Biotech Breakthroughs Restore Hearing: From Cochlear Implants to Gene Therapy
Editor’s Note: This article is republished from Hillhouse Capital, with authorization granted to VCBeat.
International Deaf Day falls on the fourth Sunday of September each year. According to the results of the Second National Sample Survey on Persons with Disabilities, there are approximately 27.8 million people with hearing disabilities in China, accounting for more than 30% of the total disabled population. As a hearing restoration device, cochlear implants can effectively improve hearing levels in individuals with severe hearing loss for whom hearing aids are ineffective or provide minimal benefit.
Broadly defined, deafness is a collective term for hearing loss of varying degrees. In today's society,Hearing Loss Is Becoming a Serious Public Health Issue. A 2011 study of the Beaver Dam cohort in the United States found that the prevalence of hearing loss steadily increases with age, affecting more than 80% of individuals over 80 years old. Based on etiology, deafness can be classified into hereditary and non-hereditary types; based on the time of onset, it can be divided into congenital and acquired deafness; and based on pathogenesis, it can be categorized as conductive, sensorineural, or mixed deafness.
Deafness can have a severe impact on physical and mental health,causing a series of serious complications, including but not limited to dementia, social isolation, and depressionIn The Lancet’s reports on dementia published in 2017 and 2020, hearing loss was consistently identified as the most significant potential risk factor for dementia (Figure 1). Small-scale meta-analyses have also suggested that hearing interventions can alleviate social isolation and loneliness among older adults. Therefore, improving patients’ hearing and mitigating cognitive impairment associated with hearing loss hold substantial and urgent clinical value.
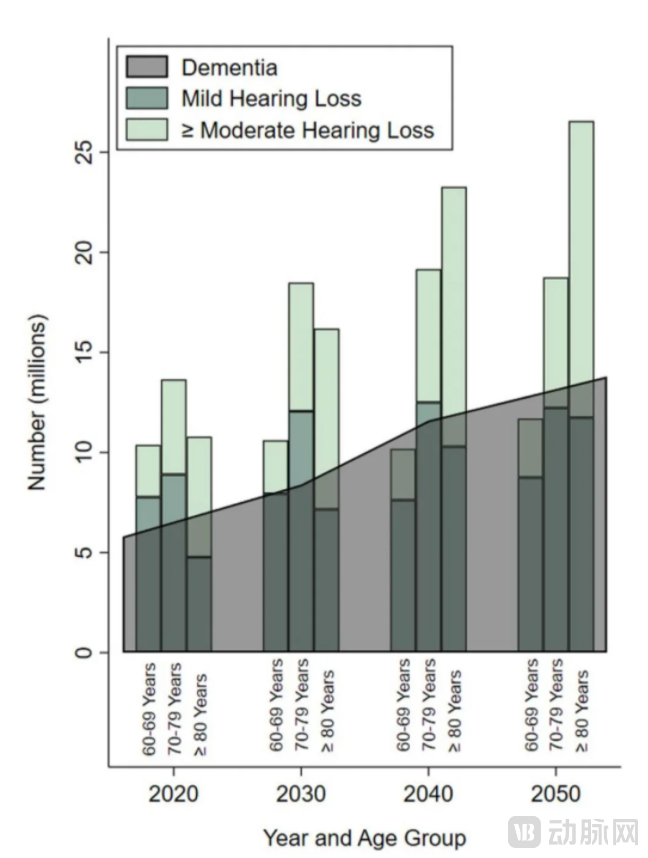
Figure 1. Estimates and Projections of Hearing Loss and Dementia Incidence Among the Older Adult Population in the United States, 2020–2050
For individuals with hearing loss, the use of hearing amplification devices is the primary intervention. Generally, amplification devices may be considered when hearing loss of ≥10 dB is measured at two to three frequencies and the hearing impairment affects daily living.
Hearing aids primarily consist of a microphone, amplifier, receiver, and battery. The microphone captures external sound signals and converts them into electrical signals, which are then amplified by the amplifier. The receiver accepts the amplified electrical signals and converts them back into acoustic signals, which are projected into the ear canal.
