Technical Bottlenecks and Innovative Solutions in rAAV-Based Gene Therapy for Ocular Diseases: Insights from Recent IND Filings
In July 2021, U.S. gene therapy company Adverum Biotechnologies Inc. (NASDAQ: ADVM, “Adverum”) suspended its Phase II clinical trial of the AAV gene therapy drug ADVM-022 for the treatment of diabetic macular edema (DME) after a participant experienced serious adverse events—including hypotony, inflammation, and vision loss—30 weeks following a single high-dose administration, raising industry concerns about the drug’s safety.
ADVM-022 is a gene therapy utilizing Adverum’s proprietary AAV2.7m8 capsid. Administered via a single intravitreal (IVT) injection, this therapy is designed to enable sustained production of therapeutic agents by retinal cells, thereby providing long-term therapeutic and prophylactic efficacy. It aims to alleviate the burden of frequent anti-VEGF antibody injections and ultimately improve patients’ vision.
Despite facing clinical safety challenges, gene therapy still offers unparalleled therapeutic advantages, particularly for monogenic inherited diseases that lack alternative treatments. By fundamentally supplementing or repairing defective genes and restoring the normal biological function of healthy genes, this approach can minimize or even eliminate lifelong symptoms in patients.
Over the past five years, clinical trials of ocular gene therapies have increased rapidly, targeting a variety of rare hereditary retinal diseases and genetically mediated corneal disorders, such as choroideremia, Leber hereditary optic neuropathy, Stargardt disease, X-linked retinoschisis, and X-linked retinitis pigmentosa. Even more promising is the hope that gene therapy brings to hundreds of millions of patients suffering from common eye diseases such as age-related macular degeneration (AMD). Conventional anti-VEGF antibody therapy requires long-term, frequent, and regular intravitreal injections, which significantly reduce patient adherence and increase treatment risks. Gene therapy is emerging as an effective alternative treatment option.
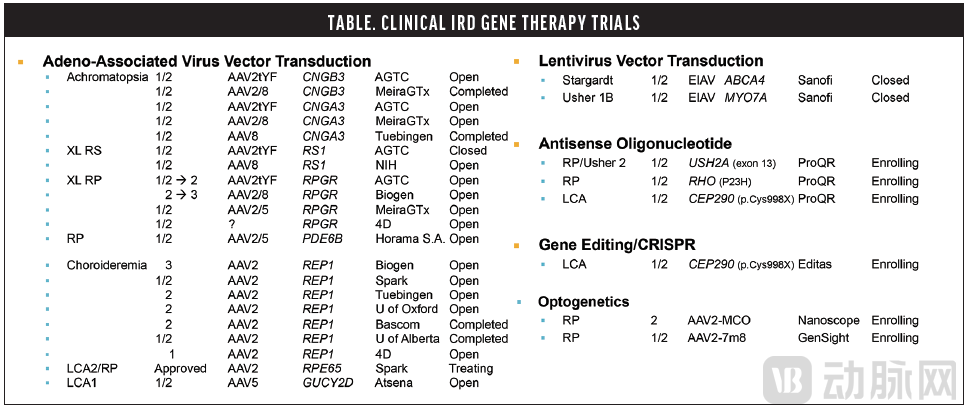
Ongoing Clinical Trials of Gene Therapy for Inherited Retinal Diseases (Partial). Image source: Paul Yang, AAO 2020
In gene therapy, viral vector technology is currently the primary method for gene delivery, and advances in this technology have largely driven the development of the gene therapy field. Over the past two decades, adeno-associated virus (AAV) vectors have sparked a clinical surge in this area.
Adeno-associated virus (AAV) is a small, non-enveloped parvovirus that offers numerous advantages as a delivery system, including non-pathogenicity, efficient and sustained expression, ease of manipulation, and low immunogenicity. After the therapeutic gene (gene of interest, GOI) carried by AAV vectors enters cells, it is transcribed and translated into functional proteins, thereby achieving the treatment of a range of diseases.
