Monteris Medical Files for IPO: Pioneering Minimally Invasive Brain Tumor Therapy with Over $143M Raised and 3,000+ Patients Treated

Monteris Medical
Minimally Invasive Brain Injury Treatment Device Developer
Birchview Fund
An American Investment Firm

Versant Ventures
Healthcare Investment Institutions

SightLine Partners
Venture Capital Firms

The Vertical Group
Venture Capital Firm

Oxford Finance LLC
Financial Company

BDC Healthcare Venture Fund
Venture Capital Firms

BDC Venture Capital
Venture Capital Firms Focused on Canadian Technology Companies
“Almost every emerging technology must undergo a trial by fire at some stage in its maturation process; only by enduring it can you truly enter the core of science and technology.”
This was the response given by Marty Emerson, current CEO of Monteris Medical, in a media interview during his first month in office, when he encountered the first FDA Class I recall in his 30-year career in the medical technology field.
Monteris Medical was established in 1999, with its headquarters in Plymouth, Minnesota, USA, and has branches in Minneapolis, USA, and Winnipeg, Canada.Monteris Medical is dedicated to the development of neurosurgical technologies, focusing on providing treatments for conditions such as brain injuries and brain tumors through its minimally invasive laser ablation system, the NeuroBlate System, offering alternatives to traditional methods.
Most major brain disorders originate from pathological changes in brain functional networks, yet effective treatments are largely lacking. The key reason lies in the significant difficulty in detecting human brain functional networks and disease-related neural circuits, which severely hinders the understanding of the mechanisms underlying brain diseases.
To date, neuroscience has garnered the most Nobel Prizes in research on human life; however, the intricate connections between the brain—an organ composed of hundreds of billions of neurons—and the rest of the human body remain not fully understood.
According to relevant statistical data,Globally, approximately 1 billion people currently suffer from brain disorders, such as Alzheimer’s disease, stroke, Parkinson’s disease, epilepsy, and autism spectrum disorder in children. Patients with brain disorders account for about 11% of all disease cases worldwide, while the societal burden approaches 30% of the total global burden of disease.
Among them, according to the report from the Central Brain Tumor Registry of the United States (CBTRUS),Each year, more than 300,000 people in the United States are diagnosed with brain tumors and lesions.
Gliomas are highly prevalent primary malignant brain tumors in adults. Despite extensive research over the past 50 years, patient survival rates remain poor.
Among these, glioblastoma is the most common primary brain tumor, but current post-treatment survival rates for patients remain low. At present, surgery is typically the preferred initial treatment.
Although further tumor resection may offer survival benefits, potential surgical risks—such as neurological deficits and wound healing complications—must also be weighed. Therefore, minimally invasive surgical approaches have become a clinical priority and a preferred therapeutic option.
The treatment of brain tumors has also continuously evolved with the development of modern science and technology. The advent of CT and MRI has made the diagnosis of brain tumors more accurate, surgical navigation systems have refined intraoperative tumor localization, and Gamma Knife and stereotactic radiotherapy have pioneered a new treatment paradigm for patients with brain tumors.However, there is still no satisfactory treatment for patients with brain tumors that are deeply located, small in size, adjacent to functional brain areas, and in poor general condition.
Advances in Modern Cutting-Edge Technologies Bring New Developments to the Diagnosis and Treatment of Intracranial Tumors, Providing Diverse Therapeutic Options for Patients with Brain Tumors.