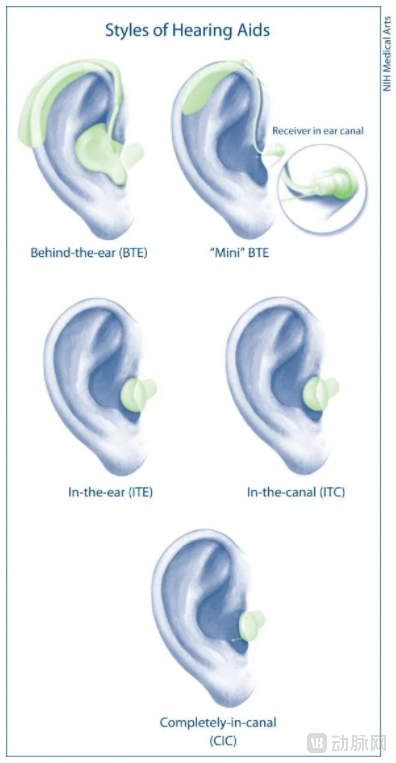
Figure 2 Different Types of Hearing Aids
Behind-the-Ear (BTE) Hearing Aids
Behind-the-ear (BTE) hearing aids are relatively large in size and sit behind the ear. Equipped with ample power supply and powerful amplification circuits, they are suitable for various degrees of hearing loss and offer advantages such as high efficiency, affordability, and ease of use. Patients with moderate to profound hearing loss may require closed-fit earmolds when using BTE hearing devices. These earmolds help block external noise and prevent acoustic feedback by stopping amplified sound from being picked up again by the microphone; however, this may compromise cosmetic appearance.
Mini Behind-the-Ear Hearing Aid (“Mini” BTE)
Mini behind-the-ear (BTE) hearing aids position the receiver within the ear canal, connected to the main body by a wire, reducing their size to half that of traditional BTE devices. This Receiver-in-the-Canal (RIC) technology significantly enhances loudness while effectively controlling acoustic feedback. It offers comfortable wear and avoids low-frequency attenuation caused by the "occlusion effect," making it highly suitable for elderly patients with presbycusis characterized primarily by high-frequency hearing loss. However, the open ear canal design combined with high-power gain makes patients more susceptible to environmental noise, and its installation is less convenient than that of traditional BTE hearing aids.
In-the-ear (ITE), in-the-canal (ITC), and completely-in-canal (CIC) hearing aids
These three types of hearing aids operate on similar principles but differ in their depth of insertion into the ear canal (Figure 3). The main body of an in-the-ear (ITE) hearing aid is located in the outer ear, making it suitable for moderate to severe hearing loss. Its drawbacks include being relatively visible and failing to utilize the sound-collecting function of the outer ear and pinna. An in-the-canal (ITC) hearing aid protrudes from the outer ear on only one side, offering greater discretion and leveraging most of the pinna’s sound-collecting capability; however, it is prone to displacement and relatively difficult to fit.
Completely-in-canal (CIC) hearing aids are entirely concealed within the ear canal and are not visible from the outside. Because the receiver is positioned close to the tympanic membrane, they require a lower level of amplification. However, they are the most difficult to fit, are most prone to being lost, and managing acoustic feedback presents a significant technical challenge for this type of device. The common advantage of the three aforementioned hearing aid styles is their discreet appearance. Nevertheless, due to their small size, the functionality of the battery and amplification circuitry is inevitably constrained, resulting in limited sound amplification performance.

Figure 3 In-the-ear (ITE), in-the-canal (ITC), and completely-in-canal (CIC) hearing aids
CROS/BiCROS Signal Transmission Circuits (Unilateral/Bilateral)
Cross-Over Hearing Aid SystemsCross-over hearing aid systems are a specialized amplification principle designed for unilateral or asymmetric hearing loss. In this configuration, the microphone is placed on the ear with poorer hearing, but the signal is transmitted to and amplified in the contralateral (better-hearing) ear to leverage its superior auditory function. Due to certain drawbacks associated with this approach—such as significant impairment in sound source localization and speech recognition in noisy environments—its clinical use has declined considerably.
Due to the limited amplification efficiency of non-implantable hearing aids, especially their limited ability to amplify high frequencies,Patients with severe to profound hearing loss may require the use of implantable hearing devices.
Bone Conduction Hearing Aid Device
Bone conduction hearing devices consist of an implant, an abutment, and a processor (Figure 4). The implant is surgically placed in the temporal bone on the affected side and connects to an external processor via either a percutaneous abutment or a transcutaneous magnet. The processor converts acoustic signals into electrical signals, causing the implant and temporal bone to vibrate. These vibrations are transmitted directly to the inner ear, enabling the patient to perceive sound. Currently, commercially available bone conduction hearing devices mainly include Ponto (Oticon) and BAHA (Cochlear). In addition, some novel non-implantable devices, such as the softband BAHA and Adhear (MED-EL), induce temporal bone vibration without requiring surgical implantation; these new technologies are being increasingly adopted and promoted.