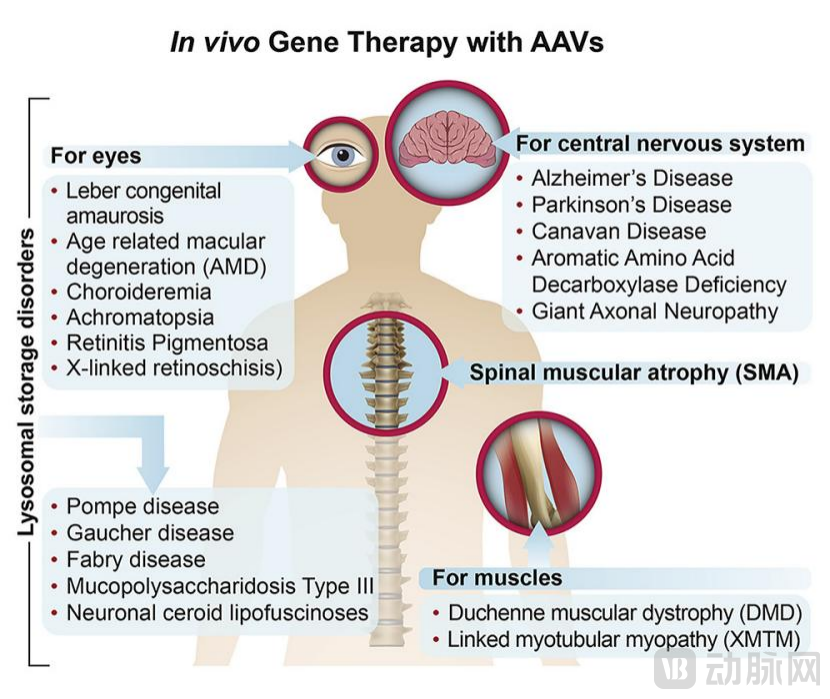
A series of diseases treated with AAV-based gene therapy. Image source: Reference 1
rAAV is the primary vector for ocular gene therapy. In therapeutic gene delivery, the DNA sequences encoding regulatory proteins (Rep) and structural proteins (Cap) within the adeno-associated virus (AAV) single-stranded DNA (ssDNA) genome are replaced by the desired gene of interest (GOI) expression cassette, resulting in what is known as recombinant AAV (rAAV). The AAV capsid facilitates GOI targeting to specific tissues. To date, 12 distinct AAV serotypes have been identified in primates; these serotypes differ in their capsid components and exhibit varying tropism, transduction efficiency, and immunogenicity. AAV serotypes 1, 2, 4, 5, 6, 7, 8, and 9 all demonstrate tropism for retinal tissue.
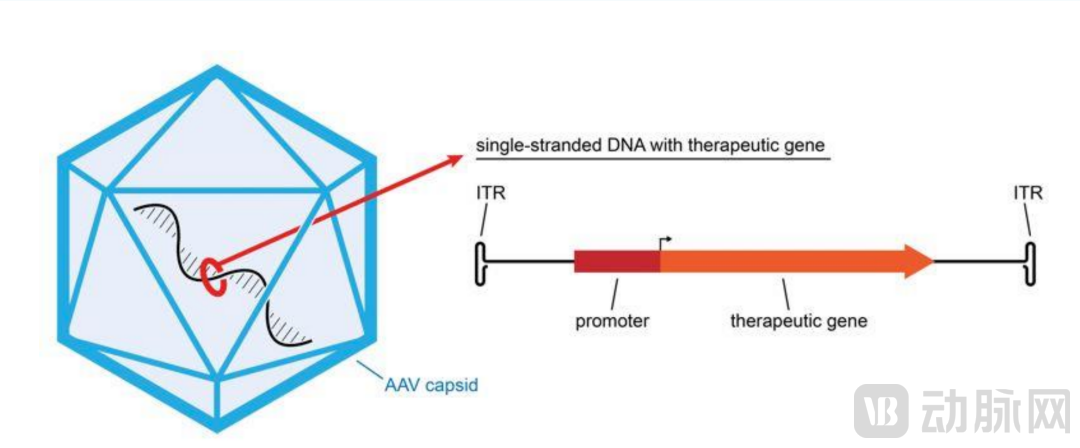
Schematic diagram of the structure of AAV therapeutic vectors. Image source: catapult.org.uk
Gene therapy offers significant advantages in the treatment of ocular diseases, a benefit determined by the genetic basis of these conditions and the unique characteristics of the ocular compartment.