Laser Interstitial Thermal Therapy (LITT) has been used in clinical practice for several decades; however, due to the early lack of non-invasive temperature monitoring mechanisms and precise, effective heating methods, it has not been widely adopted in neurosurgery.
In recent years, advances such as the development of magnetic resonance thermometry, enhanced laser control, and real-time visualization of temperature changes in both pathological and normal tissues have expanded the applicability of Laser Interstitial Thermal Therapy (LITT), leading to its broader adoption in neurosurgery.
Laser interstitial thermal therapy (LITT), first proposed in 1983, is a stereotactic-guided percutaneous minimally invasive procedure in which laser energy is delivered via optical fibers to the target site for selective ablation of pathological tissue.The distinguishing feature of this large-scale technology is its ability to achieve precise ablation therapy for deep brain lesions under real-time MRI guidance and monitoring.
This is a novel technology that integrates image-guided stereotactic navigation with microcatheter-based laser thermal therapy, offering the advantages of precise laser targeting and controllable temperature."In recent years, an increasing body of clinical evidence has demonstrated that laser interstitial thermal therapy (LITT) is an effective minimally invasive approach for treating intracranial lesions. With its advantages of safety and repeatability, LITT represents a rational treatment option for tumors or epileptic foci that are small in volume, deeply located, or adjacent to eloquent brain regions."
Regarding the mechanism of action of LITT technology, Professor James T. Rutka, a member of the INC International Neurosurgery Consultants, Editor-in-Chief of the prestigious neurosurgical journal Journal of Neurosurgery, Chief of Surgery at SickKids (The Hospital for Sick Children) in Toronto, Canada, and Chair of the Brain Tumor Research Center, pointed out that laser interstitial thermal therapy utilizes magnetic resonance imaging (MRI) guidance. With the aid of MRI, neurosurgeons can clearly identify the spatial relationship between the tumor and the surrounding healthy brain tissue, thereby formulating a precise surgical trajectory.
The surgical procedure begins with making a small incision approximately 2–4 mm wide in the skin over the affected area. A laser fiber optic probe is then inserted through the incision and guided to the target lesion. Finally, pulsed laser energy is used to ablate or destroy the tumor tissue.
LITT Offers Five Advantages in the Treatment of Intracranial Tumors:First, MRI technology provides real-time guidance throughout the procedure, enabling precise localization of lesions and avoiding damage to surrounding healthy tissues.Generally, brain tumors smaller than 3 cm can be treated with a single session; for lesions with a diameter of 3 cm or greater, the entire brain tumor can be ablated via multiple trajectories.
Second, it is minimally invasive with few complications. The surgical incision is small, with the scalp incision measuring less than 4 mm, and the procedure can be performed via burr hole puncture of the skull.Offers a new treatment option for patients who cannot tolerate craniotomy.
Third, the procedure is short and recovery is rapid. The average duration of laser interstitial thermal therapy (LITT) for primary intracranial tumors is 2.9 hours, with most patients able to return home the day after treatment and quickly resume normal activities.Patients undergoing conventional surgical treatment require a hospital stay of 5–6 days, followed by several weeks of recovery.
In a retrospective analysis, patients who underwent MRI-guided LITT for gliomas, recurrent metastases, radiation necrosis, and epilepsy between 2010 and 2014 had an average hospital stay of 1.8–3.6 days.The average length of hospital stay typically depends on the severity of postoperative complications and edema, with many patients being discharged the following day.
Fourth, safety: no tissue damage caused by radiotherapy., can help patients who are unresponsive to stereotactic radiosurgery or have radiation necrosis (tissue death caused by radiation therapy).