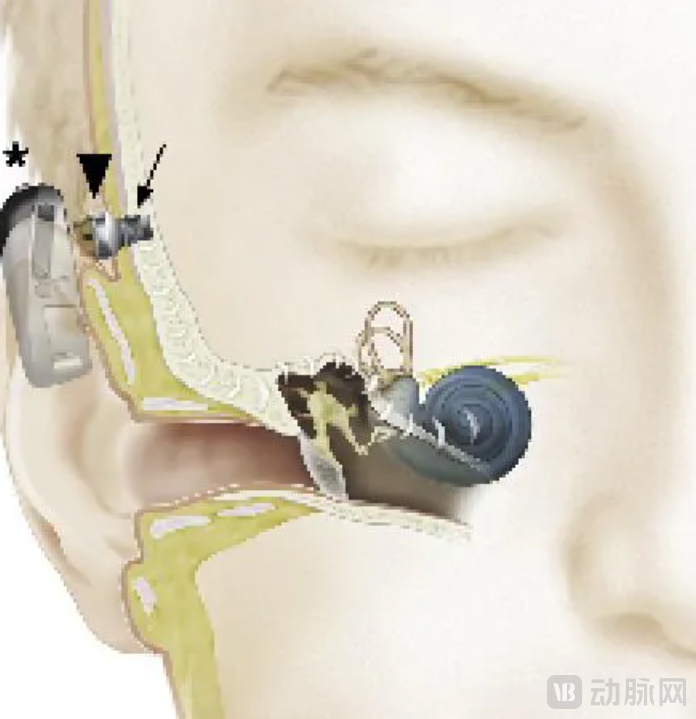
Figure 4. Schematic diagram of the components of a bone conduction hearing aid device
Middle Ear ImplantsMiddle ear implants achieve efficient auditory gain by directly stimulating the ossicles or the round window membrane. Currently, widely used middle ear implant systems include the Vibrant SoundBridge (MED-EL), MAXUM (Ototronix), and Esteem (Envoy Medical). Taking the Vibrant SoundBridge as an example, the system consists of an implanted component and a wearable external component. The implanted component comprises a receiving coil, magnet, demodulator, connecting leads, and a Floating Mass Transducer (FMT); the external component consists of a microphone, audio processor, battery, transmitting coil, and fixing magnet. The FMT can stimulate various middle ear structures, including the round window membrane and the individual ossicles, to achieve sound amplification (Figure 5).
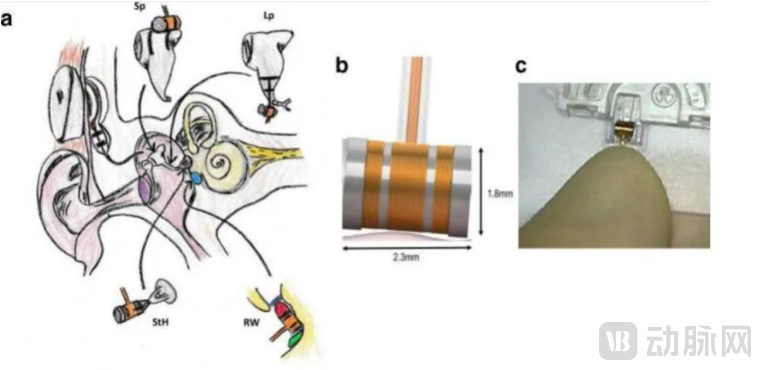
Figure 5 Illustration of the Vibrant Soundbridge Principle
a) Implant stimulating different locations in the middle ear; b) Schematic diagram of the floating mass transducer; c) Photograph of the floating mass transducer
Cochlear Implant (CI)
For some patients with severe sensorineural hearing loss (e.g., cochlear maldevelopment, hair cell dysfunction, etc.), humanCochlear implantation can lead to improvements in multiple areas, including hearing thresholds, speech development, and environmental awareness.
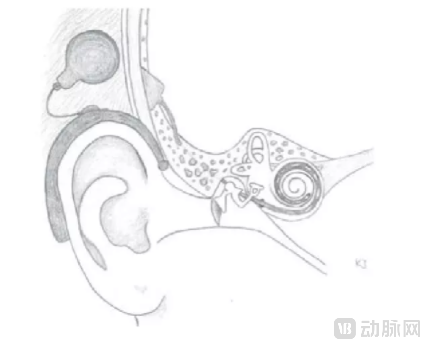
Cochlear Implant: An electronic device that converts sound into electrical signals to restore or reconstruct auditory function in deaf individuals by stimulating the auditory nerve.A cochlear implant consists of an external processor, a transmission coil, a subcutaneous receiver, and an implanted electrode array (Figure 6). The external processor converts acoustic signals into electrical signals, which are transmitted to the subcutaneous receiver. The implanted electrode array, whose frequencies basically match the intrinsic frequencies of the cochlea, then directly delivers electrical stimuli to the spiral ganglion, thereby eliciting hearing.