Due to the well-defined anatomical structure of the eye and its confined physical space, local drug delivery offers unique advantages. The blood-ocular barrier contributes to ocular immune privilege, resulting in limited immune responses to gene therapy products. Furthermore, retinal cells are post-mitotic, allowing for sustained gene expression without genomic integration. Most importantly, the potential genetic factors underlying a range of ocular diseases, including hereditary blindness, have been identified. In addition, recent development of relevant animal models has facilitated significant advances in ophthalmic research, thereby supporting the conduct of ocular gene therapy trials.
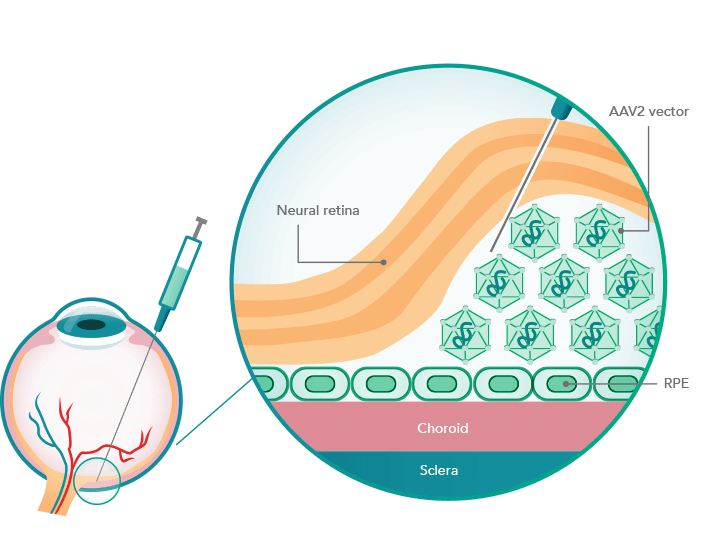
The AAV2 viral vector delivers the therapeutic gene to the eye via subretinal injection. Image source: https://luxturnahcp.com/
Spark Therapeutics’ Luxturna® (voretigene neparvovec-rzyl) is the first approved gene therapy product for the treatment of a rare ocular disorder. Luxturna delivers a functional copy of the RPE65 gene to retinal pigment epithelial (RPE) cells, treating Leber congenital amaurosis type 2 (LCA2) caused by biallelic RPE65 mutations.
The approval of Luxturna marks a significant milestone in the development of gene therapy for ocular diseases. The success of this project validates the feasibility of the gene therapy concept and confirms its substantial value in restoring or preserving vision.
rAAV products have demonstrated broad application prospects as gene therapy drugs, with over 200 rAAV-based clinical trials currently underway worldwide. However, the clinical outcomes of many investigational projects have not been as consistently translated as those observed in patients with LCA2.
In fact, as a complex biologic composed of the viral genome and multiple structural proteins, recombinant adeno-associated virus (rAAV) products face numerous technical challenges in both upstream development and downstream manufacturing. A key issue to be addressed is how to ensure the functional potency of rAAV while reducing the clinical dosage. Therefore, in addition to optimizing production and purification processes, it is equally important to engineer and modify AAV vectors to enhance their affinity for target cells and improve the efficacy of the gene of interest (GOI).
