardiac death (SCD) each year. A related study conducted by Fuwai Hospital, Chinese Academy of Medical Sciences, followed more than 670,000 individuals in four cities across eastern, central, and western regions of China from 2005 to 2006. During the one-year follow-up period, 284 cases of SCD were recorded, leading to an estimated incidence rate of 41.8 per 100,000 population in China. The incidence rate was 44.6 per 100,000 among males and 39 per 100,000 among females.
The terms “sudden death” or “sudden cardiac death” frequently used in media reports are broad descriptions that encompass both sudden cardiac arrest (SCA) and sudden cardiac death (SCD). Both conditions refer to the abrupt cessation of the heart’s mechanical activity, accompanied by hemodynamic collapse, resulting in unresponsiveness, absence of normal breathing, and lack of circulatory signs; if not rapidly corrected, this state progresses to death. These events are typically caused by sustained ventricular tachycardia (VT) or ventricular fibrillation (VF) (Figure 1). Most patients experiencing sudden cardiac arrest lose consciousness within seconds to minutes due to insufficient cerebral blood flow.

Figure 1. Normal electrocardiogram on the left, ventricular fibrillation electrocardiogram on the right
As shown in the figure above, the regular cardiac electrical rhythm of the heart on the left ensures rhythmic contraction of the myocardium and normal pulsatile blood pumping. When ventricular fibrillation occurs, as seen on the right, chaotic electrical activity in the myocardium leads to quivering of the ventricular muscle, rendering the cardiac chambers unable to contract effectively (resulting in sudden cessation of the heart’s mechanical activity) and pump blood. This causes an immediate halt in systemic blood flow, cerebral hypoperfusion, loss of consciousness, and sudden collapse.
Common emergency interventions include cardiopulmonary resuscitation (CPR) and/or defibrillation or cardioversion, as well as cardiac pacing. If circulation is restored through intervention or spontaneous reversal, the event is termed cardiac arrest (or aborted sudden cardiac death); if the patient dies, it is classified as sudden cardiac death. It is difficult to distinguish out-of-hospital cardiac arrest from sudden cardiac death, as only two-thirds of sudden deaths are witnessed, and the initial cardiac rhythm (e.g., whether ventricular fibrillation was present) remains unknown in many cases at onset.
"Warning" symptoms often precede cardiac arrest, with onset ranging from one hour to one month before the event: 51% of patients experienced warning symptoms within the four weeks prior to cardiac arrest, while 80% and 34% reported symptoms at least one hour and 24 hours before occurrence, respectively. Among these, chest pain (46%) and dyspnea (18%) were the most common symptoms; in women, dyspnea was more prevalent than chest pain (31% vs. 24%). However, since most symptoms are non-specific and do not necessarily occur before every episode, and given that no causal or temporal relationship between these symptoms and sudden death has been established, their predictive value for prevention remains limited. Forty-nine percent of sudden cardiac deaths occurred during daily activities, 23% during sleep, and 23% were associated with physical exertion.
Despite advances in emergency care in recent years, outcomes for patients with cardiac arrest remain poor. Only one-third of out-of-hospital cardiac arrest (OHCA) patients achieve successful resuscitation, and merely about 10% of all patients are ultimately discharged from the hospital, many of whom suffer from neurological impairment. Numerous factors influence outcomes, including delays in bystander cardiopulmonary resuscitation (CPR), delays in defibrillation, advanced age, and a declining proportion of patients presenting with ventricular fibrillation (VF). Among these,Time interval from onset to effective resuscitation (i.e., establishment of an effective pulse)It may be the most critical.
1Extrinsic Factors: Time Interval from Onset to Effective Resuscitation
1) Accessibility of the Emergency Medical Services System
Even in foreign countries with relatively mature emergency medical systems, where emergency resuscitation training has become more established, the proportion of patients receiving bystander cardiopulmonary resuscitation (CPR) has increased, and the interval from onset to defibrillation has shortened, the response times for basic life support (BLS) and advanced life support (ALS) services have still increased due to population growth and urbanization. Foreign studies have shown significant regional variations in the incidence and outcomes of cardiac arrest, emphasizing the critical role of local emergency medical systems in determining cardiac arrest outcomes.
2) Duration of Ventricular Fibrillation
Survival outcomes in patients with cardiac arrest depend on the prompt administration of effective cardiopulmonary resuscitation (CPR). Electrical defibrillation is the only therapeutic intervention capable of restoring organized electrical activity and myocardial contraction. Prolonged duration of ventricular fibrillation (VF) leads to two major adverse consequences: ① a reduced likelihood of terminating the arrhythmia; and ② the onset of irreversible damage to the central nervous system and other organs if VF persists for more than 4 minutes.“The Golden 4 Minutes”” origin. The longer the duration of cardiac arrest, the lower the likelihood of successful resuscitation or survival rate. Studies have shown thatIn the absence of CPR, each 1-minute delay in defibrillation reduces the survival rate for ventricular fibrillation (VF)-induced cardiac arrest by approximately 10%; if CPR is not initiated within 12 minutes, the survival rate drops to only 2%–5%.
2Endogenous Factors: Etiology
There is a correlation between the mechanism of cardiac arrest and the outcomes of initial resuscitation; patients with cardiac arrest caused by ventricular tachyarrhythmias often have higher survival rates.
1) Ventricular Tachyarrhythmias: Favorable Outcomes
The most common cause of sudden cardiac death is ventricular fibrillation. When the initial rhythm is a sustained ventricular tachyarrhythmia (such as ventricular fibrillation or ventricular tachycardia), patient outcomes are relatively favorable.
Ventricular Fibrillation (VF):25%–40% of patients with cardiac arrest caused by ventricular fibrillation (VF) survive. Among cardiac arrest patients who received treatment abroad, 38% had bystander-witnessed VF. Compared with patients experiencing cardiac arrest due to other rhythms, those with bystander-witnessed VF have a significantly higher likelihood of survival to hospital discharge (34% vs. 6%). Acute myocardial infarction or myocardial ischemia is the primary underlying cause of VF, and approximately 47%–51% of survivors have acute myocardial infarction.
Ventricular Tachycardia (VT):The survival rate for patients with hemodynamically unstable ventricular tachycardia (VT) is approximately 65%–70%. The prognosis for patients with monomorphic VT may be more favorable, as this type of arrhythmia is more regular and may allow for some degree of systemic perfusion. Furthermore, patients with VT have a lower incidence of prior myocardial infarction compared to those with ventricular fibrillation, and they generally exhibit better cardiac function (often with a higher ejection fraction).
2) Asystole: Poor prognosis
When the initially observed cardiac rhythm is asystole (even if ventricular tachycardia [VT] or ventricular fibrillation [VF] preceded the asystole) or a very slow idioventricular rhythm resulting in bradycardia, the likelihood of successful resuscitation is low. Only 10% of out-of-hospital cardiac arrest patients with initial asystole survive to hospital admission, and fewer than 5% survive to discharge with favorable neurological outcomes. The poor prognosis in these patients may be attributed to the prolonged duration of cardiac arrest (typically exceeding 4 minutes), leading to severe and irreversible myocardial injury.
3) Pulseless Electrical Activity: Poor Prognosis
Pulseless Electrical Activity (PEA), also known as electromechanical dissociation, is associated with poorer outcomes in patients experiencing cardiac arrest. Among those who were resuscitated and survived to hospital admission, 23% survived, while only 11% survived to discharge.
4) Non-cardiac cardiac arrest: Poor outcomes
One-third of cardiac arrests are non-cardiac in origin, with trauma, non-traumatic hemorrhage, poisoning, near-drowning, and pulmonary embolism being the most common causes. Forty percent of patients achieve successful resuscitation and are hospitalized; only 11% are discharged, and 6% survive with intact neurological function.
II. “Catching Up” to Address Extrinsic Factors—The Race Against Time Between Public Health and Sudden Cardiac Death
Based on the above analysis, the key to improving the survival rate of patients with sudden cardiac death lies in the early implementation of effective resuscitation. Performing cardiopulmonary resuscitation (CPR) and defibrillation within the "golden 4 minutes"—the optimal window for resuscitation—significantly increases the likelihood of patient survival, whereas very few patients can be successfully resuscitated after 10 minutes. Since 87.7% of sudden cardiac deaths in China occur outside of hospitals, immediate CPR by bystanders is the most timely intervention, buying crucial time for medical personnel to arrive on scene. Bystander first aid is critical: compared to treatment solely by professional emergency responders, early defibrillation using an automated external defibrillator (AED) by lay first responders can double patient survival rates. If defibrillation is administered within three minutes of collapse, 74% of witnessed ventricular fibrillation cases result in survival. For every minute that elapses between cardiac arrest and defibrillation, survival rates decrease by approximately 5%–10%. While bystander CPR rates in Europe can reach 60%, public awareness and practice of CPR remain low in China; it is rare for on-site witnesses to perform CPR, and the quality of resuscitation is difficult to guarantee.
