Where Did the Markup Go? Tracing the Reallocation of Margins After the Halving of Drug and Device Add-ons
When the wind blows, the course of the ship must change.
On October 16, 2020, the Joint Procurement Office for National Organization of High-Value Medical Consumables (hereinafter referred to as the “Joint Procurement Office”) issued the *Document on Centralized Volume-Based Procurement of Coronary Stents Organized by the State*. Since then, coronary stents have entered the era of thousand-yuan pricing, leading to a significant contraction in their market size.
Nearly a year after the implementation of centralized procurement, the Joint Procurement Office released relevant documents this September, disclosing the effectiveness of the coronary stent centralized procurement reform since January 2021 from three perspectives: patients, hospitals, and the industry.
The documents show, First, the public has benefited significantly. The prices of coronary stents selected in the centralized procurement have dropped markedly, substantially reducing the financial burden on patients.
Second, physicians’ legitimate income has increased. Provinces that previously had lower fee schedules for coronary stent implantation have raised their charges. Coupled with mechanisms such as the retention of medical insurance payment surpluses and reforms in payment methods, medical staff in relevant departments have seen an increase in legitimate income despite stable workloads, which helps to rationalize the compensation mechanism for public hospitals.
Third, the industrial development environment has been optimized. The volume-based procurement policy has effectively addressed the issue of artificially inflated prices, streamlined distribution channels, improved the business environment, and increased industry concentration, while also leaving sufficient market space for non-selected companies and new market entrants.
What industry development “codes” are hidden within this series of information?
By looking beyond the surface, we can see that squeezing out the moisture from consumables and avoiding overtreatment are, to a certain extent, helping healthcare return to its essence.Supported by evidence-based medicine and scientific and technological advancements, traditional empirical medicine will gradually evolve toward personalization and precision. “Volume-based procurement-immune” segments—such as bioresorbable scaffolds, intravascular imaging, and coronary functional assessment—may become the next growth engine for the industry.
Next, VCBeat will analyze the future development opportunities in cardiovascular and related sectors amid healthcare reform, drawing on relevant policies and information.
As the centralized procurement policy takes effect, slashing profits on medical consumables, pressing questions have emerged as lingering uncertainties surrounding the policy: How will the industry evolve? How can hospitals remain profitable? How can physicians’ motivation be enhanced? Is the supply of stents adequate?
As a key component of healthcare reform policies, the impact of centralized procurement can be examined from three perspectives: patients, hospitals, and the industry.
For the patient population,, with significant price reductions in medical consumables, patients’ financial burdens have been substantially alleviated. According to calculations by Beijing Municipality, the average out-of-pocket expense for patients undergoing stent implantation has decreased by RMB 10,000. Meanwhile, documents released by the National Joint Procurement Office also reveal that many individuals who previously could not afford stents, particularly chromium alloy stents, are now able to access “high-quality and affordable” chromium alloy stents. Behind these figures, we may infer that as prices for medical consumables and pharmaceuticals are reduced and inflated costs eliminated, patients can enjoy better medical services and receive more professional diagnostic care for the same expenditure.
For the medical community,The compression of profit margins on medical consumables has begun to drive hospitals to further adjust their revenue structures and increase physicians’ legitimate income.
In this regard, there are three noteworthy points in the Joint Procurement Office’s description of hospital outcomes:First, provinces that previously had lower surgical fees have raised their fee schedules. Second, mechanisms such as medical insurance payments have been layered on to increase physicians’ legitimate income. Third, the compensation mechanism for public hospitals has been strengthened.
From this, we can see that hospitals are establishing compensation mechanisms and adjusting their revenue structures to maintain a balance in physicians’ income.On one hand, medical insurance has been integrated into the pricing mechanism. On the other hand, hospital revenue structures are shifting from a historical reliance on consumables as the primary income source toward increased revenue from service fees for procedures and diagnostic tests. Following healthcare reforms, medical services that do not involve consumables—such as certain diagnostic examinations and treatments—are poised to become new trends and key directions under policy-driven changes.
In fact, as early as 2016, the “Several Opinions of the Leading Group for Deepening the Reform of the Medical and Health Care System under the State Council on Further Promoting the Experience in Deepening the Reform of the Medical and Health Care System” proposed to actively and steadily advance the reform of medical service pricing. Under the premise of ensuring the sound operation of public hospitals, the affordability of the basic medical insurance fund, and no overall increase in the burden on the public, it called for adjusting price ratios among medical institutions at different levels and for various medical service items through categorized guidance, in accordance with the requirements of aggregate control, structural adjustment, selective increases and decreases, and gradual implementation.