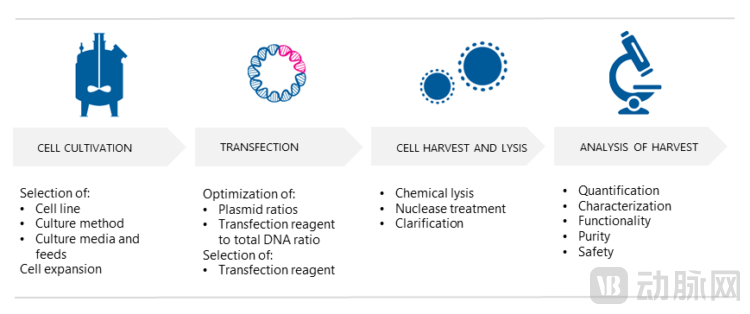
Upstream Manufacturing Process of AAV Products
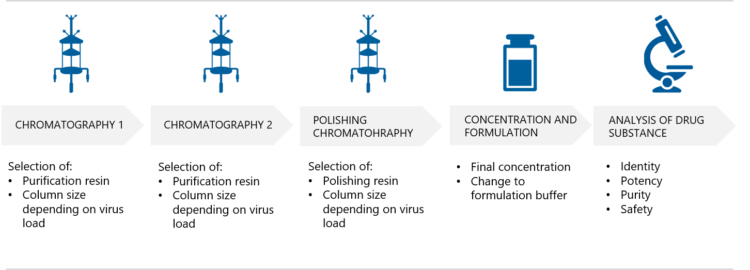
Downstream Manufacturing Process of AAV Products. Image source: biovian.com
When the targeting and transduction capabilities of the vector used are limited, it becomes necessary to increase the dosage to achieve the desired clinical effect. However, high doses of virus-like products also mean more impurities are mixed in, increasing the risk of triggering immune responses. At the same time, achieving balanced transduction with high-dose drugs is challenging, and controlling the level of transgene expression across different cell types is difficult.
To enhance vector targeting and transduction efficiency in specific cell types, engineering the AAV capsid has emerged as a key area for optimizing delivery vectors. Capsid quality and retinal tropism are critical features of AAV products for achieving safe and effective ocular gene therapy. AAV capsids can be derived from natural isolates or engineered through rational design, directed evolution, or computer-aided techniques. Professor David Schaffer at UC Berkeley is a pioneer in “directed evolution”; his laboratory developed the novel retinal-tropic AAV2.7m8 vector, which is currently used in Adverum’s ADVM-022. He is also the scientific founder of 4DMT, a company that employs directed evolution to discover novel AAV vectors and has established gene therapy pipelines across multiple disease areas, including ophthalmology, cardiovascular diseases, and respiratory disorders.
Notably, AAV capsid engineering technology is also a key R&D focus of Avirmax, a company co-founded by Chinese scientists Shengjiang Liu and Haifeng Chen. According to the company’s official website, Avirmax possesses unique AAV capsid engineering technology that enables its developed recombinant adeno-associated virus (rAAV) vectors to bind more strongly to receptors and penetrate the inner limiting membrane (ILM). This allows for highly efficient delivery of the gene of interest (GOI) into retinal cells, achieving concentrations hundreds to thousands of times higher than those attained with wild-type AAV capsids. Avirmax’s rAAV products can be used to treat common retinal diseases, such as wet age-related macular degeneration (wAMD), diabetic macular edema (DME), and polypoidal choroidal vasculopathy (PCV), as well as more than ten rare retinal diseases. The figure below shows a computer simulation of one of Avirmax’s engineered AAV capsids.

Engineered AAV-VP1 Capsid Protein
To enhance rAAV efficacy, techniques such as genetic engineering and optimization can be employed to boost the expression levels of the gene of interest (GOI) in AAV vectors, thereby reducing the required drug dosage. Avirmax is utilizing such transgene expression-enhancement technologies, with their data demonstrating that this approach can significantly increase GOI expression in AAV therapeutic vectors (by 10-fold).
