Deking Medical's DKutting® LL Scoring Balloon for Diabetic Foot: A Case Series by Professor Zhang Lei's Team

DK Medtech
Vascular Interventional Balloon Product Developer

DKutting®LL continues to use DK Medtech's unique triangular nitinol coil patent technology, combined with the actual clinical needs of lower limb arteries, significantly increasing the length of the scoring element (up to 150mm). It also developed a new fully coaxial balloon delivery system compatible with 0.014"/0.018" guidewires and enriched the selection of balloon diameters at 0.5mm intervals.
DK Medtech's exclusive directional scoring balloon boasts comprehensive performance with robust radial expansion and flexible axial bending. Its clinical performance has been widely recognized in both the coronary and hemodialysis access fields. The latest development is the DKutting.®LL Scoring Balloon is specifically designed for lower limb arterial intervention, demonstrating significant clinical advantages in directional dilation mechanisms and setting a new standard for peripheral vascular pre-dilation.
DK Medtech Special Release[Professor Zhang Lei's Team: DKutting®Application of LL in Diabetic Foot: Case Presentation, demonstrating the meticulous operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized intraoperative procedures and technical applications, complication prevention, perioperative management, and other aspects, the aim is to promote the standardization of diagnosis and treatment for vascular stenosis and occlusive diseases, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for future diagnosis and treatment, benefiting more clinical patients.
Patient Information
Basic Information:Male, 75 years old.
Chief Complaint:Admitted to the outpatient department on 2025-12-04 at 12:09 due to "intermittent claudication in both lower limbs for 7 months and ulceration of the right foot toes for 6 months."
