What Constitutes an Ideal Medical Device? Insights from Pan Wenzhi, Shen Li, and Ge Junbo
As China’s national strength continues to grow, the development levels across all industries have significantly improved. In certain fields, China has even taken a global lead, such as in aerospace, high-speed rail, quantum information, ultra-high-voltage power transmission, and 5G technology, giving rise to world-leading companies like Huawei and DJI. Industries are gradually moving away from imitating foreign products and entering a new era of independent and original innovation.
Currently, the state’s advocacy for and emphasis on innovation and intellectual property protection have reached an unprecedented level, with the important assertion that “innovation is the primary driving force leading development.” As in other industries, the development of medical devices in China has historically relied largely on imitating foreign products. Encouragingly, under the current national strategy and overall development trends, a steady stream of domestically originated medical devices has emerged in recent years, demonstrating a positive momentum of growth.
The establishment of the China Cardiovascular Physicians Innovation Club (CCI) responds to the national “Mass Entrepreneurship and Innovation” strategy and aligns with industry development trends. Based on our review of the history of medical devices, summary of personal experience in device research and development (R&D), and tracking of products developed by CCI members, this article aims to briefly outline our understanding of ideal medical devices.
We believe that an ideal medical device must adhere to the following five core principles:
Medical devices are intended for patients, while their users are physicians; therefore, clinical needs and physicians’ user experience are of paramount importance. Clinical demand can be regarded as the lifeblood of medical devices. If a device does not address genuine clinical needs or merely responds to pseudo-demands, it will become unsustainable—like water without a source or a tree without roots—regardless of how powerful its functions or how perfect its design may be, ultimately leading to non-adoption.
In Stanford University’s innovation curriculum, identifying clinical needs is the first step. It is a detailed and systematically trained component that constitutes a significant portion of the entire course. The term “clinical need” encompasses at least two aspects: First, there must be a sufficiently large target population, meaning a substantial number of patients. Second, it must represent an unmet hard need. Occasionally, certain apparent needs may seem pressing but actually have better alternative solutions or do not address genuine clinical pain points; such cases require technical discernment.
However, demand is also somewhat elastic; if a medical device is sufficiently safe, effective, and user-friendly, it can sometimes create new demand. Identifying clinical needs is not simple; it is a complex systemic process that requires specialized expertise. Accordingly, we have prioritized such courses in the CCI training program. Medical devices are generally used by physicians, although some devices are designed for patient self-use. As with other industrial products, user experience is critically important. If a product is cumbersome to use and has a steep learning curve, its adoption and market penetration will be limited.
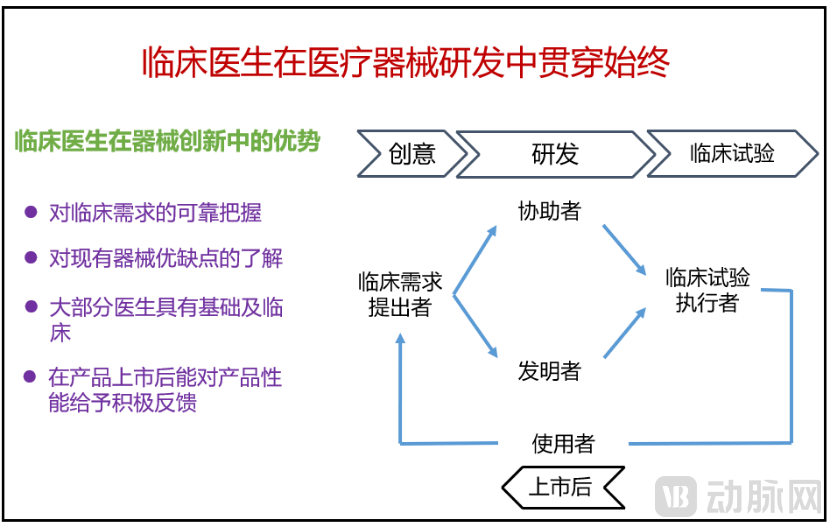
Figure 1 The Role of Physicians in the Research and Development of Medical Devices
The Tao Te Ching states, “At the origin of all things, the Great Way is supremely simple, yet its evolution leads to utmost complexity.” Medical devices differ from other industrial products in that the individual patients and application environments involved exhibit significant variability. Moreover, unlike automobiles or mobile phones, they cannot undergo large-scale, challenging, or even destructive testing prior to market launch (indeed, clinical trials for medical devices typically select classic, straightforward cases). Therefore, it is essential to address these challenges through concise and clear methods, applying invariant principles to accommodate variable conditions, thereby minimizing the occurrence of extreme adverse events during widespread post-market use.