Another challenge facing AAV gene therapy products is achieving scalable and cost-effective production of impurity-free vectors.
Capsid components, vector genomes, transgene products, or contaminating impurities in AAV products have the potential to activate host immune responses, leading to treatment failure or uncontrolled inflammation. Even though AAV vectors possess relative immune privilege, they can still elicit cellular responses in the subretinal space. Therefore, manufacturers of AAV products must improve production technologies, enhance product purification, and implement stringent quality control to ensure low immunogenicity of their products.
An ideal AAV production system must ensure sufficient viral titers while minimizing harmful contaminants, removing empty capsids or vectors with incorrect DNA packaging, thereby reducing clinical risks as much as possible. However, there is currently no technology available to remove incorrectly packaged DNA from vector products; moreover, eliminating empty capsids from the product during large-scale manufacturing remains a significant challenge.
In fact, large-scale manufacturing of AAV products is a critical step in meeting clinical demand and reducing product costs. Based on current production systems, the baculovirus expression platform employed by Avirmax offers significant advantages over triple-transfection HEK293 systems or mammalian stable cell line production systems, making it a highly attractive strategy for large-scale, clinical-grade vector manufacturing.
This platform utilizes the insect (Spodoptera frugiperda) cell line Sf9 and co-infection with two baculovirus expression vectors: one baculovirus vector carries the gene of interest (GOI) and its promoter between the inverted terminal repeat (ITR) regions, while the other encodes the rep and cap genes. This system enables rapid production of high-quality, high-titer AAV products, reduces erroneous packaging of host cell DNA, provides reliable biosafety assurance, and facilitates scalable manufacturing.
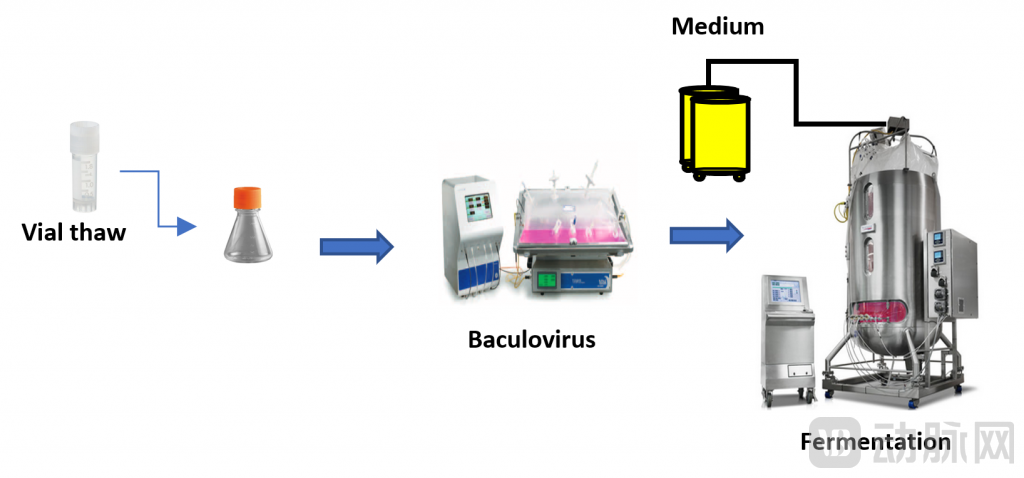
Avirmax’s Sf9-AAV Large-Scale Production Platform. Image source: Avirmax official website
Previous studies have shown that AAV experiments conducted in small animal models often yield biased results, such as transduction efficiency, when translated to large animal models. Moreover, effects observed in certain animal models are difficult to apply and reproduce in human clinical trials. Due to this unpredictability associated with novel AAV vectors, it is essential to conduct studies in large animal models, such as non-human primates (e.g., cynomolgus monkeys or rhesus macaques), before initiating clinical trials of AAV-based products. It is understood that Avirmax adheres to the strategy of employing large animal models at an early stage to validate the clinical translation success rate of its novel AAV vectors.