Liang Wannian, former Director of the Department of System Reform under the National Health Commission, has also pointed out this issue.All public hospitals have abolished drug markups. Compensation policies determined by local governments are taken into comprehensive consideration, price adjustments are precisely calculated, and medical service prices are adjusted simultaneously. By standardizing diagnosis and treatment practices, room is created to reduce expenditures on drugs and consumables, thereby enabling dynamic adjustment of medical service prices.
The policy arrived as scheduled. In September this year, the National Healthcare Security Administration and seven other departments jointly issued the Pilot Plan for Deepening the Reform of Medical Service Prices (hereinafter referred to as the “Pilot Plan”), while selecting five pilot cities to adjust medical service prices across five dimensions: the total volume control mechanism, the price classification formation mechanism, the dynamic price adjustment mechanism, the price item management mechanism, and the price monitoring and assessment mechanism.
A relevant official from the National Healthcare Security Administration stated:“The primary objective of volume-based procurement is to eliminate inefficiencies in the distribution chain and curb kickback-driven sales, rather than to justify price increases for medical services. Only when drug and consumable prices are reduced can the conditions be created for reforming medical service pricing. We encourage healthcare providers to focus more on increasing the volume of technically complex surgeries, thereby enhancing their income. This approach guides public hospitals to strengthen their core competencies, avoiding an ‘arms race,’ blind expansion, and excessively premature advancement.”
Overall, healthcare reform has entered a critical phase centered on the restructuring of medical service pricing. As the inflated costs of pharmaceuticals and consumables are squeezed out post-reform, the key to determining the success of healthcare reform lies in addressing the resulting income gap for physicians and shifting from scale-driven expansion to quality improvement and efficiency enhancement.
For enterprises,Post-VBP, industrial concentration has increased. Leading enterprises, leveraging advantages such as comprehensive product portfolios and ecosystem systems, are better positioned to seize early-mover opportunities in the VBP market. However, the “large ship is hard to turn” dilemma means that leading companies lag behind startups in innovation capacity and error tolerance within single product lines. This leaves certain market opportunities for non-selected incumbents and new market entrants.As mainstream surgical devices such as coronary stents are subject to strict regulatory control, segments exempt from centralized procurement—such as drug-coated balloons, bioresorbable scaffolds, intravascular imaging, and coronary functional assessment—may emerge as the next growth engine for the industry.
In this regard, the Pilot Program also points out that if a technology-enabled medical service can effectively optimize diagnosis and treatment protocols for major diseases or fill gaps in diagnostic and therapeutic capabilities, regulatory authorities will open a fast-track channel for the relevant technology to facilitate its early inclusion in the price catalog.
It is evident that as the winds of healthcare reform sweep through, patients, hospitals, and enterprises alike are shifting course toward “quality” and “precision.”Patients will seek more precise and reliable treatments. Hospitals, in turn, will shift their revenue focus to medical services by enhancing physicians’ clinical expertise to better meet patient needs while increasing their “transparent income.”In the cardiovascular sector, as industry consolidation intensifies, precision diagnosis and treatment modalities—such as consumables innovation, intravascular imaging, and coronary functional assessment—will emerge as new strategic growth drivers for enterprises.
From a long-term perspective, healthcare service price reforms are driving a shift in the focus of clinical diagnosis and treatment.
Historically, the focus of healthcare was on ensuring affordability for patients. Today, with the improvement of medical systems and industry development, the value of “medical services,” long undervalued and squeezed by pharmaceuticals and medical devices, is gradually coming to the fore and returning to its proper track. On one hand, regulators under the new system aim to establish a prevention-oriented diagnostic service model to minimize subsequent surgical interventions. On the other hand, rising socioeconomic status and health literacy are fostering patient awareness of “preventive care” or “treating potential diseases before they manifest.”