Basic life support, including CPR and AED defibrillation. The key to survival after cardiac arrest is early recognition and treatment; patient survival rates depend primarily on the immediate initiation of high-quality CPR and early defibrillation.
Key points emphasized in current resuscitation guidelines include: ① immediate recognition of cardiac arrest by observing unresponsiveness or absence of normal breathing/gasping; ② prompt initiation of high-quality CPR (adequate depth and rate of compressions), with continuous attention to the quality of chest compressions and ventilation frequency; ③ minimization of interruptions in CPR; ④ for healthcare providers, pulse check should not exceed 10 seconds; ⑤ for untrained lay rescuers, high-quality compression-only CPR (CO-CPR) is encouraged; ⑥ use of an automated external defibrillator (AED) as soon as available; and ⑦ prompt activation of emergency medical services.
1Time Window
The resuscitation time window is primarily divided into three stages: immediate defibrillation is required within the first 4–5 minutes; chest compressions combined with defibrillation are indicated between 4 and 10 minutes; and few patients survive after 10 minutes. This is mainly related to the pathophysiological progression of cardiac arrest:
① Electrical Phase:Within 4–5 minutes of cardiac arrest caused by ventricular fibrillation.Immediate defibrillation is required to maximize survival rates in these patients. Performing high-quality chest compressions while preparing the defibrillator also improves survival outcomes.
② Hemodynamic Stage (Circulatory Stage):Minutes 4–10 after cardiac arrest,During this period, the patient may still be in ventricular fibrillation, and early defibrillation remains critical for survival in patients identified with ventricular fibrillation. Once cardiac arrest is confirmed, high-quality chest compressions should be initiated immediately and continued until defibrillation is delivered. In practice, the defibrillator should be charged during effective chest compressions; compressions should only be paused to confirm the rhythm and deliver the shock, and CPR should be resumed immediately after the shock is administered. Patients in the hemodynamic phase benefit from high-quality chest compressions that generate adequate cerebral and coronary perfusion, as well as from immediate defibrillation.
③ Metabolic Phase:Few patients survive to this stage 10 minutes after the disappearance of the pulse.. Treatment is primarily based on post-resuscitation measures, such as therapeutic hypothermia. Patients in this phase who do not rapidly restore a perfusing cardiac rhythm typically do not survive.
2Quality of Resuscitation
1) Identification
Rapid identification of cardiac arrest is the critical first step toward successful resuscitation. When a rescuer witnesses someone suddenly collapse or encounters an individual who appears unresponsive, they should ensure the area is safe before approaching the patient, then tap the person’s shoulder and shout loudly to confirm unresponsiveness. If unresponsiveness is confirmed, the rescuer shouldImmediately initiate high-quality CPR and early defibrillationand call the emergency center. It should be noted that even professionalsIt is difficult to determine whether a pulse is present or whether breathing is adequate; bystanders should not attempt to assess the pulse.Instead, assume that the patient has stopped breathing, and even when checking for a carotid pulse, do not exceed 10 seconds. The key principle is that CPR should not be delayed.
2) Compression
The most critical component of CPR is chest compressions., as coronary perfusion and return of spontaneous circulation (ROSC) are both associated with compressions. Key indicators:① Frequency: Maintain the rate of chest compressions at 100–120 per minute. An insufficient chest compression rate reduces the likelihood of return of spontaneous circulation (ROSC) and survival with intact neurological function after cardiac arrest;② Depth: The depth of each chest compression should be at least 5 cm but no more than 6 cm;③ Rebound: After each chest compression, allow the thorax to fully recoil. Recoil reduces intrathoracic pressure, thereby increasing cardiac preload and achieving higher coronary perfusion pressure;④ Continuation:The frequency and duration of any interruptions should be minimized.
Minimize interruptions as much as possible:Any interruption in chest compressions during CPR, regardless of duration, leads to a decline in coronary and cerebral perfusion pressure, thereby further worsening patient outcomes.
3) Ventilation
When non-professional bystanders provide aid,Chest Compression-Only CPR (CO-CPR) May Be Superior to Chest Compressions Plus Ventilation.Current guidelines advocate for the compressions-airway-breathing (C-A-B) approach in cardiac arrest, based on the rationale that alveoli are likely to contain sufficient levels of oxygen during the initial phase of cardiac arrest, and that the pulmonary vasculature and heart may hold enough oxygenated blood to meet the body’s significantly reduced oxygen demand. Initiating high-quality chest compressions is the first step in improving oxygen delivery to tissues; at this stage, chest compressions are more critical than ventilation.
However, in cardiac arrest patients with concomitant hypoxia, oxygen reserves may already be depleted, necessitating the implementation of high-quality CPR with ventilation. As pulselessness persists, appropriate ventilation becomes increasingly critical. Key indicators: ① If an advanced airway has not been established, deliver 2 ventilations after every 30 chest compressions; ② Each ventilation should last no longer than 1 second; ③ The tidal volume delivered should be only sufficient to observe visible chest rise (500–600 mL).
4) Defibrillation
Early defibrillation is critical to the survival rate of patients with ventricular fibrillation. For adults, it is recommended to use the maximum available energy level for defibrillation; do not stop chest compressions while the AED is charging, and resume chest compressions immediately after delivering a single shock with the AED.
High-incidence locations for cardiac arrest include public transportation facilities, shopping malls, and public sports venues, where bystanders can use automated external defibrillators (AEDs) available on-site to deliver defibrillation before emergency medical personnel arrive. This is“Public Access Defibrillation (PAD)”, greatly expanding the pool of potential rescuers capable of providing early defibrillation.
AED Deployment Directly Impacts Survival Rates for Sudden Cardiac Arrest
Public access defibrillation can effectively improve survival rates and neurological outcomes after cardiac arrest. Foreign studies have shown that the survival rate of patients who experienced cardiac arrest in public places with AEDs (23.4%) is significantly higher than those without AEDs (14.0%), and the proportion of survivors with normal neurological function is also higher (50% vs 14%). Japan widely deployed AEDs in public places nationwide between 2005 and 2013, increasing the percentage of witnessed VF arrests shocked by non-professionals using AEDs from 1.1% to 16.5%. With the increase in public-initiated defibrillation, the time from arrest to shock decreased from 3.7 minutes to 2.2 minutes, and the survival rate with good neurological function significantly doubled (from 18.2% to 38.5%).
Further Reduce the AED Accessibility Radius
The golden window for rescuing victims of sudden cardiac death is to initiate cardiopulmonary resuscitation (CPR) and defibrillation within four minutes. Based on calculations combining the running distance of an average person with the current coverage rate of automated external defibrillators (AEDs), AED availability in China remains in a stage of “present but inaccessible.” In contrast, mobile AEDs offer six times the coverage efficiency of fixed AEDs. Taking the recent UEFA European Championship as an example, the speed and efficiency of team doctors entering the field with AEDs set a benchmark for mobile AED deployment: at 0 seconds, the athlete collapsed without contact; at 5 seconds, the referee summoned medical personnel; at 13 seconds, the team doctor arrived on site; at 37 seconds, medical staff carrying emergency equipment, including an AED, rushed onto the field; at 52 seconds, the AED was activated; and at 1 minute and 36 seconds, CPR was initiated by medical personnel. Such rapid emergency response would be impossible if AEDs were placed only in fixed locations within the stadium. Mobile AED deployment involves unidirectional movement, covering an area four times larger than that of fixed AEDs (as unidirectional running distance is half the round-trip distance); meanwhile, it eliminates the time spent on locating and retrieving devices, ensuring clear responsibilities and well-defined roles among personnel. Studies show that the rescue coverage efficiency of mobile AEDs is approximately six times that of fixed AEDs, significantly expanding the potential scope of AED-mediated lifesaving interventions.
China’s AED Penetration Lags Behind, Catching Up Since 2020
Currently, there is a significant gap in the popularization of automated external defibrillators (AEDs) and related public education in China. The AED deployment rate in China is only 0.2 units per 100,000 people, whereas in the United States it reached 317 units per 100,000 people in 2017, with Japan at 394 units and the Netherlands at 695 units per 100,000 people. Correspondingly, the survival rate for out-of-hospital cardiac arrest in China is merely 1%, while that in the United States has approached 40%.