In addition to the selection of model species, researchers must also consider factors such as the age of the models, treatment modalities, and the duration of follow-up. By selecting more appropriate in vitro disease models that reliably simulate human physiological conditions, safer and more effective clinical dosage ranges can be determined.
Human serological studies have shown that due to prior exposure to wild-type AAV, the global population has a high prevalence of AAV neutralizing antibodies. Approximately 67% of individuals possess antibodies against AAV1, 72% against AAV2, and 40% against AAV serotypes 5 through 9. Consequently, screening for pre-existing immunity is required for participants in AAV gene therapy trials, potentially excluding more than 50% of patients. Furthermore, pre-existing immunity to the vector poses a major challenge to the re-administration of AAV products, a issue that is particularly prominent in in vivo gene therapy.
To provide more patients with access to treatment, one solution is to develop AAV capsids capable of “evading” neutralizing antibodies. Recently, an emerging approach has garnered attention, offering new insights into addressing this challenge. This method utilizes enzymes discovered in bacteria, specifically imlifidase, with IdeS and IdeZ currently under investigation. These enzymes can be administered prior to AAV product delivery to rapidly degrade pre-existing anti-AAV neutralizing antibodies in the bloodstream, thereby creating a temporary window of opportunity for AAV vectors to reach target cells.
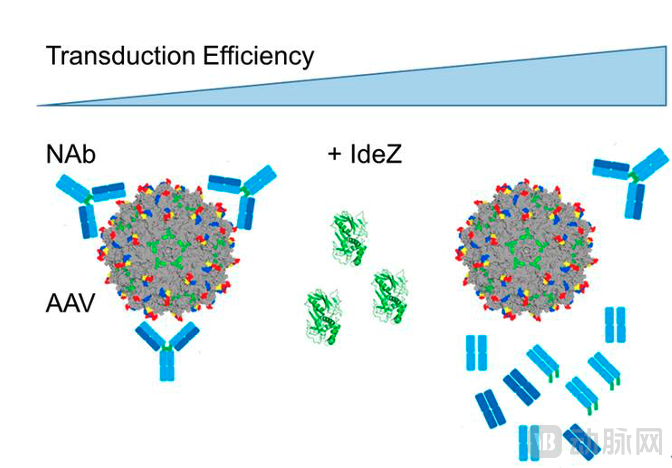
Enzymatic degradation of pre-existing AAV neutralizing antibodies to enhance transduction efficiency. Image source: Reference 9
In summary, the key to successful gene therapy lies in ensuring sufficient expression levels of the gene of interest (GOI) at doses that maintain controllable inflammation; otherwise, reduced or lost efficacy may occur, necessitating re-administration or causing local tissue damage, and even posing life-threatening risks.
The Potential of Gene Therapy Is Just Beginning to Emerge. As a novel therapeutic modality, AAV gene therapy remains in its early stages of development. Compared with other biologics that have accumulated substantial experience and knowledge, such as therapeutic antibodies and recombinant proteins, our understanding of the biological characteristics of AAV viral vectors still requires further deepening.
From the perspective of the current R&D market, an increasing number of companies are focusing on gene therapy for ocular diseases. However, we observe that many R&D projects are concentrated on accelerating pipeline advancement, with insufficient effort dedicated to addressing fundamental scientific issues. Even if some products advance into clinical stages, they may encounter various safety and efficacy challenges, leading to irreversible consequences.
To address this issue, in addition to strengthening the intensity and depth of foundational product R&D, it is equally important to continuously improve and follow up on clinical regulation, so as to clarify and standardize clinical expectations for gene therapy products.