History of Present Illness:Seven months ago, the patient developed intermittent claudication in both lower limbs without obvious cause, with a walking distance of approximately 200 meters. The patient visited a local tertiary hospital and received conservative treatment with hypoglycemic, lipid-lowering, and antiplatelet medications, after which the condition improved and the patient was discharged. Six months ago, while trimming toenails, the patient developed an ulcer on the right first toe, followed by localized increased skin temperature, suppuration of the right first toe accompanied by redness, swelling, and pain. The patient reported restricted walking and intermittent claudication. After applying disinfectants such as povidone-iodine independently, the ulcer improved compared to before. One month ago, the patient noticed that the pain in the right foot had worsened compared to before, especially at night, making walking impossible. The ulceration of the first toe bed worsened, accompanied by purplish discoloration and swelling of the third toe. The patient now seeks further diagnosis and treatment. The outpatient department admitted the patient with diagnoses of "Type 2 Diabetic Foot and Lower Extremity Arteriosclerosis Obliterans."
Past Medical History:Generally in poor health, with a 10-year history of diabetes. Denies history of viral hepatitis, hypertension, heart disease, psychiatric disorders, endemic diseases, or occupational diseases. Underwent surgery for varicose veins in the right lower limb over 10 years ago. Denies history of trauma or blood transfusion. Allergy history: none. Vaccination history: unclear.
Physical Examination:Cyanosis of the skin was observed at the tips of the toes on the right foot. The toenails of the right foot were yellowish with thickening. A wound measuring approximately 0.2cm × 0.3cm was present on the lateral side of the tip of the first toe of the right foot. No redness or swelling was noted