From a probabilistic perspective, we can explain this principle. If the probability of failure for each component of a medical device is 1%, and the device has 10 components, then its overall probability of failure is (1 - 0.99^10) * 100% = 9.6%. If failures resulting from interactions among these components are also taken into account, the failure rate can be significantly higher than 10%. The same logic applies to surgical procedures: the greater the number of steps required in a surgery, the higher the probability of errors.
A review of medical devices that have been widely used throughout history and in current clinical practice reveals that they are all characterized by simple designs and ease of use. Stents (Figure 2), occluders, and balloons all feature straightforward structures, minimal components, and simplified procedural steps. Even TAVI valves, a representative recent innovation for structural heart disease, exhibit a highly streamlined design. Taking balloon-expandable valves as an example, their composition consists solely of a bioprosthetic valve leaflet, an outer skirt, and a laser-cut integrated metal stent. The procedural steps are equally straightforward: once the valved stent is properly positioned, inflating the balloon completes the implantation. The simplicity of device design not only enhances user convenience but, more importantly, reduces the failure rate and improves device stability. Therefore, identifying the most concise solution to hit the mark directly is the core challenge in medical device innovation.
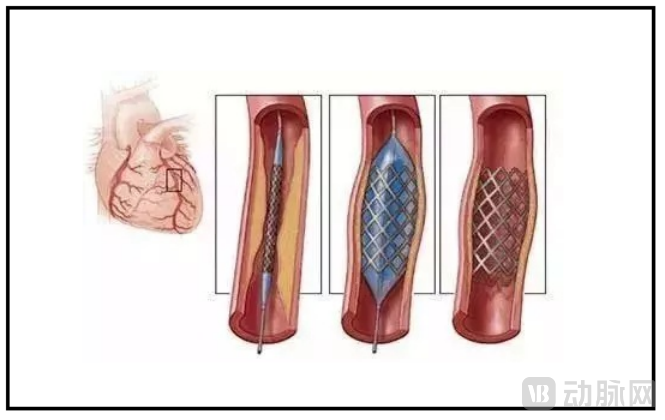
Figure 2. The Implantation Procedure of Coronary Stents
Medical devices. These four words already elucidate their inherent attributes. First, as they are used for medical diagnosis or treatment, they must be grounded in reliable medical principles. In the process of medical device innovation, leveraging previously validated and mature medical principles, or even modifying existing mature medical devices, represents the most prudent approach. Admittedly, novel medical principles or new device designs can be proposed and created; however, this necessitates re-validation, which is a lengthy and arduous process. Take the currently prominent transcatheter edge-to-edge repair (TEER) device, MitraClip, as an example (Figure 3); it is based on the surgical edge-to-edge repair technique.
Medical principles represent a fundamental directional issue in the innovation of medical devices. If the underlying principle is flawed or imperfect, the direction itself is erroneous, rendering all subsequent efforts futile. Of course, once a medical principle is proposed, it must be implemented through a specific product (device), and the development of such a product requires industrial and engineering technologies. Without reliable engineering and technical support, even a sound medical principle remains merely an unfeasible concept. Therefore, industrial and engineering technologies constitute the foundational prerequisite for innovation in medical devices.