In recent years, with the frequent occurrence of sudden cardiac deaths among public figures, Automated External Defibrillators (AEDs) have gradually garnered public attention and recognition, prompting the government to accelerate their deployment in public spaces. In 2006, AEDs were officially introduced in China, with Beijing Capital International Airport becoming the first public venue in the country to install them, deploying 11 units in Terminal 2. The 2008 Beijing Olympics spurred a surge in AED adoption nationwide; however, momentum waned after the Games concluded. In 2019, the State Council issued the Healthy China Action (2019–2030), which explicitly set targets for the proportion of personnel trained in cardiopulmonary resuscitation (CPR) and called for improved standards for emergency medical equipment and facilities in public places. It mandated the provision of emergency medications, equipment, facilities, and AEDs in densely populated areas such as schools, government agencies, enterprises, public institutions, airports, railway stations, port passenger terminals, large shopping malls, and cinemas. Furthermore, the 15th Session of the Standing Committee of the 13th National People’s Congress reviewed and passed the Law of the People’s Republic of China on Basic Medical and Health Care and the Promotion of Health, which incorporated specific provisions requiring public places to be equipped with necessary emergency rescue devices and facilities in accordance with regulations. It is hoped that AEDs will be rationally deployed in public spaces based on comprehensive considerations—including scale, population dynamics, and willingness to participate—thereby gradually forming an integrated network.
2020 marked a pivotal milestone in the popularization of automated external defibrillators (AEDs) in China. Multiple cities across the country began to install or increase the number of AEDs in public spaces, particularly in transportation hubs, signifying a significant step forward in AED adoption nationwide. Many Chinese cities are promoting AED deployment and have formulated AED configuration plans to accelerate implementation. Shenzhen was an early adopter and currently boasts the highest AED coverage rate in China. In 2017, Shenzhen launched its plan to equip public places with AEDs. By March 2021, more than 5,500 AEDs had been installed in public areas, accompanied by an “AED Navigation” system. The city aims to reach the internationally recommended standard of 100 units per 100,000 people within the next 5–10 years.In December 2020, three cities simultaneously achieved large-scale AED deployment: Dongguan Metro Line 2 achieved full station coverage; Guangzhou Metro completed the installation and operational use of the first batch of 59 pilot AEDs; and Kunming deployed 1,100 AEDs in public venues such as metro stations, large shopping malls and supermarkets, tourist attractions, and airports. Since 2016, AEDs have already begun to play a role in public spaces in several Chinese cities. On October 27, 2020, AEDs were introduced into Beijing’s metro system for the first time. By the end of December 2020, 58 AEDs had been installed on Beijing Metro Lines 1, 2, and 13.Meanwhile, various cities continue to outline future configuration plans: Nanjing has planned to deploy 1,000 AEDs by 2021, achieving full coverage in metro stations; Beijing announced that key public venues (specifically rail transit stations) would achieve full AED coverage by the end of 2022; Hangzhou plans to reach a total of 4,200 AEDs in public spaces across the city by 2022; and Yunnan Province will deploy 4,800 AED devices throughout the province.
In October 2020, the Hangzhou Municipal Administrative Measures for Automated External Defibrillators in Public Places was adopted, coming into effect on January 1, 2021. This made Hangzhou the first city in China to regulate the configuration and use of automated external defibrillators (AEDs) in public places through local legislation. Meanwhile, a plan was implemented to install an additional 3,596 AEDs across the city within three years, ensuring a deployment rate of 42 units per 100,000 people.
With the widespread adoption of automated external defibrillators (AEDs), there have been numerous news reports in the first half of this year highlighting successful AED rescues for sudden cardiac arrest cases on subways, marking a promising start for public defibrillation efforts in China.
Another reason for the initial difficulties in promoting AEDs in China was public apprehension. When individuals suffered sudden cardiac arrest in public spaces, onlookers were often reluctant to intervene due to fears of legal liability. Influenced by several widely circulated adverse legal precedents, many people worried about potential disputes with patients or their families after providing aid. This concern about civil liability for life-saving efforts was not limited to individuals; many managers of public venues shared similar anxieties. Although Article 184 of the Civil Code of the People’s Republic of China stipulates that individuals who voluntarily provide emergency assistance shall not bear civil liability for any harm caused to the recipient, changing public fear of providing aid will take considerable time. Nevertheless, with the implementation of relevant policies and regulations, along with increased publicity of successful resuscitation cases in public settings, the burden on “bystanders” closest to victims of cardiac arrest is gradually diminishing.
In addition to the density of AED deployment and issues regarding bystander legal liability, the low prevalence of first aid training in China is also a major reason for the low resuscitation rate for cardiac arrest. Many witnesses at the scene of sudden cardiac death lack the skills or confidence to perform CPR; they can only call the emergency number 120, thereby missing the critical “golden four minutes” for resuscitation. The coverage of first aid training in developed countries is very high: 40% of the total population in France, 80% in Germany, and 30% in the United States have received such training, whereas the rate in China is merely 1%.Currently, institutional arrangements have been made to popularize first aid knowledge. The Healthy China Action (2019–2030) encourages and supports social organizations such as the Red Cross Society and medical institutions like emergency centers to conduct mass emergency rescue training, popularize national emergency rescue knowledge, and enable the public to master essential self-rescue and mutual-aid skills such as cardiopulmonary resuscitation (CPR). The National Health Commission is designated to take the lead, with the Ministry of Education, the Ministry of Finance, and the Head Office of the Red Cross Society of China assuming responsibilities according to their respective divisions of labor. The plan explicitly proposes health promotion actions for primary and secondary schools, incorporating student health knowledge and first aid knowledge—particularly CPR—into examination curricula. Furthermore, proficiency in health and first aid knowledge, along with physical fitness test results, will serve as important indicators for student awards, graduation assessments, and advancement to higher levels of education. However, effective implementation still requires multi-sectoral collaboration involving guidance from health administrative departments, training by educational authorities, and cooperation from public welfare organizations. Only through seamless coordination across multiple links can the current shortcomings in public services be addressed, ultimately leading to a significant improvement in survival rates from sudden cardiac death in China.
Currently, the rate of favorable neurological outcomes following conventional cardiopulmonary resuscitation (CPR) for out-of-hospital cardiac arrest is only 5%–10%. Patients often lose the opportunity for a favorable neurological prognosis due to the lack of timely and efficient resuscitation measures. Although conventional CPR remains the widely promoted basic method for cardiopulmonary resuscitation due to its convenience and ease of use, its circulatory support effect is relatively weak. After cardiac arrest, the body enters a state of hemodynamic stagnation, with vital organs experiencing non-perfusion. Under high-quality chest compressions, conventional CPR actually results in a low-flow state (cardiac output can reach 30%–40% of pre-arrest levels, and coronary perfusion pressure reaches 20–25 mmHg), which can meet certain requirements for the return of spontaneous circulation. However, if a patient fails to sustain spontaneous circulation for more than 30 minutes after cardiac arrest, it is termedRefractory Cardiac Arrest, such patients have a lower probability of favorable neurological outcomes due to prolonged hypoperfusion of vital organs (e.g., brain and kidneys).
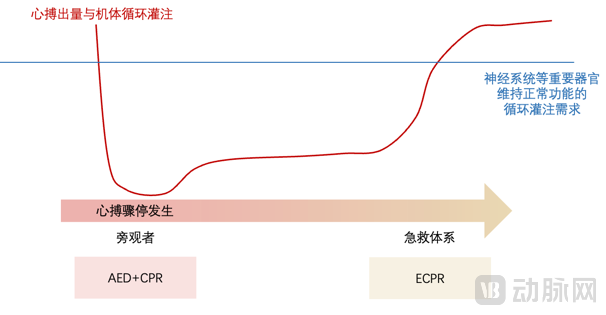
Figure 2. During conventional CPR, cardiac output is 30%–40% of normal; however, if return of spontaneous circulation cannot be sustained after more than 30 minutes of cardiac arrest, ECMO should be immediately initiated to provide emergency circulatory and oxygenation support, thereby maintaining perfusion to vital organs.
Extracorporeal Cardiopulmonary Resuscitation (ECPR) refers to a technique that involves the rapid initiation of extracorporeal membrane oxygenation (ECMO) to provide temporary circulatory and respiratory support for selected patients with reversible causes of cardiopulmonary arrest who have failed to achieve return of spontaneous circulation despite conventional cardiopulmonary resuscitation (CPR). As a novel resuscitation strategy introduced in recent years, ECPR can shorten the duration of low-flow state after cardiac arrest, achieving favorable neurological outcomes in 30%–40% of patients with refractory cardiac arrest. The 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation suggest that ECPR may be considered for specific cardiac arrest patients, provided that a rapid and specialized team is available. According to reports from the Extracorporeal Life Support Organization (ELSO), adult ECPR cases have increased rapidly over the past decade, reaching 1,197 cases in 2018 with an overall survival rate of 29.5%, whereas the overall survival rate for ECPR in China is 26%. Data from certain centers indicate that among ECPR patients, those in whom ECMO circulation was established within 60 minutes of CPR achieved a favorable neurological outcome rate of 50%, compared to 23.1% for those in whom ECMO was initiated after more than 60 minutes of CPR.