around the ulcer, and the skin temperature was normal. No bone exposure was detected, and the proximal metatarsophalangeal joint was not involved. A foul odor was noted. The third toe of the right foot appeared cyanotic and purplish without ulceration. The skin temperature of the right lower limb significantly decreased below the knee joint. Arterial palpation: bilateral femoral artery pulses were palpable, while the popliteal artery, dorsalis pedis artery, and posterior tibial artery pulses were not palpable bilaterally.
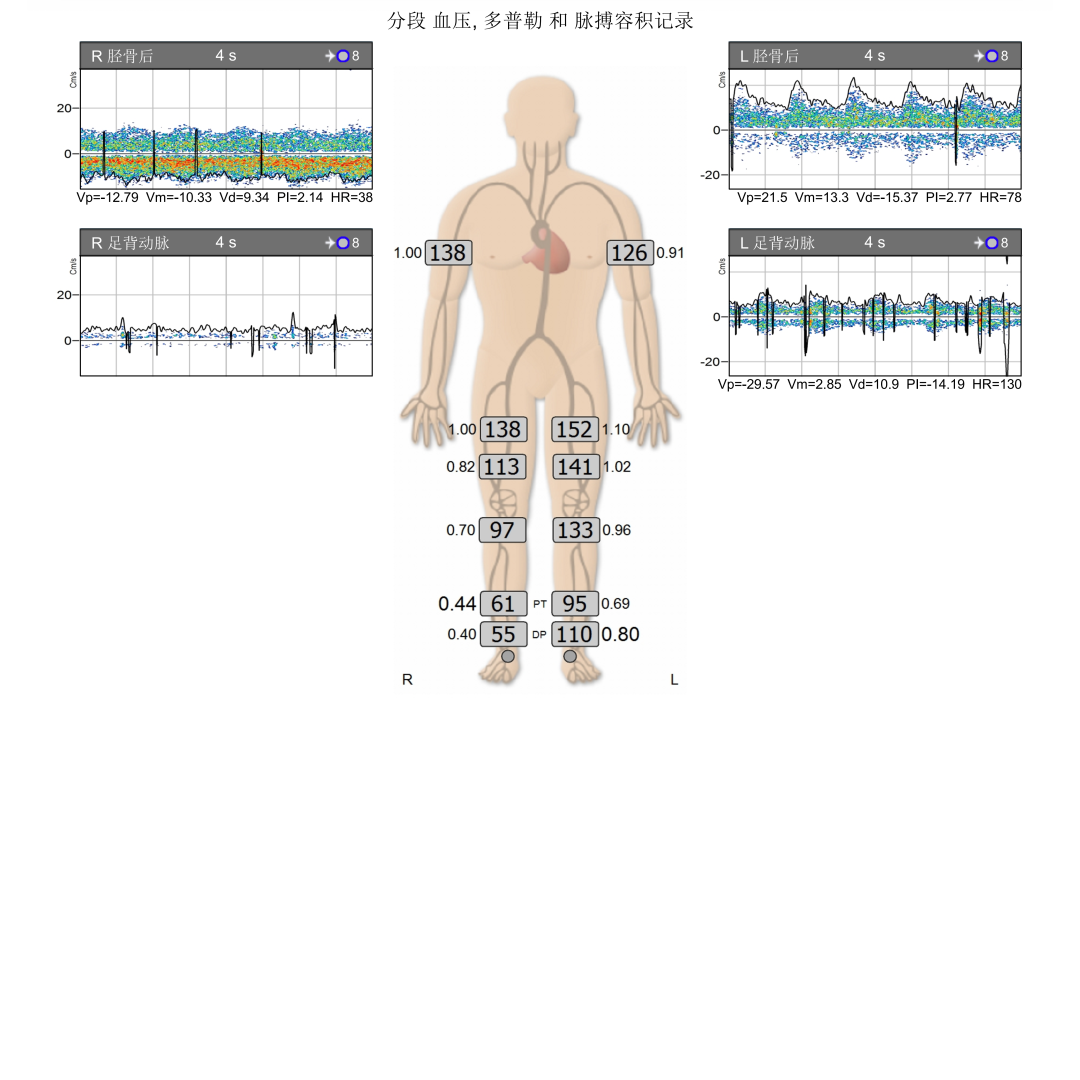
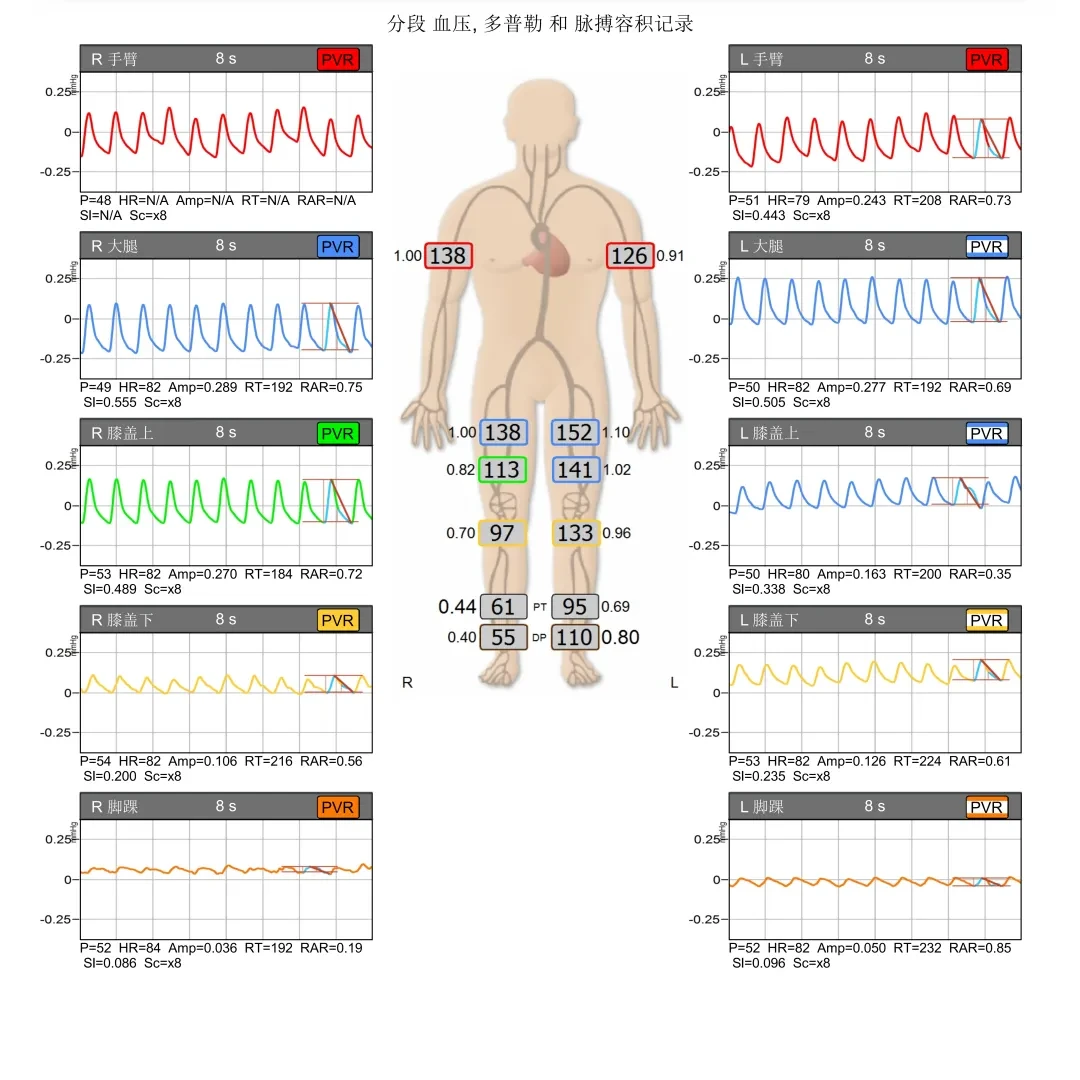
Preoperative Examination:Short segment occlusion of the right popliteal artery P1 segment; Occlusion of the right anterior tibial artery; Stenosis and occlusion of the proximal posterior tibial artery.
Right ABI 0.4, Severe Ischemia.
Admission Diagnosis:
Type 2 Diabetic Foot;
Lower Extremity Arteriosclerosis Obliterans;
Soft tissue infection of the right foot;
Intermittent Claudication;
Type 2 Diabetes Mellitus with Multiple Complications;
Type 2 Diabetic Nephropathy;
Type 2 Diabetic Peripheral Vascular Disease;
Type 2 Diabetic Peripheral Neuropathy.
Previous interventional treatment
No history of previous interventional surgery.
Preoperative Analysis
Preoperative Analysis:
With sufficient antegrade distance, adopt the right common femoral artery antegrade puncture approach to open the popliteal artery, avoiding dissection and residual stenosis.
Patients with diabetic foot toe ulcers need to establish straight-line blood flow in the arteries below the knee directly to the wound.
Surgical Objective:
Main Objectives:Open the popliteal artery, avoid flow-limiting dissection, and reduce stent implantation rate;
Secondary Objectives:Restoration of Blood Supply to the Wound by Opening the Infrapopliteal Artery.
Surgical Plan:Right Popliteal Artery Balloon Angioplasty + Tibial Artery Balloon Angioplasty.
Surgical Procedure