● In April 2008, the FDA issued its first guidance on human gene therapy. In July of the same year, the FDA released a draft updated guidance document on human gene therapy, outlining its current regulatory perspectives;
● In January 2020, the FDA issued the guideline on gene therapy for retinal diseases, “Human Gene Therapy for Retinal Disorders”;
● On September 30, 2021, the FDA issued the “Draft Guidance for Industry: Studying Multiple Versions of a Cellular or Gene Therapy Product in an Early-Phase Clinical Trial” (see Reference 10 for details). In this latest guidance, the FDA innovatively proposed that multiple different versions of cellular and gene therapy products may be included under a single Investigational New Drug (IND) application for a specific disease. It also provided several recommendations for assessing the preliminary safety and biological activity of such clinical studies, including how to organize and structure the IND, submit new information, and report adverse events (AEs). The draft is currently open for industry feedback. Once finalized, this new guidance is expected to significantly enhance the speed and efficiency of early-stage development of cellular and gene therapy products.
Although AAV gene therapy still faces many challenges and limitations, existing clinical data indicate that it remains a safe, well-tolerated, and effective approach. For instance, in the ADVM-022 trial for treating diabetic macular edema (DME) mentioned at the beginning of this article, high-dose toxicity was observed; however, no adverse events were reported in the low-dose cohort. Furthermore, another clinical trial of ADVM-022 for wet age-related macular degeneration (AMD) showed no similar adverse events in patients receiving either low or high doses, with follow-up periods ranging from 52 weeks to 2.5 years post-treatment.
Globally, rAAV accounts for 24% of all gene therapy products. Between 2015 and 2020, the FDA received 99 Investigational New Drug (IND) applications for rAAV-based gene therapies. With advancements in technology and the refinement of clinical regulatory frameworks, we anticipate that more gene therapy products will reach the market, benefiting a broader population of patients with common ocular diseases and providing long-lasting therapeutic benefits.
References:
1. Jerry R. Mendell, et al., Current Clinical Applications of In Vivo Gene Therapy with AAVs. Molecular Therapy(2021)29:464-488.
2. Allison M. Keeler and Terence R. Recombinant Adeno-Associated Virus Gene Therapy in Light of Luxturna (and Zolgensma and Glybera): Where Are We, and How Did We Get Here? Flotte Annual Review of Virology (2019) 6:601-621.
3. Kuzmin DA, et al., The clinical landscape for AAV gene therapies. Nat Rev Drug Discov (2021) 20:173-174.
4. Beginner’s guide to the production of AAV vectors for gene therapy–Mentored by a CDMO.https://biovian.com/beginners-guide-to-the-production-of-aav-vectors-for-gene-therapy-mentored-by-a-cdmo/
5. Mark White. Addressing the Top Five Challenges to AAV-Based Gene Therapy with ddPCR.https://www.genengnews.com/insights/addressing-the-top-five-challenges-to-aav-based-gene-therapy-with-ddpcr/
6. Christine Kay. AAV Gene Therapy Trials To Watch. July/August 2021. https://retinatoday.com/articles/2021-july-aug/aav-gene-therapy-trials-to-watch
7. Bulcha, J.T., Wang, Y., Ma, H. et al. Viral vector platforms within the gene therapy landscape. Sig Transduct Target Ther (2021) 6, 53.
8. Leborgne C, Barbon E, Alexander JM, et al. IgG-cleaving endopeptidase enables in vivo gene therapy in the presence of anti-AAV neutralizing antibodies. Nat Med. (2020) 26:1096-1101.
9. Zachary C. Elmore, Daniel K. Oh, et al.Rescuing AAV gene transfer from neutralizing antibodies with an IgG-degrading enzyme. JCI Insight. (2020) 5:e139881.
10. US Food and Drug Administration, HHS 【Docket FDA-2021-D-0776】 Studying Multiple Versions of a Cellular or Gene Therapy Product in an Early-Phase Clinical Trial:Draft Guidance for Industry, Availability.