The success of ECPR depends on timely CPR, a robust ECMO team, and subsequent intensive care in the ICU. In China, the coordination between the current emergency medical system and critical care clinical practice still needs to be further strengthened:
System: Emergency Care Network Coordination and ECPR Response Zone Coverage
It is important to note that ECPR also has a distinct resuscitation time window: if return of spontaneous circulation (ROSC) is not achieved after more than 15 minutes of continuous CPR, ECMO should be immediately initiated for emergency circulatory and oxygenation support. To ensure timely application of ECMO within 15 minutes for patients experiencing out-of-hospital cardiac arrest (OHCA), reliance on the existing emergency medical services (EMS) system is essential. In the pre-hospital phase, when bystanders call 120 (the emergency number in China), they should simultaneously notify the regional hospital’s ECPR team to prepare in advance. Upon arrival at the scene, EMS personnel assess the patient and inform the ECPR team of the designated receiving hospital, prompting the ECPR team to depart immediately with the necessary equipment. During transport by 120 EMS, both the transportation radius and travel time to hospitals capable of providing ECPR must be carefully considered, as these factors are directly correlated with ECPR success rates. Upon hospital arrival, an established in-hospital ECPR green channel enables patients to promptly enter the ECPR clinical pathway. The resuscitation room dedicated to ECPR must be fully equipped with all required devices and supplies.
Personnel: ECPR Technology and ECMO Training
Given the critical importance of time in extracorporeal cardiopulmonary resuscitation (ECPR), transport distances should be minimized. Where distance permits, patients can be transferred to regional ECPR centers with comprehensive treatment capabilities for multidisciplinary collaborative care. To further reduce the transport radius, it is imperative to establish ECPR sub-centers to ensure coverage across different regions and guarantee timely treatment for patients with cardiac arrest. For the large-scale implementation of ECPR, ECMO training is essential, relying on technical guidance from experienced local regional ECPR centers to ensure the quality of resuscitation and proficiency in ECPR skills.
Equipment and On-Site ECPR: Mobile ECMO Shortens Circulatory Recovery Time
The traditional approach of performing resuscitation while transporting patients to the hospital inevitably leads to a decline in the quality of resuscitation during transit. Currently, some pre-hospital emergency systems in Europe and the United States directly carry ECMO equipment to the scene to implement ECPR, which shortens the duration of low-flow perfusion and increases the rate of return of spontaneous circulation (ROSC). However, due to limitations in China’s emergency medical system and resources, on-scene ECPR is still in its early stages of development. In recent years, with advancements in emergency care awareness, high-end ambulances in China have begun to be equipped with ECMO devices.
Due to the differences between the transport environment and the ICU environment, ECMO systems used for emergency transport have specific performance requirements—they must withstand vibrations and impacts during transit and be portable. Due to high technical barriers, domestic production has not yet been achieved; currently, all ECMO systems in China are imported, primarily dominated by foreign manufacturers such as Maquet, Medtronic, and LivaNova. Among these, owing to stringent performance requirements, only Maquet’s Cardiohelp is available for emergency transport. As a high-end product line, it is priced at nearly RMB 3 million and has not been widely deployed. Companies currently developing emergency ECMO systems in China include Suzhou Xinqing Medical, among others.
III. “Transcending” to Address Endogenous Factors—Taking a Proactive Step: The Critical Responsibility of Clinical Prevention
Sudden cardiac death (SCD) occurs abruptly and is difficult to predict, with the vast majority of cases taking place outside of hospitals. Although automated external defibrillators (AEDs) can effectively facilitate resuscitation, their use depends on bystander intervention. Statistics show that only 50% of cardiac arrests are witnessed; when no bystander is present to identify a cardiac arrest patient, effective rescue becomes impossible. Therefore, at the population level, relying on post-event treatment to save lives after SCD occurs is often too late. The key to reducing SCD mortality lies in the effectiveness of prevention and control measures for sudden cardiac death.
1Mechanism of Sudden Cardiac Death: Myocardial "Structural" Abnormality → "Electrical Short Circuit" → Cessation of "Pump Function"
Cardiac arrest frequently occurs in patients with underlying structural heart disease, most notably coronary artery disease (CAD), which accounts for 70% of cardiac arrest cases. Among patients with CAD, cardiac arrest can occur both during acute coronary syndrome (ACS) and in those with chronic stable CAD. Patients with chronic CAD typically have prior myocardial injury and myocardial scarring that may predispose them to cardiac arrest.
How, then, does myocardial injury affect electrical conduction, thereby leading to cardiac arrest? Among the types of arrhythmias that can cause sudden cardiac death, 25%–35% are attributable to ventricular fibrillation and pulseless ventricular tachycardia, and 25% are caused by pulseless electrical activity (PEA). The occurrence of ventricular fibrillation and ventricular tachycardia is closely associated with electrical conduction abnormalities resulting from myocardial ischemia or post-myocardial infarction scarring:
Mechanisms of Ventricular Fibrillation (VF)—Myocardial Heterogeneity: Rotating spiral waves are the most likely mechanism, almost always occurring in the context of underlying diffuse myocardial disease (Figure 3), which leads to heterogeneity of depolarization and dispersion of repolarization. This inconsistency in electrophysiological properties is a prerequisite for reentry. Multiple local micro-reentrant circuits result in ventricular fibrillation, during which there is no organized electrical activity. Differences in conduction and repolarization parameters (myocardial heterogeneity) cause impulse fragmentation during propagation through the myocardium, thereby forming multiple local reentrant zones or multiple spiral wavelets of myocardial activation. Due to the absence of organized electrical activity and myocardial depolarization, uniform ventricular contraction does not occur, rendering the heart unable to generate cardiac output.
Mechanisms of Ventricular Tachycardia (VT): In approximately 80% of patients with VT/ventricular fibrillation (VF), sustained ventricular arrhythmias are preceded by an increase in ventricular ectopic beats and recurrent ventricular arrhythmias, particularly multiple episodes of non-sustained VT. The duration of these spontaneous arrhythmias prior to the onset of VT/VF varies. Sustained polymorphic VT can progress to VF, most commonly due to underlying ischemia. VF can also be the primary event in sudden cardiac death.
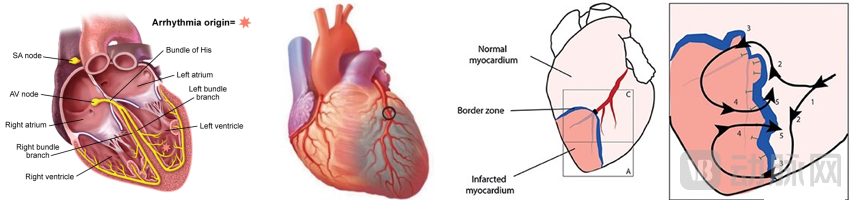
Figure 3. Relationship between sudden cardiac death and coronary heart disease (an example of one mechanism underlying common post-infarction arrhythmias): Ischemia-induced myocardial injury or myocardial scarring → myocardial heterogeneity → inconsistency in electrophysiological properties → reentry → multiple local micro-reentrant circuits → ventricular fibrillation → absence of any organized electrical activity → cardiac arrest (a. Normal cardiac conduction system; b. Distal myocardial ischemia due to vascular occlusion (black circles), resulting in myocardial infarction in the supplied region (gray area); c. Infarcted area (dark red); d. Electrical reentry occurring at the border zone between normal myocardium (light pink) and infarcted myocardium (dark red), leading to ventricular fibrillation.)
2A Vast Potential Patient Population: Patients with Coronary Heart Disease and Heart Failure in the Course of Chronic Diseases
1) Causes of Sudden Cardiac Death
Etiology of Sudden Cardiac Death in Relation to Age and Population: Among patients under 40 years of age with sudden cardiac death (all without pre-existing heart disease), 73% had cardiac causes, while 15% had non-cardiac causes (most commonly intracranial hemorrhage). In individuals under 35 years of age, non-coronary artery disease etiologies are more likely. The incidence of sudden death increases with age in both sexes, but men are more susceptible than women, with a male-to-female ratio of 2–3:1.
The risk of cardiac arrest varies significantly depending on the presence of underlying heart disease: it increases 6- to 10-fold in patients with established heart disease, and 2- to 4-fold in those with risk factors for coronary artery disease. The major causes of sudden cardiac death include:
1. Coronary Artery Disease:The most common cause, with 70% of cardiac arrests attributable to coronary heart disease (58% in patients older than 30 years and 22% in those younger than 30 years). In patients with coronary heart disease, cardiac arrest can occur both during acute coronary syndrome (ACS) and in those with chronic stable coronary heart disease (who typically have prior myocardial injury and scarring that may predispose to cardiac arrest). In fact, sudden cardiac death is more common in patients without identifiable acute cardiac events; more than 50% of cardiac arrests are the initial manifestation of previously unknown or unrecognized heart disease.