After local anesthesia, the right common femoral artery was punctured antegrade, and a vascular sheath was inserted. Angiography showed: the right common femoral artery, deep femoral artery, and superficial femoral artery were well visualized; segmental stenosis and occlusion in the P1 segment of the popliteal artery; no visualization of the main trunk of the anterior tibial artery; segmental severe stenosis at the origin of the posterior tibial artery, with the rest of the main trunk visualized satisfactorily; mild segmental stenosis of the peroneal artery, with acceptable visualization.
Import the VER catheter and molly guidewire, advance to the distal segment of the femoral artery, switch to a V-18 guidewire, and use roadmap technology. Carefully pass through the occluded lesion with the cooperation of the guidewire and catheter until reaching the P3 segment of the popliteal artery. Apply roadmap technology to super-select the posterior tibial artery below the knee, continuing until the distal segment of the posterior tibial artery. Retain the guidewire and introduce.DKutting®LL Scoring Balloon 4*150mmBalloon dilation was performed on the popliteal artery lesion segment, and subsequent angiography showed good results with no significant residual stenosis, providing adequate vascular preparation for the subsequent use of drug-coated balloons.

Import drug-coated balloon (4*150mm) to dilate the original lesion segment.

A balloon (2.5*150mm) was positioned at the proximal segment of the posterior tibial artery for balloon dilation. Then, a drug-coated balloon (2.5*150mm) was used for post-dilation.
Final angiography: The right common femoral artery, superficial femoral artery, popliteal artery, tibioperoneal trunk, posterior tibial artery, and peroneal artery showed good visibility with acceptable blood flow velocity.
After the surgery, a plug was used to compress the puncture site of the right femoral artery, followed by sterile bandage compression dressing. The patient was safely returned to the ward.
Follow-up
Condition of the affected foot:

Before Surgery on December 7, 2025

December 14, 2025, post-surgery

March 10, 2026, 3 months post-operation
Case Summary
Case Characteristics:Short segment occlusion of the popliteal artery; Infrapopliteal arterial disease.
Preoperative Assessment Key Points:Antegrade Femoral Artery Puncture, True Lumen Passage Through the Occluded Popliteal Artery Segment, Avoiding Flow-Limiting Dissection and Residual Stenosis.
Surgical Strategy/Technical Key Points:Make every effort to achieve true lumen opening, slowly expand with a directional scoring balloon, and avoid the formation of flow-limiting dissections, creating favorable conditions for adopting the "intervention without implantation" strategy in the taboo area of cross-joint stents.
Characteristics/Usage Tips of the Device:DKutting®LL Scoring BalloonUpon reaching the lesion site, first inflate to 3atm and maintain for at least 30 seconds to ensure minimal shear force during balloon expansion. Then, expand the balloon to the nominal pressure of 10atm and maintain for at least 120 seconds; observe residual stenosis, and if necessary, increase to 14atm. The 120° directionally distributed scoring elements fully open the lesion while minimizing flow-limiting dissections, laying the best foundation for the subsequent efficacy of drug-coated balloons.