An industry insider discussed this trend, stating:“The ultimate objective of the state’s push to realign medical service prices with their intrinsic value may not be singular. On one hand, the high premiums on pharmaceuticals and medical devices have incentivized physicians to overprescribe them, causing harm to both the health insurance system and patients; establishing a rational pricing mechanism for medical services will reshape the incentive structures for doctors and hospitals, enabling physicians to benefit from delivering high-quality care. On the other hand, in line with the broader trend toward early diagnosis and screening, the state favors upgrading diagnostic capabilities to intervene as early as possible in the disease course, substituting invasive surgical treatments at later stages with non-invasive tests and pharmacological therapies, thereby fundamentally reducing the high costs associated with surgery.”
Coronary consumable prices have been slashed, significantly reducing the profits doctors derive from them and dampening their motivation. The current policy aims to eliminate the negative impacts of centralized procurement by increasing fees for related medical services provided by physicians, such as preoperative diagnosis and surgical procedures.
It is conceivable that if patients with coronary heart disease undergo preoperative examinations using methods such as CT-FFR, and the results are normal, coronary angiography would not be necessary. In the past, forgoing angiography represented a financial loss for hospitals. However, with the intensified implementation of policies such as Diagnosis-Related Groups (DRG) and medical service reforms, services like CT-FFR can not only serve as a legitimate incentive mechanism for physicians but also enable patients to receive more precise diagnostic and therapeutic services at the same cost.
The same approach can also be applied in fields such as imaging diagnostics and liquid biopsy.Both healthcare reform policies and technological advancements are, to a certain extent, driving the transformation of traditional medical paradigms toward the goals of “minimizing iatrogenic harm” and “maximizing health benefits.” This direction will significantly enhance the accuracy and controllability of disease prevention, diagnosis, and treatment within medical processes.
Fractional Flow Reserve (FFR), as a novel diagnostic modality, represents a significant application for enhancing the precision of diagnosis and treatment.
Why Is FFR an Example of Policy Benefits Favoring MedTech? This Starts with the Core Function of FFR.
In the field of cardiovascular imaging diagnosis, coronary CT angiography can only assess the anatomical severity of coronary artery stenosis and cannot accurately determine whether such stenosis causes corresponding myocardial ischemia. In contrast, fractional flow reserve (FFR) enables functional assessment of the coronary arteries, evaluating from a physiological perspective whether the degree of stenosis induces myocardial ischemia. This further assists physicians in making diagnoses, reduces unnecessary coronary angiography procedures, and helps patients save on medical expenses.
On the one hand, this diagnostic approach enables functional assessment of patients solely through non-invasive imaging, thereby avoiding unnecessary contrast procedures and effectively reducing patients’ unwarranted medical expenses, thus embodying the value of “returning to the essence of healthcare.” On the other hand, FFR represents a new strategy for pharmaceutical and medical device companies to enter hospitals. Specifically, it streamlines existing diagnostic and treatment workflows in a more efficient and cost-effective manner, achieving improvements in medical efficiency and outcomes while reducing healthcare expenditures. Such innovative products can rapidly gain recognition from hospitals.
Currently, FFR measurement has received the highest Class IA recommendation in the "2014 ESC/EACTS Guidelines on Myocardial Revascularization" and the "Chinese Guidelines for Percutaneous Coronary Intervention (2016)."
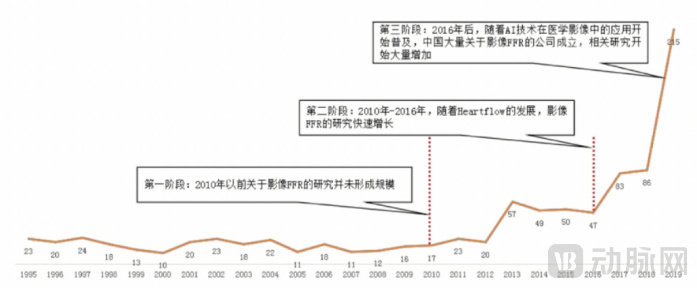
Annual Global Publication Volume of Imaging-Based FFR Papers. Data Source: PubMed
With the widespread adoption of AI technology in medical imaging, academic research on this topic has shown a year-on-year upward trend.
Since 2016, a large number of enterprises have recognized the feasibility of this approach, leading to the establishment of numerous domestic companies focused on image-based fractional flow reserve (FFR). Key system developers and manufacturers include Keya Medical, PulseMed Technology, Pulstec Technology, Heart Century, Shukun Technology, and Northcore Life.

Overview of Products from Domestic Imaging FFR Companies
Note: Only a partial list of companies is provided; the order does not imply ranking.