2. Other organic heart diseases:Accounting for 10% of out-of-hospital cardiac arrest cases. ① Heart failure (HF) and cardiomyopathy: approximately one-third of deaths are caused by sudden cardiac death.② Left ventricular hypertrophy caused by hypertension or other causes (myocardial hypertrophy caused by hypertension is usually accompanied by myocardial fibrosis, which may create conditions for ventricular arrhythmias); ③ Myocarditis; ④ Hypertrophic cardiomyopathy (13% in patients under 30 years old); ⑤ Arrhythmogenic right ventricular cardiomyopathy; ⑥ Congenital coronary artery anomalies; ⑦ Mitral valve prolapse.
3. No organic heart disease:It accounts for 10%–12% of cardiac arrest cases in individuals under 45 years of age.① Brugada syndrome; ② Idiopathic VF; ③ Long QT syndrome; ④ Familial polymorphic VT; ⑤ Unexplained familial sudden cardiac death; ⑥ WPW syndrome; ⑦ Commotio cordis.
Among them, two major patient populations warrant attention:
1. Coronary Heart Disease
65%–70% of sudden cardiac deaths can be attributed to coronary artery disease, and 30%–50% of coronary deaths are caused by sudden cardiac death. Coronary angiography shows that 71% of survivors of cardiac arrest have significant coronary stenosis (of whom 48% have coronary occlusion), and acute coronary syndrome or myocardial ischemia cannot be excluded in the remaining patients. Approximately 24% of sudden cardiac death cases in individuals under 30–40 years of age are due to coronary artery disease. The incidence of sudden cardiac death is associated with the clinical manifestations of coronary artery disease: inIt is highest among patients with a history of myocardial infarction, intermediate among angina patients without a history of myocardial infarction. However, sudden cardiac death can occur in the presence of asymptomatic ischemia.among patients, and may be the initial presentation of coronary heart disease.
Acute Myocardial Infarction:In patients presenting with acute myocardial infarction (AMI) rather than sudden cardiac death, the incidence of ventricular fibrillation (VF) varies by infarct type and timing: the overall incidence of ventricular tachycardia (VT)/VF in acute ST-segment elevation myocardial infarction (STEMI) is 10.2%, with 80%–85% of such arrhythmias occurring within the first 48 hours. The overall incidence of VT/VF in non-ST-segment elevation acute coronary syndrome (NSTE-ACS) is 2.1%. The median time to arrhythmia onset is 78 hours (interquartile range: 16 hours to 7 days). Multiple studies have shown a peak incidence of VF within the first 48 hours after AMI, presumably due to ischemia, whereas VF occurring later may be associated with scar formation during infarct healing (and an increased risk of monomorphic VT), thereby increasing the risk of late sudden cardiac death. Late sudden cardiac death most commonly occurs within the first year, with the majority happening in the initial few months, and is caused by ventricular tachyarrhythmias. The risk of late-onset VT/VF appears similar in patients with ST-segment elevation and non-ST-segment elevation infarctions. These data exclude patients who died from sudden cardiac death before hospital admission. It is estimated that more than 50% of deaths due to AMI occur out of hospital, with the majority occurring within one hour of symptom onset.
Myocardial Ischemia:Unstable coronary artery lesions are present, which may lead toAcute ischemic events (without infarction) and can lead to electrical instability. 76% of patients with cardiac arrest haveSignificant coronary artery lesions, spasm, or unstable plaques,Nearly 1/2 of patients have coronary artery occlusion.Even after successful revascularization, patients who are not in the acute phase of myocardial infarction may still face a persistently high risk of recurrent ventricular tachycardia (VT) or ventricular fibrillation (VF).
2. Heart Failure
Heart failure is a relatively common cause of sudden cardiac death. Thirty to fifty percent of deaths in patients with heart failure are attributable to sudden cardiac death, and the incidence of sudden cardiac death increases during periods of worsening heart failure symptoms. The incidence of sudden cardiac death in patients with heart failure is five times that in patients without heart failure, with the absolute risk in female patients being one-third of that in male patients.
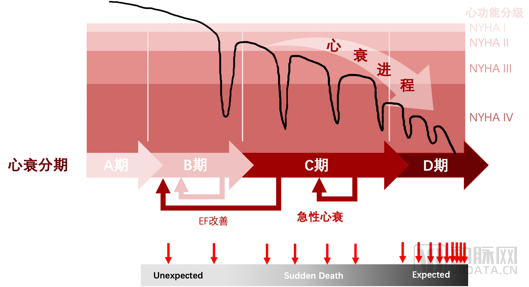
Figure 4. Correlation between the progression of heart failure and the incidence of sudden cardiac death: As heart failure progresses from the early stages (Stages A and B, or NYHA Class II) to the moderate and end-stage phases (Stages C and D, or NYHA Classes III and IV), the incidence rate and probability of sudden death increase progressively (the red arrow below indicates the frequency of sudden death).
Among the causes of death in patients with heart failure, progressive pump failure, unexpected sudden cardiac death (usually caused by ventricular tachyarrhythmias, and sometimes by asystole or pulseless electrical activity), and sudden cardiac death occurring during episodes of clinical worsening of heart failure each account for approximately one-third of all heart failure-related deaths. Sudden death in 39% of heart failure patients is considered to be caused by arrhythmias. The progression from ventricular tachycardia (VT) to ventricular fibrillation (VF) is the most common cause of sudden cardiac death, while bradyarrhythmias or pulseless electrical activity (PEA) are responsible for 5%-33% of cases. Acute coronary events may serve as triggers for sudden death in some heart failure patients. Among heart failure patients with significant coronary artery disease, 54% of those who experienced sudden death and 32% of those who died from heart failure had acute coronary lesions.
The more severe the heart failure, the higher the overall mortality rate and the absolute incidence of sudden cardiac death (Figure 4). The mortality rate and mode of death in patients with heart failure vary according to the severity of heart failure and the type of cardiomyopathy. Patients with NYHA class II or III heart failure are more likely to experience “sudden” cardiac death, whereas those with NYHA class IV heart failure are more likely to die from “pump” failure (Figure 5), with ventricular tachycardia (VT) and ventricular fibrillation (VF) remaining the most common arrhythmias leading to sudden cardiac death. The MERIT-HF study showed that the higher the severity of heart failure (NYHA classes II, III, and IV), the greater the likelihood of sudden cardiac death within one year (6.3%, 10.5%, and 18.6%, respectively); however, the proportion of total deaths attributable to sudden cardiac death decreased (64%, 59%, and 33%, respectively).
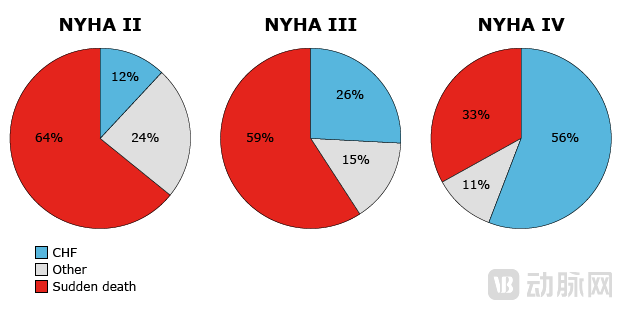
Figure 5. Causes of death in heart failure patients are associated with the severity of heart failure; sudden cardiac death is predominant in early-to-mid stages (NYHA class II and III).
2) “Triggers”—Acute Precipitating Factors
In addition to underlying structural heart disease, certain transient or reversible causes may precipitate arrhythmias and sudden cardiac death (SCD). Identifying these causes is crucial for treating the underlying conditions and assessing the risk of SCD recurrence. Potentially reversible triggers of SCD include: ① Acute myocardial ischemia and myocardial infarction: Coronary artery disease is the most common cause of SCD; therefore, acute coronary ischemia should be considered in all survivors of SCD; ② Heart failure: The incidence of SCD may increase during periods of worsening heart failure symptoms; ③ Autonomic nervous system activation, particularly sympathetic stimulation, such as sudden emotional agitation; ④ Other factors: Antiarrhythmic drugs, toxins, electrolyte abnormalities, acidosis, and severe hypoxemia.
Based on the above, various cardiac diseases carry the risk of sudden cardiac death (SCD), and indeed, many patients with coronary heart disease present with SCD as their initial manifestation. Therefore, prevention is particularly crucial for the large population of patients at high risk of SCD due to cardiovascular disease. Currently, in accordance with guidelines for the prevention and treatment of cardiovascular diseases, China has established standards and measures for both primary and secondary prevention of SCD. Primary prevention involves identifying patients with high-risk factors through clinical diagnosis and implanting an implantable cardioverter-defibrillator (ICD) at an early stage. Secondary prevention targets patients who have already experienced SCD, aiming to prevent recurrence through ICD implantation. However, secondary prevention strategies are limited to those who have already suffered SCD and fail to cover the broader high-risk population. In Europe and the United States, primary prevention—targeting high-risk individuals who have not yet experienced SCD—is widely accepted and implemented.
