Application of DEEPQUAKE Peripheral Lithotripsy System in a Case of Severely Calcified Arteriovenous Fistula Stenosis by Professor Liu Yangdong’s Team

Trulive
Structural Heart Disease Device Developer

In the field of pan-vascular intervention, the treatment of calcified lesions is one of the key and difficult points in clinical practice. Produced by Trulive and promoted by Grand Pharmaceutical Group Limited,DEEPQUAKE Peripheral Vascular Intravascular Shockwave SystemOfficially launched (China Medical Device Registration No. 20243012335).
Stenosis of arteriovenous fistulas associated with severe calcification represents a significant challenge in the maintenance of vascular access for maintenance hemodialysis. Conventional balloon angioplasty often faces limitations such as insufficient dilation and a relatively high risk of complications. Although intravascular lithotripsy has been widely used in the treatment of calcified lesions in coronary and peripheral arteries, its application in calcified stenosis of arteriovenous fistulas remains very limited, with only a few technical reports or case studies currently available.
This issue is shared with everyoneAn Application of DEEPQUAKE Peripheral Shock Wave System in the Treatment of Severe Calcified Arteriovenous Fistula Stenosis, by South China Hospital Affiliated to Shenzhen UniversityProfessor Liu Yangdong's TeamCompleted, welcome everyone to read, study, exchange, and discuss.
【Ref:Zhou A, Zi Y, Lu Y, Hu L, Wang C, He Y, Wen L, Liu Y. Application of intravascular lithotripsy in a case of severely calcified arteriovenous fistula stenosis: A case report and technical note. J Vasc Access. 2025 Dec 14:11297298251391723. doi: 10.1177/11297298251391723. Epub ahead of print. PMID: 41392402.】
Case Summary
Patient Basic Information
Diagnosis and Surgical Strategy
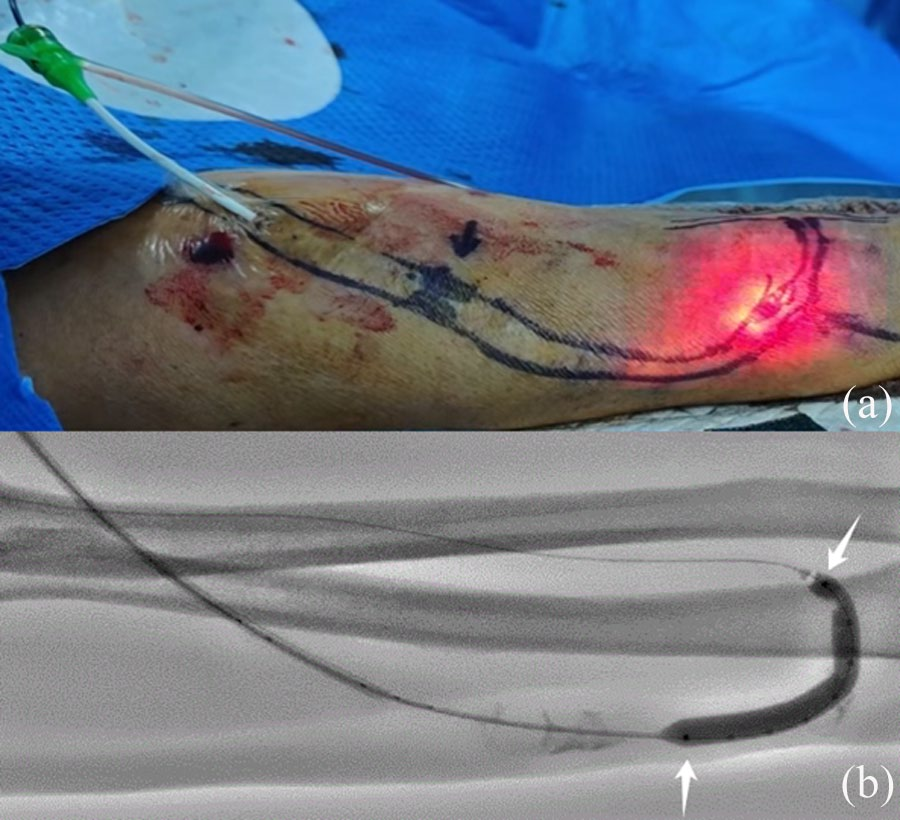
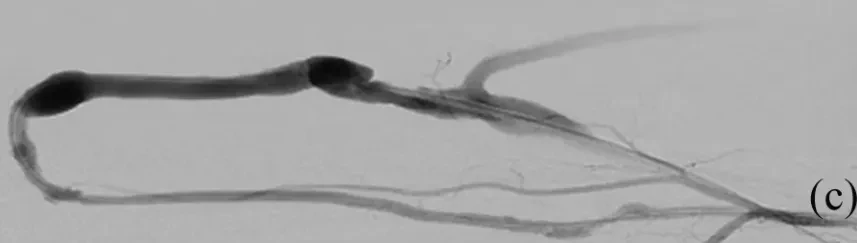
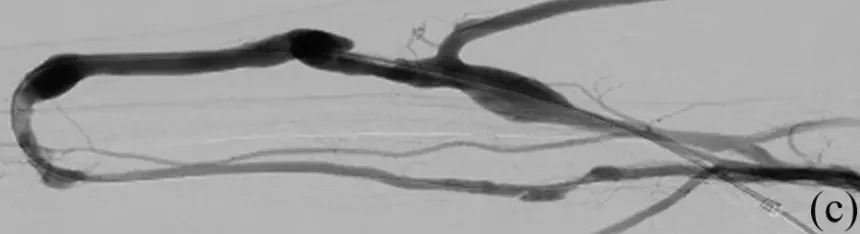
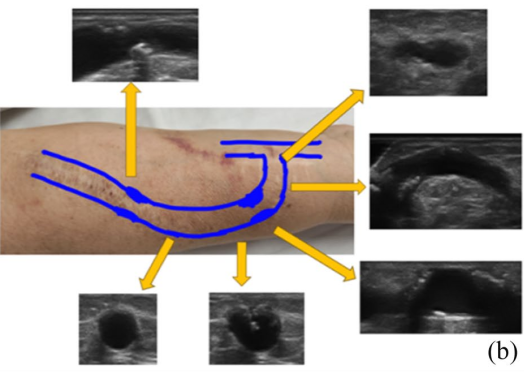
Surgical Procedure
Postoperative Follow-up
Technical Points
Surgeon's Evaluation
1. An Effective Breakthrough for the Limitations of Traditional Balloon Dilation
Traditional Percutaneous Transluminal Angioplasty in the treatment of circumferential calcified lesions often results in balloon drift towards the less calcified side due to uneven hardness between the calcified plaque and normal vessel wall, leading to eccentric dilation and the "watermelon seed effect." This not only makes it difficult to effectively disrupt the calcified plaque but also subjects the thinner non-calcified vessel wall to greater stress, increasing the risk of vascular rupture, dissection, or perforation. In this case, an intravascular lithotripsy balloon was used, which selectively targets high-density calcified structures through acoustic shock waves, generating shear stress to fragment the calcification and avoiding the aforementioned risks. No complications such as vascular rupture or dissection occurred during the procedure.
2. Improve patient comfort during surgery
During the traditional high-pressure balloon dilation process, patients often report severe pain due to the high dilation pressure endured under local anesthesia. In this case, the patient only experienced mild pain during the procedure, significantly less than the pain felt during previous percutaneous transluminal angioplasty treatments, suggesting that the shockwave balloon has advantages in improving the patient's treatment experience.
3. Safety Considerations in the Treatment of Arteriovenous Fistula Calcification
The venous position of the arteriovenous fistula is superficial, allowing for clear assessment of the balloon's position and working status during surgery through the light spots generated by balloon discharge and the radiopaque ring under fluoroscopy, offering a high degree of visualization. Additionally, the walls of mature fistula vessels are relatively thick with no vital organs nearby, which may provide higher operational safety compared to deeper vascular anatomical locations. Considering the limited efficacy of traditional balloons on long-segment circumferential calcified lesions, intravascular lithotripsy demonstrates good applicability in treating superficial fistula calcifications. During this procedure and the three-month follow-up period post-operation, no complications such as embolism or vessel rupture were observed, consistent with the low complication rate (1.25%) and rare significant embolic events reported in the literature for intravascular lithotripsy in lower limb arteries.
4. Limitations and Prospects
This case report describes the application of intravascular lithotripsy in a patient with severe circumferential calcification of an arteriovenous fistula, preliminarily indicating that the technique is safe and effective for treating such lesions. This provides a new therapeutic approach for clinically addressing this challenge. However, its long-term efficacy and applicability in larger samples still require further research and validation.
Expert Introduction