5. Wide applicability.Metastatic tumors with focal recurrence after radiotherapy, deeply located malignant gliomas, recurrent focal gliomas, radiation necrosis, and inoperable recurrent meningiomas are all indications for LITT. It enables repeated, multi-directional treatment of intracranial tumors that are difficult to manage, such as recurrent glioblastoma.
An increasing body of relevant research has demonstrated that, compared with traditional open craniotomy, laser interstitial thermal therapy (LITT) is considered a minimally invasive technique. It has shown promising results in the treatment of small, recurrent, or deep-seated lesions, such as gliomas, brain metastases, radiation necrosis, and epilepsy. LITT offers a safer therapeutic alternative for patients whose lesions are surgically inaccessible, who are not candidates for surgery, or for whom other standard treatments have failed.
However, the consumables required for LITT are extremely expensive, and currently, only two companies in the United States and Canada can provide equipment related to LITT technology. One of them is Monteris Medical.
Monteris Medical’s NeuroBlate system is well-established; since receiving U.S. FDA approval in 2013, it has been used in over 3,000 patient procedures across the United States and Canada.
NeuroBlate provides patients with precise ablation of brain lesions without the need for open neurosurgery, while minimizing damage to surrounding healthy tissue during the procedure.
Monteris offers a comprehensive, end-to-end laser ablation system solution, including disposable components, hardware, Fusion™ software, and TruTemp™ technology.
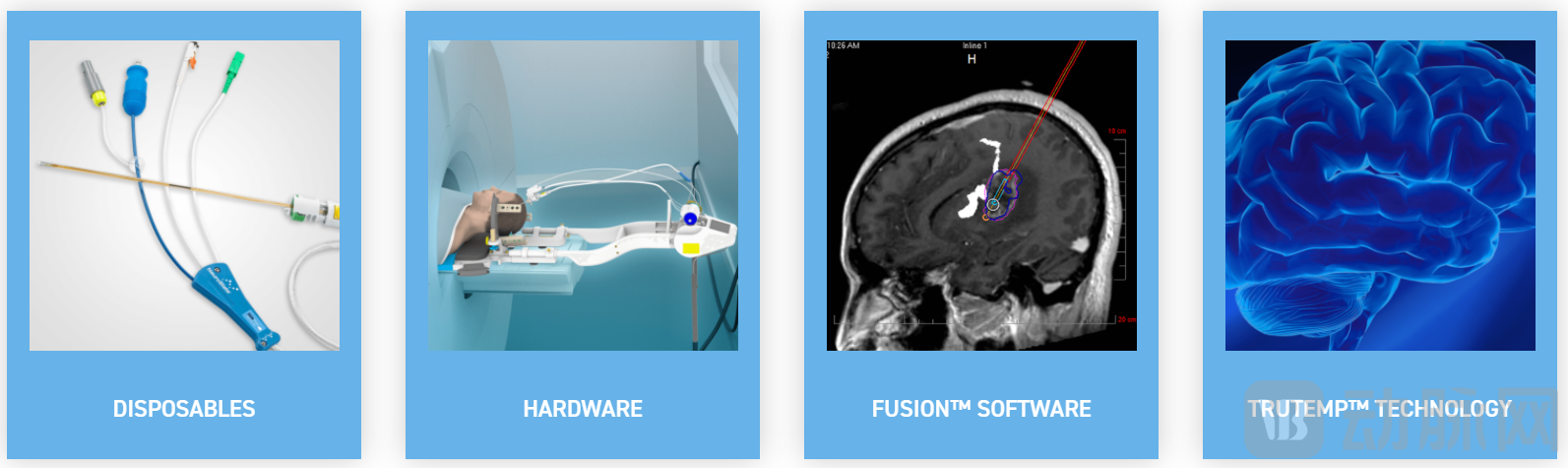
NeuroBlate System (Image source: Monteris official website)
The NeuroBlate system hardware includes a desktop monitor, an electronic rack, and a robot interface, which can be used with AtamA.®Patient board and head fixation. The AtamA System is used for patient transport and head immobilization.
Disposable items include the NeuroBlate Optic laser probe,According to Monteris, this is the first and only commercially available laser probe with fiber-optic controlled cooling, enabling single or multiple sequential trajectories using just one probe.Compared with other laser ablation surgery options for the brain, the unique use of a single probe multiple times during the procedure also avoids additional surgical costs.
In addition, it includes the NeuroBlate Robotic Probe Driver and the Monteris Mini-Bolt. The Mini-Bolt interfaces directly with the Robotic Probe Driver to enable precise laser probe control and laser delivery.
The NeuroBlate Fusion software regulates carbon dioxide within the probe to maintain the temperature at the probe tip. TruTemp™ technology is used to provide precise thermal imaging and enhanced visualization.
Currently, Laser Interstitial Thermal Therapy (LITT) is being increasingly and maturely applied at some of the world’s renowned neurosurgical research institutions, such as the world-famous University of California, San Francisco (UCSF) Medical Center, the International Neuroscience Institute (INI) in Germany, Lariboisière Hospital in Paris, France, and SickKids (The Hospital for Sick Children) at the University of Toronto in Canada, which is one of the world’s leading children’s hospitals.
SickKids Hospital is among the first children’s hospitals to be equipped with a complete LITT technology suite, utilizing the Monteris NeuroBlate® System.
In 2016, less than a month after Marty Emerson assumed the role of CEO, a problem report emerged from Minnesota indicating that Monteris Medical’s NeuroBlate robotic-assisted neurosurgical device had experienced unexpected heating during magnetic resonance imaging (MRI)-guided procedures.
This issue ultimately led to the U.S. Food and Drug Administration (FDA) classifying the Monteris Medical product as a Class I recall. This marked the first recall in Emerson’s 30-year history in the medical technology sector. Resolving and understanding this problem consumed the time and energy of Emerson and dozens of Monteris Medical employees over the following two years.