1Indication Dimension: Stratification Strategy and Logic
Although implantable cardioverter-defibrillators (ICDs) are highly effective in treating ventricular tachyarrhythmias and preventing sudden cardiac death, they are costly, require ongoing follow-up, and carry numerous risks during implantation and throughout the device’s lifespan (such as bleeding, pneumothorax, perforation, infection, and device or lead malfunction). Moreover, only a subset of patients with cardiomyopathy experience sustained ventricular tachyarrhythmias or sudden cardiac death. Therefore, risk stratification should be performed prior to ICD therapy to target treatment to patients at the highest risk of sudden cardiac death and to minimize ICD implantations in those unlikely to benefit. The primary indicators for risk stratification for sudden cardiac death to guide primary prevention ICD implantation mainly include: ① etiology of left ventricular dysfunction; ② left ventricular ejection fraction (LVEF); ③ classification of heart failure symptoms; ④ life expectancy exceeding one year; ⑤ inducibility of sustained ventricular tachycardia; and ⑥ non-sustained ventricular tachycardia detected on electrocardiographic monitoring.
The key indicators primarily cover two major areas.:① Patients with significantly reduced LVEF appear to be at the highest risk, and also derive the greatest benefit from primary prevention with ICD implantation;② Risk factors for sudden cardiac death after acute myocardial infarction include: Left ventricular dysfunction or reduced LVEF; symptoms and severity of heart failure; left ventricular aneurysm; Q waves on surface electrocardiogram; intraventricular conduction delay, etc.
Patients for whom ICD implantation is recommended for the primary prevention of sudden cardiac death are as follows (Figure 6):
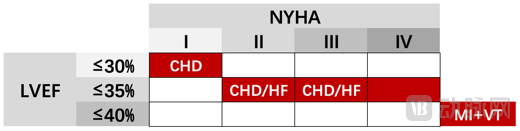
Figure 6. A simple matrix of patient selection criteria for primary prevention of sudden cardiac death: Patients with poor cardiac function (EF indicates cardiac pumping capacity; NYHA classifies cardiac function based on symptoms) are at high risk of sudden death, particularly those with underlying conditions such as cardiomyopathy and heart failure caused by myocardial ischemia due to coronary heart disease (CHD: coronary heart disease or ischemic cardiomyopathy; HF: heart failure; MI: myocardial infarction; VT: ventricular tachycardia).
① Patients with cardiomyopathy due to ischemic heart disease, left ventricular ejection fraction (LVEF) ≤35%, and New York Heart Association (NYHA) class II or III heart failure should undergo ICD evaluation at least 40 days after myocardial infarction and more than 3 months after revascularization and initiation of guideline-directed medical therapy.
② Patients with ischemic cardiomyopathy due to ischemic heart disease, LVEF ≤30%, and NYHA class I status should undergo ICD evaluation at least 40 days after myocardial infarction and more than 3 months after revascularization and guideline-directed medical therapy.
③ Patients with a history of myocardial infarction (MI)-related non-sustained ventricular tachycardia (NSVT), left ventricular ejection fraction (LVEF) ≤40%, and inducible sustained ventricular tachycardia (VT) or ventricular fibrillation (VF) during electrophysiological study (EPS). Patients should be beyond the acute phase of MI, receiving guideline-directed medical therapy, and have an expected survival of at least 1 year. Patients with reduced LVEF due to MI are at increased risk of sudden cardiac death, most commonly caused by rapid ventricular arrhythmias. For specific patients with ischemic cardiomyopathy, prophylactic implantable cardioverter-defibrillator (ICD) implantation for primary prevention of sudden cardiac death can reduce mortality.
④ For patients with non-ischemic dilated cardiomyopathy, LVEF ≤35%, and NYHA class II or III heart failure, ICDs can significantly reduce all-cause mortality and mortality due to sudden cardiac death. All patients receiving an ICD for primary prevention of sudden cardiac death should undergo at least 3 months of guideline-directed medical therapy prior to ICD implantation.
⑤ For patients with an LVEF ≤35%, NYHA class III or IV heart failure, and a QRS duration ≥120 ms, implantation of a CRT-D device (biventricular pacing combined with an ICD) is recommended over implantation of an ICD alone. CRT should be most strongly considered for patients with left bundle branch block (LBBB) morphology, a QRS duration ≥150 ms, and those who are dependent on ventricular pacing due to atrioventricular conduction block.
2Primary Prevention: Preventing Sudden Cardiac Death in At-Risk Populations
1) General Population: Risk Stratification and Reduction of Risk Factors
Screening and Risk Stratification: For populations with a known elevated risk of cardiac arrest (e.g., prior myocardial infarction), further risk stratification through testing is used to identify patients who would benefit from an implantable cardioverter-defibrillator (ICD). For the general population without known cardiovascular disease, guidelines recommend screening for cardiovascular risk factors and, as appropriate, screening for coronary artery disease in selected patients.
Lifestyle Intervention: Many traditional risk factors associated with the development of coronary heart disease (CHD) are also linked to cardiac arrest; therefore, targeted interventions addressing these risk factors can reduce the incidence of cardiac arrest. Interventions include: effective management of hypercholesterolemia and hypertension; adoption of a heart-healthy diet; regular physical exercise; smoking cessation; moderate alcohol consumption; and effective management of diabetes. Although there is no definitive evidence that reducing risk factors in the general population lowers the incidence of cardiac arrest, since most CHD-related deaths result from sudden cardiac death, studies have confirmed that interventions aimed at reducing risk factors can lower overall cardiovascular and coronary artery disease-related mortality, thereby reducing the incidence of cardiac arrest.
2) Patients with ischemic heart disease (coronary heart disease)
Patients with ischemic heart disease are at increased risk of cardiac arrest, particularly those with a history of myocardial infarction. The risk of cardiac arrest after myocardial infarction is significantly increased by several factors. Methods to prevent cardiac arrest in such patients include: ① Standard pharmacological therapy. Beta-blockers and angiotensin-converting enzyme inhibitors can reduce overall mortality after myocardial infarction and may be used routinely. These agents can also reduce the incidence of sudden cardiac death. ② Should undergoRisk Stratification to Identify Patients at Highest Risk of Cardiac Arrest③ Implant an ICD in selected patients.
Research on Primary Prevention of ICD Implantation in Ischemic Cardiomyopathy Shows That ICDs Significantly Improve Survival: The MADIT-I TrialThe Multicenter Automatic Defibrillator Implantation Trial (MADIT) was the first clinical study to demonstrate the efficacy of implantable cardioverter-defibrillators (ICDs) in the primary prevention of sudden cardiac death among certain high-risk, asymptomatic patients. These patients had a history of myocardial infarction with reduced left ventricular ejection fraction (LVEF ≤35%), nonsustained ventricular tachycardia (NSVT) on electrocardiographic monitoring, and inducible sustained monomorphic ventricular tachycardia (VT) during electrophysiological study (EPS), which remained inducible even after intravenous administration of procainamide. Compared with the pharmacological therapy group, patients in the ICD group exhibited significantly reduced all-cause mortality, cardiac mortality, and arrhythmic mortality (Figure 7, left panel).MADIT-II Trial:Patients with a prior myocardial infarction occurring more than 30 days before enrollment and reduced left ventricular ejection fraction (LVEF ≤30%). The all-cause mortality rate was lower in the ICD group than in the medical therapy group (ICD group 14.2% vs. conventional therapy group 19.8%; HR 0.65, 95% CI 0.51–0.93) (Figure 7, right panel).
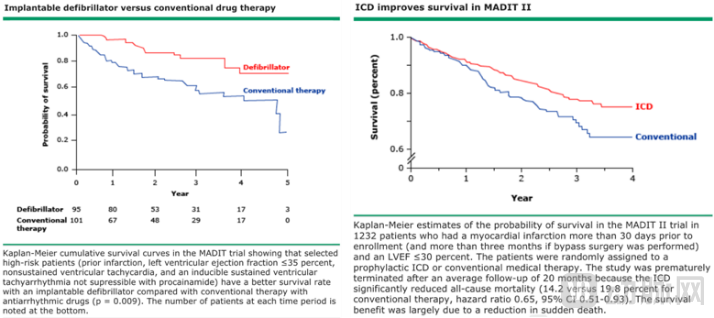
Figure 7. The left panel shows the MADIT-I trial, and the right panel shows the MADIT-II trial; both demonstrate a significant increase in survival among patients at high risk of sudden cardiac death following primary prevention with an implantable cardioverter-defibrillator (ICD).