Historically, the lag in medical device innovation in China was largely attributable to backwardness in related industrial technologies, subpar raw materials and processing capabilities, and an incomplete supply chain. Creative engineers design novel medical devices by applying established medical principles alongside their expertise in mechanical and industrial engineering. These engineers are responsible for optimizing product performance, enhancing system stability, and enabling scalable mass production. Throughout this process, the participation of medical professionals is essential to provide clinical feedback. Thus, innovation in medical devices is invariably the outcome of close collaboration between medicine and engineering.

Figure 3. MitraCTechnical Principles and Device Design of LIP
A review of the history of medical technology development reveals an evolution from highly invasive to minimally invasive, and from minimally invasive to non-invasive procedures. The pursuit of minimally invasive and non-invasive approaches remains a perpetual theme in the advancement of medical technology. This trend is evident in the evolution of medical devices: stent implantation has replaced coronary artery bypass grafting; endovascular stent grafts have supplanted open vascular surgery; laparoscopic and thoracoscopic techniques have taken the place of traditional open abdominal and thoracic surgeries; and endoscopic treatments and percutaneous interventions have emerged prominently. All these developments exemplify this overarching pattern.
Currently, structural heart disease represents the most significant trend in the development of interventional cardiology, focusing on the research and development of transcatheter minimally invasive techniques to replace traditional surgical procedures. However, there may be differences in efficacy between minimally invasive therapies and traditional open-heart surgery, with the former potentially being slightly inferior. This is because open-heart surgery allows for direct visualization of the lesion site with ample local operating space, enabling a wide range of surgical maneuvers. In contrast, minimally invasive procedures are typically performed in confined spaces, under indirect imaging guidance, and with limited devices, which may restrict the ability to perform complex surgical operations and lesion interventions. Consequently, in certain technical scenarios and patient cases, outcomes may be poorer than those achieved with traditional open-heart surgery, potentially leading to postoperative recurrence.
At this point, the re-intervention capability of the technology becomes crucial. Examples include valve-in-valve TAVR for failed TAVR bioprostheses, repeat radiofrequency ablation for recurrent arrhythmias, and repeat percutaneous coronary intervention for new lesions following stent implantation. If minimally invasive re-interventions are feasible and effective for these patients, then such technologies and medical devices can be considered ideal.
An ideal medical device must be a perfect fusion of science and art, possessing both scientific value and aesthetic appeal. A close examination of any implantable medical device reveals that its form invariably features a streamlined, aesthetically pleasing design, standing in stark contrast to the angular designs typical of many industrial products. This is because eliminating sharp edges and adopting a streamlined shape minimizes damage to surrounding human tissues during surgical procedures and after implantation. Furthermore, streamlined designs ensure uniform stress distribution, preventing fracture due to localized stress concentrations and thereby enhancing fatigue durability. The streamlined design of extracorporeal operating systems, such as delivery systems, also improves user experience by adhering to ergonomic standards, while aesthetic enhancements increase the product’s visual appeal and foster greater user affinity.
In the process of research and development and innovation in medical devices, it is often surprising to find that when a device’s performance reaches its peak perfection, its form also achieves its greatest aesthetic appeal. In essence, the human body and its organs represent a perfect fusion of science and art. Devices implanted in or used by the human body must adhere to this principle to ensure biocompatibility.

Figure4 Several Classic Medical Device Designs
In summary, the research and development (R&D) of medical devices in China has entered a new phase, with innovation gradually becoming the central theme. This necessitates that industry professionals shift their mindset, grasp the underlying principles governing medical device R&D, and place greater emphasis on the role of the clinical side in driving medical device innovation. The Five Golden Rules for Medical Device R&D Innovation proposed in this article represent our team’s in-depth synthesis and reflections, offering valuable reference for the industry’s medical device R&D efforts.
Authors: Pan Wenzhi, Shen Li, Ge Junbo
Zhongshan Hospital, Fudan University; National Clinical Research Center for Radiological Diagnosis and Treatment; China Cardiovascular Physicians Innovation Club