The team quickly determined that the issue lay with a coated metal thermocouple within the device. This thermocouple, which helps measure the temperature inside the probe, sometimes positioned the connector from the rear of the probe to the system too close to the inner wall of the MRI magnet, causing it to absorb energy transmitted down the probe and heat the probe tip.
Moreover, this issue occurred only in specific MRI systems running particular scan types, prompting the Monteris Medical team to ultimately test more than 20 configurations and combinations of equipment from companies such as Philips, Siemens, and General Electric to determine the MRI scan types compatible with NeuroBlate.
However, they were constrained by the fact that the MRI scan types available were not what the Monteris team desired. Over those two years, the Monteris team worked diligently to overcome the limitations of MRI scanning. As Marty Emerson stated, “Almost every emerging technology must undergo a trial by fire at some stage in its maturation process; only by enduring this can it truly enter the core of science and technology.”
In October 2018, Monteris Medical received FDA approval for the fiber-optic, actively cooled laser probe used in its NeuroBlate system. The fiber-optic component replaces the metal thermocouples previously housed within the laser probe, thereby eliminating MRI scanning restrictions for the NeuroBlate system. Currently, all patient-contacting components of the device are non-metallic.
The following year, Monteris secured nearly $11 million in Series D financing and obtained insurance coverage from Aetna and Anthem by the end of 2018.
It must be said that the calm and rational leadership was one of the reasons why Monteris was able to withstand the test. After leaving his top position at Galil Medical, Emerson joined Monteris. Previously, he led an interventional oncology cryoablation technology company, which was acquired by BTG, headquartered in London, for $110 million in 2016.
After graduating from Emerson University in 1985, he joined Baxter International in a finance role. In the late 1990s, he served as General Manager of Boston Scientific’s Singapore branch, marking his first foray into management.
Later, Emerson became an executive at American Medical Systems (AMS). AMS’s male urology portfolio is now part of Boston Scientific, while its women’s health portfolio is now part of Astora Women’s Health.
Although his sales background and communication skills were the reasons he initially joined AMS,However, Doug Krosch, the CEO at the time, stated in a media interview that Emerson’s calm demeanor and data-driven approach quickly made him stand out within the team.
Following the issue report, Emerson immediately led its team to dedicate full efforts to resolving the problem. In response to external skepticism, Emerson also proactively issued statements.
Throughout this process, Emerson’s top priority has been maintaining communication and transparency with the Monteris team, the FDA, and physicians.
When facing the media, Emerson recalled several instances of late-night sessions where executives and regulatory experts jointly edited responses to the FDA. As a trained accountant, he made a concerted effort to recognize the limits of his knowledge.
“I am not an FDA expert,” Emerson stated. “I rely heavily on the scientists, technicians, engineers, and specialists in my team to help us navigate this process.”
Following the crisis, Monteris Medical continued to grow. In 2020, Blue Cross and Blue Shield of North Carolina (BCBSNC), a health insurance provider, expanded coverage for Monteris Medical’s NeuroBlate System.
Emerson believes that Monteris, which saw a 40% increase in annual revenue to approximately $10 million before 2018, will experience renewed growth as it shifts its business focus to sales and marketing.
Since its establishment in 1999, Monteris Medical has completed 17 rounds of financing, totaling $143 million, according to data from Crunchbase and VCBeat.

Its major investors include SightLine Partners, Versant Ventures, Birchview Fund, BDC Venture Capital, Oxford Finance Corporation, The Vertical Group, and BDC Healthcare Venture.