3) Patients with heart failure and cardiomyopathy
The risk of sudden cardiac death increases with worsening left ventricular systolic dysfunction and greater severity of clinical heart failure,Regardless of the underlying etiology, patients with heart failure and left ventricular systolic dysfunction are at an increased risk of cardiac arrest. In patients with heart failure and cardiomyopathy, the role of implantable cardioverter-defibrillators (ICDs) in the primary prevention of sudden cardiac death depends on several factors:Severity of left ventricular systolic dysfunction; severity of clinical heart failure; etiology of left ventricular dysfunction (ischemic vs. non-ischemic cardiomyopathy); competing risks affecting life expectancy and ICD complication riskComorbidities (chronic kidney disease, chronic obstructive pulmonary disease, etc.). Meanwhile,The risk of death from other causes (progressive heart failure) also increases with worsening heart failure and left ventricular systolic function.Therefore, appropriate patient selection is critically important prior to ICD implantation for primary prevention.
4) Congenital conditions associated with an increased risk of cardiac arrest (e.g., Brugada syndrome, congenital long QT syndrome, and WPW).
31.5-Level Prevention: Necessary and Sufficient Interventions for Target Populations in the Context of China
In China, the number of patients meeting the indications for primary prevention significantly exceeds those requiring secondary prevention; however, few patients utilize preventive devices for the prevention of sudden cardiac death (SCD). Currently, the implantation rate of implantable cardioverter-defibrillators (ICDs) in China is only 1.4 per million people, and existing medical resources are insufficient to meet the primary prevention needs for SCD given the country’s large population base. Factors hindering the implementation of primary prevention include health insurance policies, a lack of evidence-based medical data, and patients’ limited understanding of or even fear toward implantable ICDs, all of which contribute to many patients refusing ICD implantation.
To further enhance the awareness of patients, physicians, and other stakeholders regarding the use of implantable cardioverter-defibrillator (ICD) therapy for the prevention of sudden cardiac death (SCD), and to strengthen targeted prevention efforts for patients at extremely high risk, the Chinese Society of Pacing and Electrophysiology has proposed a "Level 1.5 Prevention" strategy tailored to Chinese patients. This approach expands upon the international indications for primary prevention by adding one of four major high-risk factors: left ventricular ejection fraction (LVEF) <30%, frequent premature ventricular contractions (PVCs), non-sustained ventricular tachycardia (NSVT), or syncope and presyncope. The introduction of the Level 1.5 Prevention concept holds practical significance for advancing the prevention and treatment of SCD. The population covered under Level 1.5 Prevention represents those for whom ICD implantation is both fully indicated and necessary. Compared with primary prevention, this approach narrows the scope, offering greater specificity and necessity, thereby indirectly reducing the financial burden on both medical insurance systems and patients.
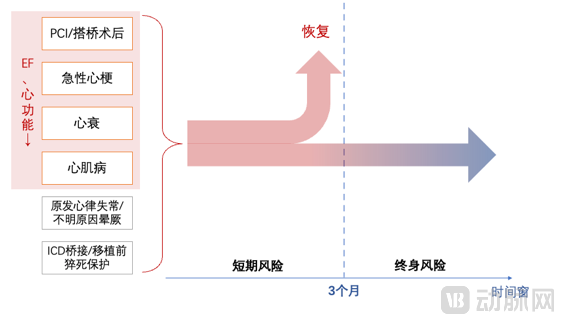
Figure 8. After risk stratification of patients at high risk for sudden cardiac death, the prevention time window is divided by a 3-month threshold into short-term and long-term risks, allowing for the selection of corresponding preventive strategies.
Currently, the time window for primary prevention of sudden cardiac death (as mentioned above) involves evaluating and considering ICD implantation only after three months post-revascularization. However, patients remain at high risk during this initial three-month period. Data from large-scale U.S. national registries, including the National Cardiovascular Data Registry (NCDR) and The Society of Thoracic Surgeons (STS) Adult Cardiac Surgery Database, indicate that patients with left ventricular dysfunction (e.g., LVEF ≤30%) have significantly higher mortality rates in the early period following PCI or CABG. Specifically, 30-day mortality after CABG is significantly higher in patients with marked left ventricular dysfunction compared to those with normal left ventricular function. These patients face not only an increased risk of sudden cardiac death due to ventricular arrhythmias but also an elevated risk of death from non-arrhythmic events. Meanwhile, both domestically and internationally, clinical practice faces challenges regarding short- to medium-term ICD implantation for sudden cardiac death prevention: In the United States, reimbursement does not cover the cost of ICD implantation for primary prevention within three months after CABG or PCI. In China, due to concerns about the invasiveness of ICD implantation and its cost, clinicians often spend considerable time persuading patients, a duration that may well exceed the high-risk window for these patients. Therefore, the key lies in how to prevent sudden cardiac death within the first three months using methods that are more acceptable to patients, namely non-invasive and moderately priced approaches.
For the temporary management of patients at high risk for sudden cardiac death, the wearable cardioverter-defibrillator (WCD) can be used as an alternative measure to prevent sudden cardiac death. The WCD is an external vest-style defibrillation device capable of automatically detecting ventricular tachycardia (VT) and ventricular fibrillation (VF) and delivering non-invasive defibrillation. According to the 2016 American Heart Association (AHA) Scientific Statement, the Heart Rhythm Society (HRS), and the 2017 AHA/American College of Cardiology (ACC)/HRS Guidelines, the following patients may benefit from temporary use of a WCD:
① LVEF ≤35% within 40 days after myocardial infarction: A wearable cardioverter-defibrillator (WCD) is recommended for active patients with NYHA class II–III heart failure, or those with LVEF <30% and NYHA class I heart failure, as these patients may require implantable cardioverter-defibrillator (ICD) implantation after the 40-day period. LVEF should be reassessed 1–3 months post-myocardial infarction; if LVEF remains ≤35% despite optimal medical therapy, ICD implantation is indicated and should be considered.
② LVEF ≤35% and coronary artery bypass grafting (CABG) revascularization within the past 3 months: WCD as primary prevention for sudden cardiac death. Meanwhile, LVEF should be reassessed 3 months after CABG; if sustained ventricular tachyarrhythmias occur or LVEF remains ≤35%, ICD implantation is generally indicated.
③ Newly diagnosed non-ischemic cardiomyopathy: For patients with severe but potentially reversible cardiomyopathy, such as those with tachycardia-induced or myocarditis-associated cardiomyopathy, a wearable cardioverter-defibrillator (WCD) may help prevent sudden cardiac death due to ventricular arrhythmias while awaiting improvement in left ventricular function, implantable cardioverter-defibrillator (ICD) implantation, or heart transplantation if necessary.
④ Transition to heart transplantation: Patients with severe heart failure awaiting heart transplantation are at particularly high risk of sudden cardiac death, and implantation of an ICD is generally recommended. A WCD may be a reasonable non-invasive alternative, especially for patients who have not yet received an ICD implant and are expected to have a shorter waiting time.
⑤ Bridging to indicated or interrupted ICD therapy: Some patients with indications for ICD implantation may need to postpone the procedure due to comorbidities (such as infection, postoperative recovery, or lack of vascular access). Additionally, some patients with an implanted ICD may require device explantation due to infection. For these patients, a wearable cardioverter-defibrillator (WCD) can protect against ventricular tachyarrhythmias until the patient is eligible for initial or repeat ICD implantation.
IV. Outlook
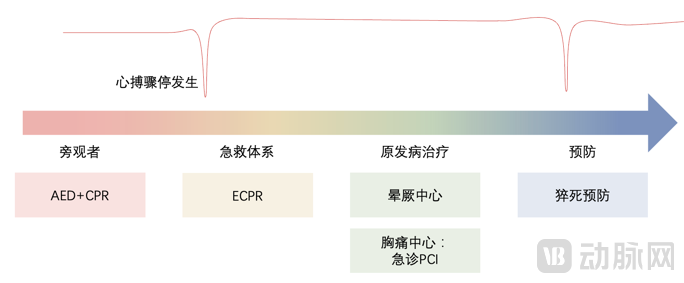
Figure 9. The emergency response, treatment, and prevention of sudden cardiac death involve multi-sectoral coordination; close collaboration between public health and clinical sectors is required at each stage to achieve optimal outcomes.
● First-Line Emergency Response—Bystander CPR and AED
China has a high population density and, consequently, a large absolute number of individuals at risk for sudden cardiac death (SCD). The most effective approach to addressing pre-hospital emergency care challenges is the implementation of “public access defibrillation.” This strategy involves equipping public transportation hubs, shopping malls, and sports venues with automated external defibrillators (AEDs), enabling bystanders to administer defibrillation before professional emergency responders arrive. By expanding the pool of potential rescuers capable of providing early defibrillation, this approach maximizes the capacity to address emergency needs among SCD patients within China’s large population base. Meanwhile, due to historically prominent and widely circulated unfavorable legal precedents concerning Good Samaritan acts that have attracted significant public attention, the Chinese public harbors specific concerns regarding civil liability. Alleviating the burden on “bystanders” requires more positive public opinion campaigns and media outreach.