While there is slight overlap in product portfolios among various companies, their specific focal points and strategies are distinct. Each company continues to explore precise diagnostic methods for cardiovascular diseases from different perspectives, resulting in a diverse range of products that enhance the accuracy and efficiency of medical diagnostics across multiple dimensions.
For instance, Keya Medical leverages AI to rapidly assess the severity of coronary artery stenosis, thereby reducing unnecessary invasive coronary angiography procedures and subsequent percutaneous coronary intervention (PCI) treatments; Pulse Medical has established a presence in the fields of coronary physiology and imaging, gradually expanding into neurointerventional, peripheral interventional, and electrophysiology domains to cover the complete industry chain for precise diagnosis in pan-vascular interventions; FlowMed Technology has developed three major product lines centered on cardiovascular and cerebrovascular diseases: cardiovascular disease solutions, cerebrovascular disease solutions, and the FlowMed Cloud Platform; LifeCore Biomedical possesses a portfolio of products for both precise intravascular physiology and imaging.
As the industry undergoes a transition, an analysis of the imaging FFR industry map reveals that the direction of increased investment in medical services may have shifted toward tracks such as consumables innovation, intravascular imaging, and coronary functional assessment.
In the face of industry changes, overseas leading enterprises and innovative companies have different strategies.
Large corporations possess stable ecosystems and established commercial channels. First, their business layouts are more comprehensive, with better-controlled costs. Second, their core strengths lie not in individual products but in their proprietary resources and product ecosystems. Leveraging these two advantages, large companies can provide clients with end-to-end solutions, thereby building sustainable corporate development capabilities. However, large corporations lag behind emerging imaging enterprises in terms of innovation capacity and risk tolerance within single product lines. This gap consequently creates room for innovative companies to grow.
For innovative companies, achieving product innovation and breakthroughs is the key to success. Currently, the companies that are moving quickly in this sector have almost all relied on making breakthroughs in a single product or several products to rapidly enter the market.
Keya Medical submitted its prospectus to the Hong Kong Stock Exchange in March this year, aiming to become the first listed AI medical device company with its “DeepVessel FFR.” NorthLife Medical, leveraging its unique position as the sole company with a portfolio combining precise intravascular physiology and imaging products, filed its draft prospectus with the Hong Kong Stock Exchange in August this year.
Homogenization of innovation is bound to undergo a new round of reshuffling in the future. The cases of Keya Medical and Northlife Medical both demonstrate that breaking away from homogenization, establishing proprietary technological barriers, and transitioning from “domestic substitution” to “domestic surpassing” are the keys for innovative enterprises to achieve overtaking on a bend.
However, both large enterprises and innovative startups have their respective strengths and weaknesses. Collaborative efforts between innovative startups and industry leaders to drive product innovation represent a viable development pathway. Large companies offer established ecosystems, while innovative firms contribute specialized products and technologies—a synergy that benefits both the industry and society as a whole.
It is reported that Pulsar Vascular has established collaborations with Shanghai Jiao Tong University, the National Center for Cardiovascular Diseases, Fuwai Hospital of the Chinese Academy of Medical Sciences, the National Clinical Research Center for Radiology and Therapy, and Zhongshan Hospital Affiliated to Fudan University, among others, to accelerate the implementation and widespread adoption of QFR series technologies—original innovations from China—in hospitals at all levels. Additionally, the company has entered into strategic partnerships with multiple international medical device giants, including Philips and Medtronic, to further deepen its commercial footprint both domestically and globally.
In this regard, industry experts have suggested that the future of the sector should focus on innovation, the transition from minimally invasive to non-invasive procedures, complex cases, and clinical challenges that are difficult to address with conventional therapies. The goal is to develop products that are genuinely embraced by physicians and widely adopted in clinical practice. To achieve this, companies must remain attuned to clinical needs while simultaneously building robust evidence-based medicine barriers for their products.
Following the implementation of centralized volume-based procurement (VBP), companies across sectors such as high-value medical consumables, medical imaging, and liquid biopsy—whether industry leaders or innovative startups—must adjust their strategies in alignment with their core competencies to keep pace with evolving trends and seize opportunities amidst challenges. Clearly, VBP is not intended to eliminate the industry but rather to drive innovation. Professionals within affected enterprises can shift focus upstream to enhance the precision of medical diagnostic processes, though innovation remains imperative. As domestic substitution of consumables advances and supporting services rise, guided by policy, the market is poised for expansion.