Professor Liu Yangdong
Ph.D., Postdoctoral Fellow, Chief Physician, Master's Supervisor.
Director of the Department of Interventional Vascular Surgery, South China Hospital, Shenzhen UniversityStanding Committee Member of the Endovascular Specialty Committee, Chinese Medical Doctor AssociationVice Chairman of the Hemodialysis Access Expert Committee, Endovascular Specialty Committee, Chinese Medical Doctor AssociationVice Chairman of the Vascular Access Expert Committee, Peripheral Vascular Disease Specialty Committee, Chinese Society of Integrated Traditional and Western MedicineVice Chairman of the Hemodialysis Access Expert Committee, Chinese Division of the International Union of Angiology (IUA)Vice Chairman of the Interventional Vascular Access Group, Integrated Traditional and Western Medicine Intervention Branch, China Health Information AssociationMember of the Vascular Access Group, Vascular Surgery Physician Branch, Chinese Medical Doctor AssociationMember of the Hemodialysis Access Group, Blood Purification Management Branch, Chinese Hospital AssociationStanding Committee Member of the Hemodialysis Access Group, Vascular Surgery Branch, China International Exchange and Promotion Association for Medical and HealthcareMember of the Vascular Medicine Specialty Committee, Chinese Research Hospital AssociationMember and Secretary of the Hemodialysis Vascular Access Group, Vascular Surgery Specialty Committee, Cross-Straits Medical and Health Exchange AssociationVice Chairman of the Peripheral Vascular Disease Branch, Guangdong Precision Medicine Application SocietyStanding Committee Member of the Vascular Surgery Branch, Guangdong Medical Association.
Features of DEEPQUAKE Peripheral Shock Wave System

Previous Recommendations
Copyright Statement: This platform aims to help healthcare professionals better understand the latest developments in relevant disease areas. The information published on this platform does not imply agreement with its descriptions or viewpoints; it is only intended to provide more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will address them as soon as possible. The information is solely for healthcare professionals to stay informed and should not replace professional medical guidance in any way, nor should it be considered as medical advice. If such information is used for purposes other than staying informed, this platform and the authors assume no responsibility.Contact Email for Cooperation:vascular@edoctor.work。