In cases of cardiac arrest, defibrillation alone is insufficient to restore spontaneous circulation; effective, high-quality CPR is critical to successful resuscitation, underscoring the urgent need to strengthen emergency response training. Implementing such training requires multi-sectoral collaboration and seamless coordination among health administrative authorities for guidance, educational institutions for training, and public welfare organizations for support. This integrated approach is essential to address current gaps in public services, maximize the utilization of public health resources, and ultimately improve survival rates from sudden cardiac death in China.
● Advanced Life Support—ECPR
When cardiac arrest persists for more than 30 minutes without sustained return of spontaneous circulation, extracorporeal cardiopulmonary resuscitation (ECPR) is required to provide adequate circulatory perfusion. This approach aims to minimize the duration of low-flow state following cardiac arrest and reduce complications arising from post-resuscitation hypoperfusion of vital organs, thereby effectively safeguarding critical organ functions—particularly neurological function—as well as renal and hepatic functions. However, the success of ECPR relies heavily on a robust ECMO team and subsequent intensive care unit (ICU) management. In China, the coordination between emergency medical services and critical care clinical practices requires further strengthening. This can be achieved by improving the integration of emergency networks and expanding regional coverage of ECPR response capabilities, as well as by enhancing specialized training in ECPR techniques and ECMO management for professional teams. Where feasible, mobile ECMO units should be deployed to enable on-site ECPR, thereby minimizing the accessibility radius and maximizing timely intervention.
● Addressing primary diseases—establishment of Chest Pain Centers and Syncope Centers
Since nearly 70% of sudden cardiac deaths are caused by coronary heart disease (CHD), and sudden death is often the initial manifestation of CHD, it is particularly important to address both resuscitation and treatment of the underlying condition within their respective therapeutic time windows during emergency care for sudden cardiac arrest. To improve early diagnosis and treatment for patients with acute chest pain, China has established a nationwide Chest Pain Center system; since its inception in 2015, more than 1,000 such centers have been set up across the country. These Chest Pain Centers feature emergency green channels that enable rapid and accurate diagnosis, risk stratification, and treatment. Their catheterization laboratories operate 24 hours a day, 365 days a year, allowing for immediate emergency percutaneous coronary intervention (PCI), thereby effectively reducing mortality among patients with chest pain.
Furthermore, among the symptoms observed in survivors of cardiac arrest, syncope may present as a warning sign. Syncope is a disturbance of consciousness caused by cerebral hypoperfusion, with etiologies primarily including cardiogenic syncope, neurally mediated reflex syncope, and orthostatic syncope. Due to the multidisciplinary nature of its diagnosis, involving both cardiovascular and neurological fields, accurate diagnosis is challenging; in the absence of standardized management, diagnostic rates are low while misdiagnosis rates are high. To address this, experts recommend establishing syncope centers and dedicated syncope clinics in tertiary hospitals to provide centralized and standardized management for patients with transient loss of consciousness. In 2019, China launched the construction of syncope centers in the first batch of 72 hospitals, which were officially designated. Staffed by specially trained physicians and nurses, these centers unify diagnostic criteria and treatment protocols, oversee patient management and follow-up, emphasize risk stratification for syncope patients, actively treat cardiac diseases, and prevent the occurrence of malignant arrhythmias.
● Sudden Cardiac Death Prevention—High-Risk Stratification and ICD
Primary prevention relies on risk stratification by cardiologists in relevant subspecialties. Secondary prevention depends on prompt intervention following detailed assessment in outpatient or syncope clinics.
Primary prevention emphasizes screening for and managing risk factors for coronary heart disease in the general population without known heart disease, with a focus on lifestyle modifications and interventions. For patients with heart disease at increased risk of cardiac arrest, such as those with a history of myocardial infarction, cardiomyopathy, or heart failure, the primary preventive measures include standard pharmacological therapy, implantation of an implantable cardioverter-defibrillator (ICD) in selected patients after determining their risk stratification for cardiac arrest, and consideration of a non-implantable wearable cardioverter-defibrillator (WCD) for patients at short-term risk. Once cardiac arrest occurs, it falls within the scope of secondary prevention of sudden cardiac death, focusing on comprehensive evaluation and secondary prevention for survivors of cardiac arrest. After cardiopulmonary resuscitation, survivors of cardiac arrest require identification and treatment of acute reversible causes, assessment for structural heart disease and/or primary electrical disorders, neurological evaluation, and family member assessment in specific cases. Secondary prevention of sudden cardiac death typically involves the use of an ICD, which is suitable for most survivors of cardiac arrest.
● AED Accessibility
Mobile AEDs Shorten Response Radius: In addition to increasing the deployment density of AEDs, further enhancing AED coverage efficiency within the "golden four minutes" can be achieved through mobile AEDs. The rescue coverage efficiency of mobile AEDs is six times that of fixed AEDs, significantly expanding the potential treatment range of AEDs.
Mobile App for Monitoring Cardiac Arrest Patients and Notifying Nearby Volunteers for Immediate First Aid: Consider developing a mobile application capable of detecting cardiac arrest incidents and automatically alerting the 120 emergency medical services (EMS) system. The emergency dispatch center would then assign volunteers located within a four-minute travel distance from the incident site to respond, guided by the app’s map-based positioning features to reach the patient and provide care. For cardiac arrests occurring in certain public areas or private residences, this approach may help increase the rates of early CPR and improve survival outcomes.
Home AED Deployment: Since approximately three-quarters of cardiac arrests occur at home, having an automated external defibrillator (AED) available for home use may reduce mortality rates.
● ECPR Accessibility
Unlike automated external defibrillators (AEDs), extracorporeal membrane oxygenation (ECMO) systems are not suitable for deployment in routine public spaces, making it impractical to increase their availability density through large-scale regional distribution. Currently, extracorporeal cardiopulmonary resuscitation (ECPR) still relies on technical support from central hospitals within a given region. To improve the accessibility of ECPR, a key direction is enhancing the portability and miniaturization of ECMO devices. Portable ECMO units are significantly more compact and lightweight than conventional ICU-based ECMO systems, allowing a single person to easily carry them onto helicopters or ambulances. Given the specific demands of long-distance patient transport, these devices must simultaneously ensure high stability during transit, provide impact protection, and offer extended battery life.
● Minimally Invasive and Non-Invasive Defibrillation: WCD and SICD
Currently, the implantable cardioverter-defibrillator (ICD) is the preferred treatment for preventing sudden cardiac death (SCD). Traditional ICD implantation involves delivering leads via peripheral veins to the right ventricle, with the pulse generator and lead system implanted subcutaneously in the left chest. Although ICDs are widely used, their complications, particularly those related to transvenous leads, have long posed clinical challenges. Due to the frequent failure of defibrillation leads and the high incidence of complications associated with the transvenous approach, the subcutaneous implantable cardioverter-defibrillator (S-ICD) has been increasingly adopted in clinical practice in recent years. Both its leads and pulse generator are located subcutaneously, with the defibrillation leads not directly contacting the heart or veins, thereby effectively addressing the need for long-term SCD prevention. Nevertheless, a subset of patients at high risk for SCD still does not meet the implantation indications outlined in current guidelines. A significant proportion of these patients are in a short-term high-risk state following discharge after myocardial ischemia and related revascularization procedures, creating a more urgent need for short-term SCD prevention through non-invasive defibrillation. The wearable cardioverter-defibrillator (WCD), being non-invasive and easy to wear, effectively addresses the challenge of SCD prevention in these patients.
Dr. Chen Yang oversees investments in innovative medical devices at Northern Light Venture Capital, bringing over a decade of experience in clinical practice and early-stage healthcare investment. Prior to entering the investment field, Dr. Chen worked on the clinical frontlines for many years at Fuwai Hospital, National Center for Cardiovascular Diseases, and Beijing Anzhen Hospital. He possesses extensive clinical expertise and industry resources, having participated in several international multicenter academic studies and large-scale clinical trials of cardiovascular devices, as well as the early research and development of multiple innovative medical devices. Dr. Chen also serves as a startup mentor for several clinical translation centers in China, providing guidance on zero-to-one sector selection, strategic direction, and device R&D, with a commitment to advancing China’s domestic medical device innovation driven by clinical needs.
Dr. Yang Chen holds a Master’s degree and a Ph.D. in Medicine from Peking Union Medical College, as well as a Bachelor’s degree in Clinical Medicine from Shanghai Jiao Tong University School of Medicine.
