Traditional CAR-T cell therapy is complex to prepare and has a complicated administration process.But it has also significantly changed the treatment landscape of multiple myeloma, butIn vivo CAR-T therapy aims to induce the patient's own cells to exert anti-tumor effects directly within the body through a single, simple infusion.Such a concept has made it highly sought after by both pharmaceutical companies and investment institutions.Last year, AstraZenecaAstraZeneca AcquisitionEsoBiotec, pushing in vivo CAR-T to new heights. By 2026,Researchers from Wuhan Tongji HospitalNature MedicineThe latest research published provides a more in-depth analysis of the safety profile of the first in vivo CAR-T product to enter clinical research.This Phase I, single-arm, open-label clinical trial evaluated the safety and tolerability of ESO-T01. ESO-T01 is a nanobody-directed, immune-shielded lentiviral vector encoding a humanized anti-B-cell maturation antigen (BCMA) CAR for the treatment of adult patients with relapsed or refractory multiple myeloma.
ESO-T01 is administered as a single intravenous infusion at a dose of 0.2×10⁹ transducing units, without the need for leukapheresis, ex vivo preparation, or lymphodepleting chemotherapy. A total of five male patients who had previously received multiple lines of treatment were consecutively enrolled (median number of prior treatment lines was 3), with a median follow-up time of 6.0 months. The trial was terminated early in 2025 and did not continue enrolling patients.
The primary endpoint was safety and tolerability, with secondary endpoints including the efficacy, pharmacokinetics, and pharmacodynamic characteristics of ESO-T01.
No dose-limiting toxicity (DLT) was observed during the study period. All patients experienced grade 3 or higher adverse events. Four patients developed cytokine release syndrome (CRS) (three cases were grade 3, and one case was grade 2), which was managed with glucocorticoids.tocilizumabOr supportive treatment is under control.
The most common adverse reactions were transient cytopenia and reversible elevation of liver enzymes, with 2-grade infections occurring in three patients.One patient developed grade 1 immune effector cell-associated neurotoxicity and eventually died from spinal cord compression caused by extramedullary lesions.
Preliminary antimyeloma activity was observed: 4 out of 5 patients achieved objective response, with 3 reaching stringent complete response (sCR); among all evaluable responders (4/4), minimal residual disease (MRD) negativity was achieved by Day 60 (detection sensitivity 10⁻⁵).
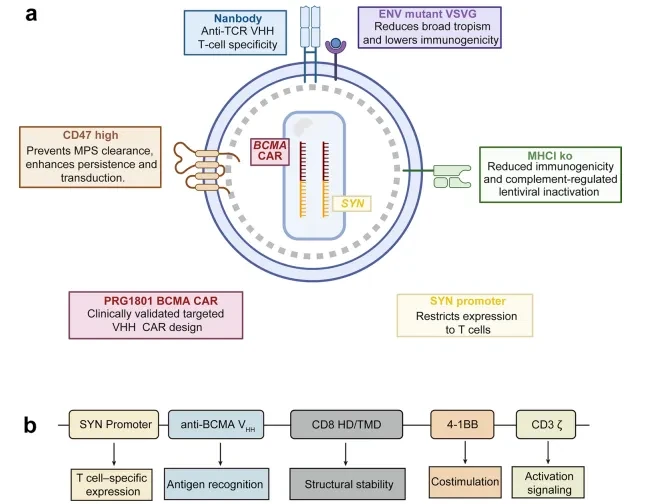
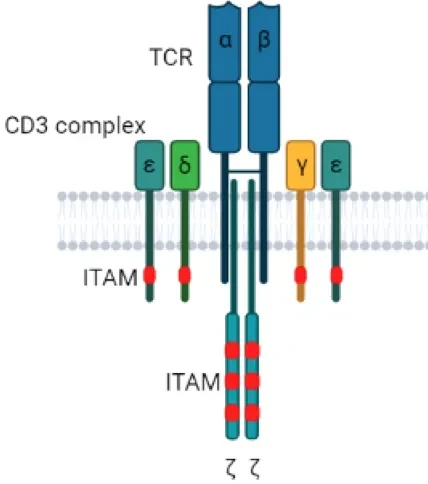
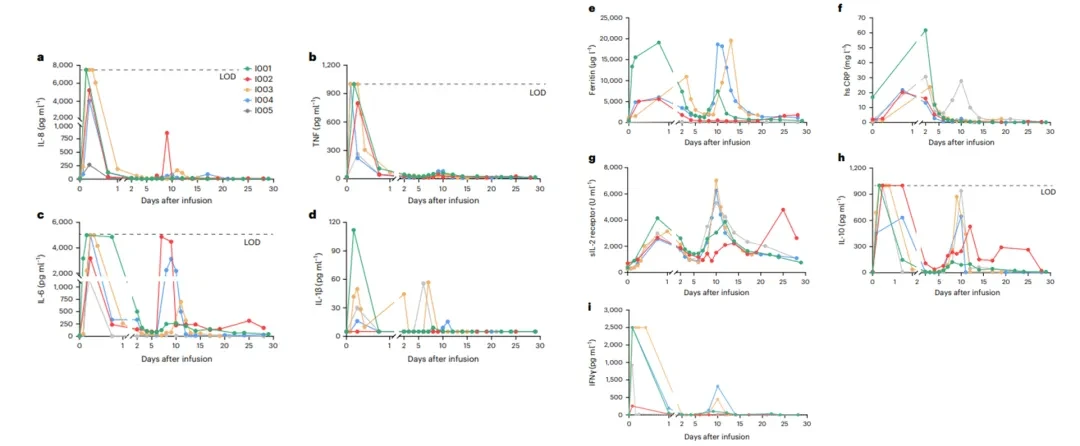