Currently, cochlear implants have evolved into various types, including different numbers of electrode arrays, standard/soft electrodes, straight/pre-curved electrodes, half-band/full-band electrodes, full-coverage/short electrodes, monopolar/multipolar configurations, and diverse speech processing strategies. However, there remains a significant gap in cochlear implantation in China. As early as 2006, more than 500,000 hearing-impaired minors in China met the criteria for cochlear implantation, including 100,000 children under the age of six. Yet, by 2013, only over 30,000 patients nationwide, including adults, had received cochlear implants (85% of whom were children).
The high cost of equipment remains the greatest barrier to treatment for many patients. For a long time, the cochlear implant market has been monopolized by three foreign companies. Notably, several domestically produced cochlear implants have entered the market and demonstrated efficacy through clinical trials, such as Nurotron’s Morning Star Cochlear Implant System developed by Zhejiang Nurotron Biotechnology Co., Ltd. This system received approval from the China Food and Drug Administration (CFDA) in 2011 and obtained the European Union CE certification in 2012. In 2021, Tencent’s Tianlai AI Lab and Nurotron jointly launched a combined solution featuring “cochlear implants + mobile phone companions,” which improved speech clarity and intelligibility for cochlear implant users by 40%.
Auditory Brainstem Implantation (ABI)
For patients with retrocochlear lesions or those whose cochlear conditions preclude cochlear implantation, auditory brainstem implantation may be considered. The composition of the auditory brainstem implant is similar to that of a cochlear implant (Figure 7). The difference is that the auditory brainstem implant is directly attached to the cochlear nucleus of the patient’s brainstem, bypassing peripheral conduction via the auditory nerve and directly eliciting auditory perception.

Figure 7. Composition of the Auditory Brainstem Implant Device
A) External device; B) Internal device; C) Electrode array board
With technological advancements, hearing aids are subtly transforming people’s lives. Individuals using these devices are increasingly active across various professions, including police officers, military personnel, pilots, athletes, and musicians. In the future, hearing aids will undoubtedly evolve toward greater comfort and more realistic auditory simulation, marking a transition from disability treatment to human enhancement tools.
* Content reviewed by PUMC Eight
# Reference Materials:
1. Nash, S.D., et al., The prevalence of hearing impairment and associated risk factors: the Beaver Dam Offspring Study. Arch Otolaryngol Head Neck Surg, 2011. 137(5): p. 432-9.2. Goman, A.M. and F.R. Lin, Prevalence of Hearing Loss by Severity in the United States. Am J Public Health, 2016. 106(10): p. 1820-2.
3. Powell, D.S., et al., Hearing Impairment and Cognition in an Aging World. J Assoc Res Otolaryngol, 2021.
4. Ellis, S., S. Sheik Ali, and W. Ahmed, A review of the impact of hearing interventions on social isolation and loneliness in older people with hearing loss. Eur Arch Otorhinolaryngol, 2021.
5. Schuster-Bruce, J. and E. Gosnell, Conventional Hearing Aid Indications And Selection, in StatPearls. 2021, StatPearls Publishing
Copyright © 2021, StatPearls Publishing LLC.: Treasure Island (FL).
6. Fagan, J.J., Open Access Publishing of Textbooks and Guidelines for Otolaryngologists in Developing Countries. OTO Open, 2019. 3(3): p. 2473974x19861567.
7. Atcherson, S.R., et al., Hearing Loss: Hearing Augmentation. FP Essent, 2015. 434: p. 18-23.
8. Ghossaini, S.N. and P.C. Roehm, Osseointegrated Auditory Devices: Bone-Anchored Hearing Aid and PONTO. Otolaryngol Clin North Am, 2019. 52(2): p. 243-251.
9. Banakis Hartl, R.M. and H.A. Jenkins, Implantable Hearing Aids: Where are we in 2020? Laryngoscope Investig Otolaryngol, 2020. 5(6): p. 1184-1191.
10. Burd, C., I. Pai, and S.E. Connor, Active middle ear implantation: imaging in the pre-operative planning and post-operative assessment of the Vibrant Soundbridge(TM). Br J Radiol, 2020. 93(1109): p. 20190741.
11. Entwisle, L.K., S.E. Warren, and J.J. Messersmith, Cochlear Implantation for Children and Adults with Severe-to-Profound Hearing Loss. Seminars in hearing, 2018. 39(4): p. 390-404.
12. Dazert, S., et al., Cochlear Implantation. Dtsch Arztebl Int, 2020. 117(41): p. 690-700.
13. Li, J.N., et al., The Advances in Hearing Rehabilitation and Cochlear Implants in China. Ear Hear, 2017. 38(6): p. 647-652.
14. Zeng, F.G., et al., Development and evaluation of the Nurotron 26-electrode cochlear implant system. Hear Res, 2015. 322: p. 188-99.
15. Simpson, A.N., et al., Time From Hearing Aid Candidacy to Hearing Aid Adoption: A Longitudinal Cohort Study. Ear Hear, 2019. 40(3): p. 468-476.