Expert Introduction


Professor Zhang Lei
Director of Interventional Vascular Surgery
Director of the Department of Vascular Surgery, First Hospital of Hebei Medical University, Chief Physician, and Master's Graduate Supervisor.
Vice Chairman of Hebei Vascular Health and Technology Association;Chairman of the Hemorrhagic Emergency Committee, Hebei Vascular Health and Technology Association;Vice Chairman of the Hebei Province Vascular Surgery Branch of the Chinese Medical Association;Vice Chairman of the Hebei Province Vascular Surgery Branch of the Chinese Medical Doctor Association;Vice Chairman of the Emergency Hemorrhage Committee, Vascular Surgery Branch, Asia-Pacific Vascular Union;Vice Chairman of the Thrombosis Prevention and Control Committee of the Vascular Surgery Branch of the Chinese Society of Microcirculation;Editorial Board Member of "Vascular and Endovascular Surgery".
Began working in vascular surgery in 1997 under the guidance of Academician Zhonggao Wang, one of the founding figures of vascular surgery in China. During his career in vascular surgery, he has visited and studied at several renowned domestic and international institutions specializing in vascular diseases, including the Vascular Intervention Department at Garten Hospital, Leipzig University in Germany, the Cardiothoracic Surgery Department at Taipei Veterans General Hospital, and Beijing Anzhen Hospital. He is proficient in various vascular surgical procedures and endovascular treatment techniques. He was the first to introduce multiple pioneering technologies in Hebei Province, such as interventional treatment for iliac vein disease, endovascular treatment for aortic lesions involving critical branches, and interventional treatment for chronic thromboembolic pulmonary hypertension.

Professor Zhang Hongsong
The Surgeon of This Case
The First Hospital of Hebei Medical University, Department of Vascular Surgery, Associate Chief Physician, Master of Medicine;Vice Chairman of the Chronic Wound Management Professional Committee of the Hebei Vascular Health and Technology Association;Vice Chairman of the Atherosclerosis Professional Committee of Hebei Province Vascular Health and Technology Association;Standing Committee Member of the Diabetic Foot Professional Committee of Hebei Province Vascular Health and Technology Association;Secretary of the Varicose Vein Prevention and Treatment Committee, Hebei Vascular Health and Technology Association;Young Member of the Vascular Access and Interventional Nephrology Professional Committee.

Department Introduction

The Vascular Surgery Department of the First Hospital of Hebei Medical University is the Peripheral Vascular Disease Research and Treatment Center of Hebei Province. Approved by the Hebei Provincial Health Department in 1998, it is the only medical professional center in the province that relies on university advantages to specialize in the diagnosis, treatment, and research of peripheral vascular diseases. It is also a key medical specialty in Hebei Province and the main committee unit of the Hebei Vascular Health and Technology Association. Currently, it can perform advanced surgeries such as complex aortic dissection composite surgery, endovascular treatment and vascular replacement for abdominal aortic aneurysms, carotid endarterectomy, various vascular bypasses, plantar artery arch revascularization, and transjugular intrahepatic portosystemic shunt. Among these, the annual number of surgeries for aortic diseases reaches 200 cases, ranking at the forefront in the province.
Our department has more than 30 medical staff, including 3 with senior professional titles, 7 with associate senior professional titles, and 8 doctoral students. The department has 46 beds, with an annual outpatient and emergency volume reaching over ten thousand people, admitting 3,000 inpatients annually, performing 2,000 interventional surgeries, and conducting 600 open and hybrid surgeries. It is also a "Demonstration Base for Stroke Screening and Prevention" certified by the National Health Commission.
Copyright Statement: This platform aims to help medical and health professionals better understand the latest developments in related disease areas. The information content published on this platform does not imply agreement with its descriptions or viewpoints, but is merely for providing more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will handle it as soon as possible. This information is intended solely for medical and health professionals to stay informed. Such information cannot replace professional medical guidance in any way and should not be regarded as medical advice. If such information is used for purposes other than staying informed, this platform and the author shall not bear any related responsibility.Contact email for cooperation:vascular@edoctor.work。