Although in vivo CAR-T therapy may be more accessible than traditional CAR-T therapy, which requires individualized preparation, it also carries significant toxicity risks.As can be seen from the following schematic diagram,EsoBiotecTo prevent phagocytosis and reduce immunogenicity, the vector incorporates the CD47 expression gene and MHCI knockout gene. Nanobodies or scFv are anchored on the surface of the vector to bind target cells, primarily immune cells such as T cells. The conventional CAR structure is also included, allowing the CAR structure to be expressed once bound to immune cells.EsoBiotecPatentWO2025003526A1 used CD3 antibody, CD8 antibody, TCR antibody, and CD14 antibody as targeted T-cell antibodies for a series of validations.ESO-T01 adoptsTCR AntibodyBody.Whether it is a CD3 antibody or a TCR antibody, there is one issue that must be faced: the problem of systemic activation. In other words, whether it’s a CD3 antibody or a TCR antibody, as long as cross-linking-like binding occurs, the downstream signaling pathways will be activated. Lentiviral vectors provide such a suitable carrier (the same applies to other carriers). On such a vector, it is loaded with CD3 antibodies or TCR antibodies, making it an immunological "deep-water bomb."Therefore, the results show that the first supra-acute cytokine surge occurs within 24 hours after infusion, earlier than detectable CAR-T cell expansion, and is temporally associated with the occurrence of early cytokine release syndrome (CRS); followed by a second, lower-amplitude peak between days 6 and 14, consistent with CAR-T cell expansion and low-grade fever.This is a visible surge in cytokines caused by targeted reasons, leading to T-cell activation.This is also a key point that restricts the treatment window of CAR-T therapy in vivo. In terms of methods, preventive medication may be required in advance, and there might even be a need to reduce the dosage. A reduction in dosage will naturally affect the final transfection outcome.After all, good targeted delivery targets are very scarce at present.The preliminary efficacy of CAR-T in the body is evident to all, but this does not mean that it has surpassed current therapies. The current safety issues and persistence problems have become limiting factors.Currently, numerous in vivo CAR-T companies, whether utilizing LNP or lentivirus, have transitioned from mRNA vaccines, traditional CAR-T, or TIL companies. A good drug requires both luck and the test of time.ADC has already proven that it's not about entering the market too early or being the first to succeed, but rather about timing it just right.
Welcome to join my Knowledge Planet, where professional free consultation is available.
The official account has established a real-name discussion WeChat group for readers. You can join the group by adding WeChat (zhuisu2210). When adding, please actively indicate your name, company, and position.